Cornual Epithelioid Trophoblastic Tumor: A Report of a Rare Case and Literature Review
Nawal A Alharbi, Ghada I Abdulhamid, Salafa Albaghli, Ayman M Husain

TL;DR
This paper reports a rare case of a cornual epithelioid trophoblastic tumor and discusses its diagnosis and treatment challenges.
Contribution
The paper presents a rare case of ETT in a cornual ectopic pregnancy and emphasizes the importance of histopathology for diagnosis.
Findings
The patient had persistently elevated β-hCG levels despite initial methotrexate treatment.
Surgical resection followed by multi-agent chemotherapy normalized β-hCG levels.
Histopathological confirmation was crucial for diagnosing ETT.
Abstract
Cornual ectopic pregnancy is a rare type of ectopic pregnancy that occurs in the cornua of the uterus. This condition poses significant risks, including rupture and severe hemorrhage, making early diagnosis and management crucial. Gestational trophoblastic neoplasm (GTNS) is a spectrum of malignant diseases including invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT). ETT is a rare type of gestational trophoblastic tumor. While ETT shares some similarities with other trophoblastic tumors, it has distinct histological features, clinical behaviors, associations, and treatment approaches that set it apart. We present a rare case involving a 38-year-old Saudi woman diagnosed with a cornual ectopic pregnancy, which was later histopathologically confirmed as ETT. Initial treatment included systemic and local methotrexate,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
