Optimal Surgical Strategies for Posterior Malleolar Ankle Fractures: A Morphology-Based Approach
Ting-Yu Chang, Chih-Wei Chang, Yen-Nien Chen

TL;DR
This study shows that the shape of ankle bone fractures, not just their size, should guide surgical decisions, with plates providing better results than screws or no surgery.
Contribution
The study introduces a morphology-based approach to surgical fixation of posterior malleolar fractures, emphasizing personalized strategies over traditional size-based methods.
Findings
Surgical intervention improved outcomes for specific fracture types compared to non-fixation.
Plate fixation resulted in lower joint instability than screw fixation.
Small-fragment fractures treated surgically had outcomes as good as or better than large-fragment cases.
Abstract
Background Surgical fixation of posterior malleolar fractures (PMFs) has traditionally been guided by fragment size. Recent studies have proposed fragment morphology as a more effective determinant for optimal fixation. To determine the optimal strategy for PMFs, we conducted a radiographic review of our patients. Methods Between January 2016 and December 2019, all adult patients with ankle fractures who underwent surgical fixation at our institution were reviewed (n=648). The exclusion criteria included pilon fractures, tumors, or infections causing neuromuscular dysfunction, insufficient follow-up, bilateral involvement, and prior injuries. After applying these criteria, 110 eligible patients remained for the study. They were further categorized on the basis of treatment type (non-fixation, screw, and plating) and fracture classification system (Haraguchi, Lauge-Hansen, and Weber…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
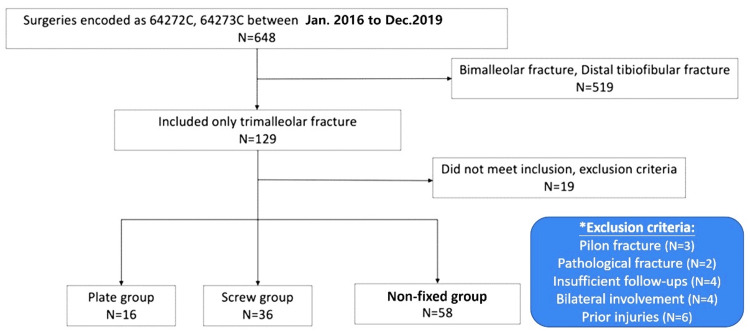 Figure 1
Figure 1 Figure 2
Figure 2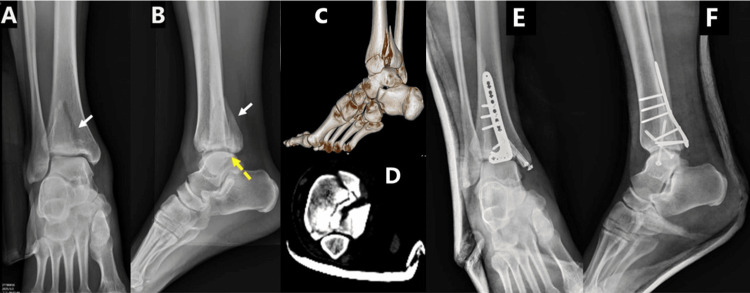 Figure 3
Figure 3| Characteristic | Plate | Screw | Non-fixation | Total | p-value |
| Gender | 0.50 | ||||
| Male | 6 | 8 | 16 | 30 | |
| Female | 10 | 28 | 42 | 80 | |
| Age | 50.4±17.6 | 50.4±14.9 | 49.8±13.2 | 50.1±14.4 | 0.98 |
| Inpatient stay | 3.9±1.4 | 5.4±3.9 | 4.7±4.5 | 4.7±3.4 | 0.18 |
| Articular involvement % | 35.9±9.6 | 33.4±9.1 | 23.1±11.3 | 28.3±10.3 | 0.00* |
| Weber classification | 0.59 | ||||
| A | 0 | 0 | 1 | 1 | |
| B | 10 | 26 | 45 | 81 | |
| C | 6 | 10 | 12 | 28 | |
| Lauge-Hansen classification | 0.13 | ||||
| SER | 11 | 28 | 51 | 90 | |
| PER | 3 | 5 | 7 | 15 | |