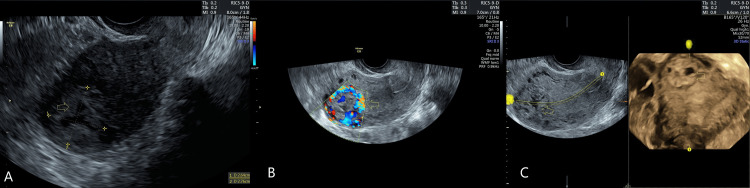 Figure 1
Figure 1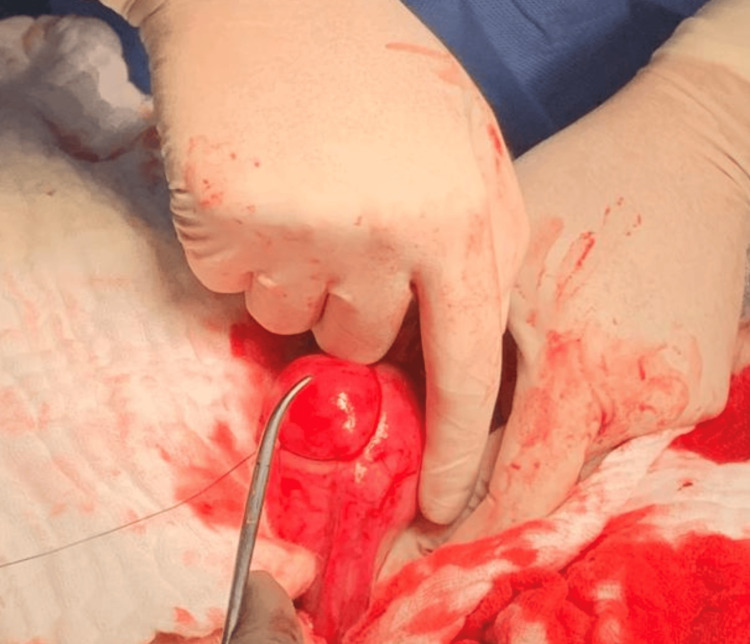 Figure 2
Figure 2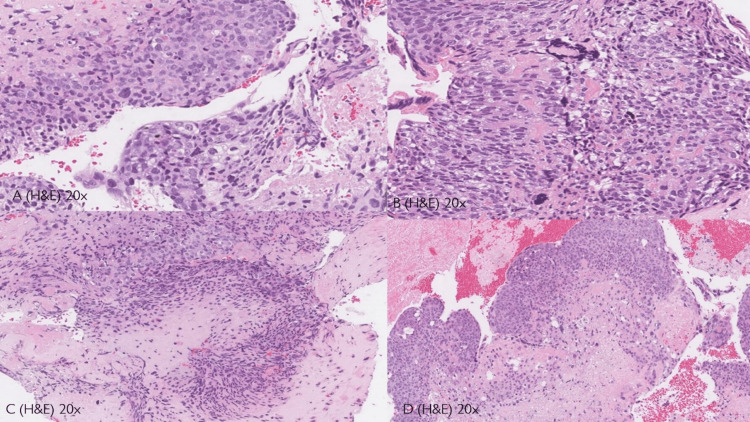 Figure 3
Figure 3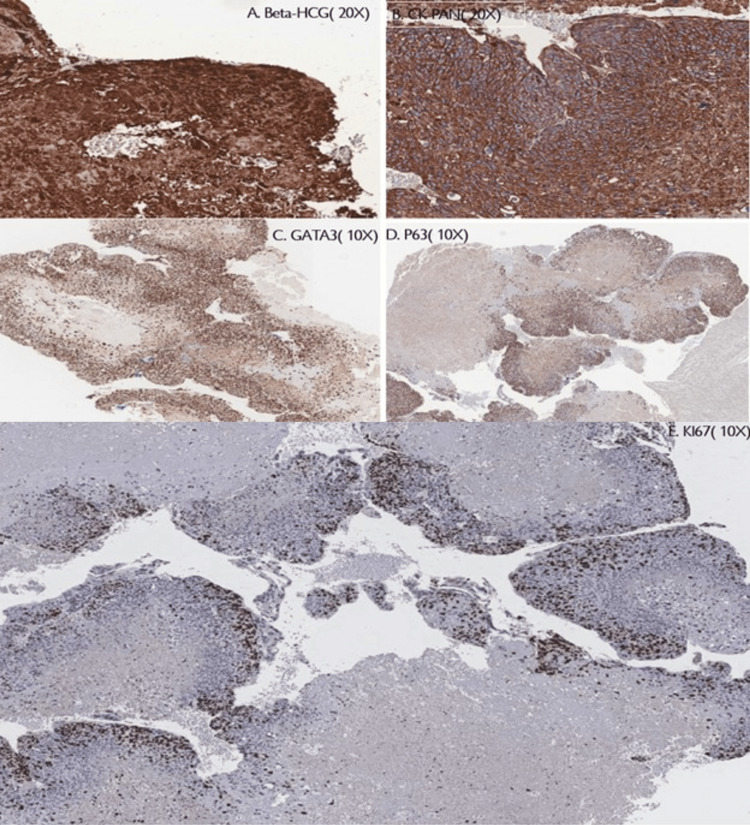 Figure 4
Figure 4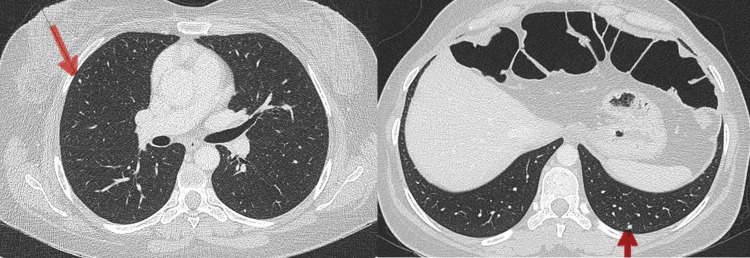 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Trophoblastic Disease Studies · Prenatal Screening and Diagnostics
Introduction
Cornual ectopic pregnancy is a rare and dangerous form of ectopic pregnancy, representing 2-4% of all ectopic cases [1]. It occurs at the uterine cornu, where the fallopian tube connects to the uterus. This type carries a high risk of rupture and severe hemorrhage due to the area’s abundant blood supply and thin myometrial wall.
Gestational trophoblastic neoplasms (GTNs) include a variety of malignant trophoblastic disorders such as invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT). ETT, a rare subtype, constitutes only 1-2% of all GTNs [2,3]. Initially referred to as “atypical choriocarcinoma,” ETT was officially classified by the World Health Organization (WHO) in 2003 [4,5]. Unlike choriocarcinoma, which arises from syncytiotrophoblasts and cytotrophoblasts, ETT originates from chorionic-type intermediate trophoblasts and displays distinct histopathological characteristics [5,6].
Typically, ETT occurs in the lower uterine segment or cervix, but it is infrequently found in the uterine cornua. Diagnosis remains challenging due to overlapping clinical features with other GTNs and ectopic pregnancies. This case report discusses an unusual manifestation of ETT that mimicked a cornual ectopic pregnancy, detailing its diagnosis and management.
Case presentation
A 38-year-old multiparous Saudi woman (G4P3) presented to the emergency department three months after childbirth, complaining of abdominal pain and irregular vaginal bleeding. Her obstetric history included two vaginal deliveries and a preterm cesarean section at 32 weeks due to placenta previa accompanied by antepartum hemorrhage.
Upon examination, the patient was hemodynamically stable. Laboratory results indicated a hemoglobin level of 12 g/dL and a significantly elevated serum beta-human chorionic gonadotropin (β-hCG) level of 24,000 mIU/mL. A transvaginal ultrasound revealed a 30 × 27 mm right cornual mass with peripheral vascularity, indicative of a gestational sac without an embryo. A diagnosis of cornual ectopic pregnancy was established (Figure 1).
Ultrasound images shows the cornual ectopic.(A) shows the cornual ectopic. (B) shows the increased vascularity of the mass. (C) shows the three-dimensional ultrasound of the mass.
Initial management
The patient received three doses of intramuscular methotrexate; however, her β-hCG levels showed only a suboptimal decline from 24,000 to 10,864 mIU/mL. A fourth dose of locally injected methotrexate into the suspected gestational sac led to a temporary drop in β-hCG to 3,759 mIU/mL, but levels subsequently rose again, reaching 6,708.83 mIU/mL, prompting the need for surgical intervention.
Surgical findings and histopathology
The patient underwent laparotomy with wedge resection of the cornual mass, followed by primary repair of the uterus (Figure 2).
Intraoperative finding (cornual ectopic pregnancy).Cornual ectopic pregnancy was managed with wedge resection.
Histopathological examination revealed monomorphic cells arranged in a nested pattern, eosinophilic cytoplasm, and extensive necrosis, consistent with ETT (Figure 3).
Histopathology analysis(A) Tumor cells have a moderate amount of finely granular, eosinophilic to clear cytoplasm with distinct cell membranes and round nuclei with small nucleoli. (B) Moderate nuclear atypia is seen in most of the tumors with occasional syncytiotrophoblastic. (C) Eosinophilic hyaline material is characteristically present in the center of some tumor nests. (D) Extensive or geographic necrosis
Immunohistochemical staining was positive for β-hCG, CK-Pan, GATA3, and p63, while negative for hPL, inhibin, SALL4, and PAX8 (Figure 4).
Immunohistochemical stain.The tumor cells are positive for β-hCG (A), CK-Pan (B), GATA3 (C), p63 (D) and negative for hPL, INHIBIN, SALL4, and PAX8. KI67 labeling index 10% (E).hPL: human placental lactogen; β-hCG: beta-human chorionic gonadotropin; CK-Pan: cytokeratin
Postoperative course and chemotherapy
A CT scan of the abdomen and pelvis was normal; however, chest imaging detected bilateral small pulmonary nodules, suggesting metastasis (Figure 5).
CT scan images.CT scan images showing bilateral small pulmonary nodules. The red arrows indicate small bilateral pulmonary metastases.
The patient was referred to gynecologic oncology and initially underwent five cycles of methotrexate. Due to plateauing β-hCG levels, a switch to dactinomycin was made. Following three cycles of dactinomycin, her β-hCG levels decreased to below 2.5 mIU/mL, and she continues to be monitored by the oncologist.
Discussion
Cornual pregnancies are associated with a high risk of rupture and hemorrhage, with a mortality rate of 2-2.5% [7]. Management approaches may vary based on clinical scenarios, including medical therapy, cornual resection, or hysterectomy [8].
The incidence of GTNs in Asian women is much higher compared to non-Asian women [9]. Our patient was aged 38 years, an age consistent with that of reports that ETT occurs primarily in women of reproductive age with a median age of 32 years. Term or preterm delivery was the most common type of antecedent pregnancy [10]. The majority of cases (67%) occur after full-term pregnancy [11]. This patient's antecedent pregnancy was preterm, and delivery was at 32 weeks gestation by cesarean section because of vaginal bleeding, which was due to placenta previa.
Diagnosis of ETT often faces delays because of its rarity and nonspecific clinical presentation, which can resemble ectopic pregnancy or choriocarcinoma. Histologically, ETT is distinct from choriocarcinoma, characterized by monomorphic intermediate trophoblastic cells, geographic necrosis, and a hyaline-like extracellular matrix; confirmation of ETT requires immunohistochemistry [12-14].
Surgical excision is the preferred treatment for localized ETT, as chemotherapy alone is frequently ineffective. For metastatic cases or those with persistently elevated β-hCG levels, multi-agent chemotherapy is advised. Our patient experienced a suboptimal response to methotrexate monotherapy but showed a positive response to dactinomycin, resulting in normalized β-hCG levels.
ETT has a higher mortality rate (10-24%) compared to post-molar GTN (6.5%) and choriocarcinoma (13.4%) [4,5,14]. Due to the potential for delayed diagnosis and resistance to monotherapy, early surgical intervention combined with multi-agent chemotherapy is vital for optimal outcomes.
Conclusions
This case illustrates an exceptionally rare presentation of ETT that was initially misdiagnosed as a cornual ectopic pregnancy. The diagnostic challenges associated with ETT highlight the necessity for histopathological and immunohistochemical verification in patients with persistently elevated β-hCG levels. While surgical resection is the primary treatment method, combined chemotherapy is essential for cases that are metastatic or resistant to initial treatment. Early identification and collaborative management are critical for enhancing patient prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1On the look out for a rarity - interstitial/cornual pregnancy Eur J Emerg Med Kun WM Tung WK 147150820011143691210.1097/00063110-200106000-00012 · doi ↗ · pubmed ↗
- 2Increase in the incidence of gestational trophoblastic disease in The Netherlands Gynecol Oncol [Internet] Lybol C Thomas CM Bulten J van Dijck JA Sweep FC Massuger LF 33433812120112124761810.1016/j.ygyno.2011.01.002 · doi ↗ · pubmed ↗
- 3Epithelioid trophoblastic tumors: treatments, outcomes, and potential therapeutic targets J Cancer Yang J Zong L Wang J Wan X Feng F Xiang Y 1119102019 http://dx.doi.org/10.7150/jca.281343066252010.7150/jca.28134 PMC 6329873 · doi ↗ · pubmed ↗
- 4Epithelioid trophoblastic tumor: a neoplasm distinct from choriocarcinoma and placental site trophoblastic tumor simulating carcinoma Am J Surg Pathol Shih IM Kurman RJ 13931403221998980813210.1097/00000478-199811000-00010 · doi ↗ · pubmed ↗
- 5Epithelioid trophoblastic tumor: a review of the literature J Reprod Med Palmer JE Macdonald M Wells M Hancock BW Tidy JA 465475532008 https://pubmed.ncbi.nlm.nih.gov/18720920/18720920 · pubmed ↗
- 6Epithelioid trophoblastic tumor: a single institution case series at the New England Trophoblastic Disease Center Gynecol Oncol Davis MR Howitt BE Quade BJ Crum CP Horowitz NS Goldstein DP Berkowitz RS 45646113720152577320310.1016/j.ygyno.2015.03.006 · doi ↗ · pubmed ↗
- 7Cornual invasive hydatidiform mole: a rare case report and literature review BMC Womens Health Qian J Xu S Chen L 5662320233791970410.1186/s 12905-023-02727-z PMC 10621079 · doi ↗ · pubmed ↗
- 8Management of a cornual ectopic pregnancy J Visc Surg Prenaud C Scherier S Malgras B 46746815420172915361710.1016/j.jviscsurg.2017.10.003 · doi ↗ · pubmed ↗