| PA | 2 | 3 | 0 | 5 | |
| SAD | 0 | 0 | 0 | 0 | |
| Haraguchi classification | 0.07 | ||||
| Type 1 | 11 | 13 | 20 | 44 | |
| Type 2 | 4 | 4 | 3 | 11 | |
| Type 3 | 0 | 0 | 6 | 7 | |
| Fracture morphology | Management | n (%) | Age | Art. surface (%) | K-L grade | Step off n (%) | ROI n (%) | Re-surgery n (%) | Wound poor heal n (%) | |||||
| Total | Osteophyte | Lateral-JSN | AP-JSN | Talar tilt n (%) | Talar Scl n (%) | |||||||||
| Dannis Weber Classification | ||||||||||||||
| B | Plate | 12 (14.6) | 51.8 (SD: 16.8) | 38.5 (SD: 9.5) | 1.33 (SD: 0.65) | 1.33 (SD: 0.78) | 0.83 (SD: 0.84) | 0.50 (SD: 0.52) | 0 (0) | 0 (0) | 4 (33.3) | 4 (33.3) | 5 (41.7) | 3 (25) |
| Screw | 27 (32.9) | 49.3 (SD: 15.8) | 33.2 (SD: 9.7) | 1.37 (SD: 0.69) | 11.41 (SD: 0.75) | 0.85 (SD: 0.53) | 0.81 (SD: 0.48) | 0 (0) | 0 (0) | 12 (44.4) | 2 (7.4) | 6 (22.2) | 2 (7.4) | |
| Non-fixation | 43 (52.4) | 49.8 (SD: 12.2) | 21.6 (SD: 6.8) | 1.77 (SD: 0.95) | 1.58 (SD: 0.70) | 1.28 (SD: 0.59) | 1.19 (SD: 0.55) | 4.7 (2) | 9.3 (4) | 22 (51.2) | NA | 19 (44.2) | 5 (11.6) | |
| P | 0.833 | <0.000* | 0.247 | 0.636 | 0.011* | <0.000* | 0.395 | 0.149 | 0.533 | 0.06 | 0.165 | 0.297 | ||
| C | Plate | 6 (21.4) | 47.5 (SD: 20.3) | 33.8 (SD: 9.7) | 1.83 (SD: 0.98) | 1.67 (SD: 0.52) | 1.17 (SD: 0.75) | 1.00 (SD: 1.10) | 0 (0) | 33.3 (2) | 1 (16.7) | 2 (33.3) | 2 (33.3) | 2 (33.3) |
| Screw | 10 (35.7) | 53.1 (SD: 12.6) | 35.1 (SD: 7.5) | 1.90 (SD: 1.10) | 1.80 (SD: 0.79) | 0.90 (SD: 0.99) | 1.00 (SD: 1.25) | 0 (0) | 40 (4) | 9 (90) | 1 (10) | 2 (20) | 1 (10) | |
| Conservative | 12 (42.9) | 49.8 (SD: 17.0) | 23.3 (SD: 8.3) | 1.33 (SD: 0.65) | 1.33 (SD: 0.78) | 1.08 (SD: 0.29) | 1.08 (SD: 0.29) | 0 (0) | 8.3 (1) | 3 (25) | NA | 5 (41.7) | 1 (8.3) | |
| P | 0.852 | 0.015* | 0.467 | 0.311 | 0.468 | 0.543 | NA | 0.202 | 0.002* | 0.304 | 0.555 | 0.321 | ||
| Lauge-Hansen Classification | ||||||||||||||
| SER | Plate | 13 (14.4) | 49.3 (SD: 18.5) | 38.2 (SD: 9.2) | 1.31 (SD: 0.63) | 1.31 (SD: 0.75) | 0.85 (SD: 0.80) | 0.54 (SD: 0.52) | 0 (0) | 0 (0) | 4 (30.8) | 4 (30.8) | 5 (38.5) | 3 (23.1) |
| Screw | 29 (32.2) | 49.8 (SD: 15.3) | 33.1 (SD: 9.4) | 1.48 (SD: 0.79) | 1.48 (SD: 0.79) | 0.90 (SD: 0.56) | 0.83 (SD: 0.54) | 0 (0) | 3.4 (1) | 14 (48.3) | 2 (6.9) | 6 (20.7) | 3 (10.3) | |
| Non-fixation | 48 (53.3) | 48,7 (SD: 13.5) | 21.3 (SD: 6.6) | 1.67 (SD: 0.93) | 1.50 (SD: 0.68) | 1.27 (SD: 0.57) | 1.17 (SD: 0.52) | 2 (4.2) | 5 (10.4) | 23 (47.9) | NA | 20 (41.7) | 5 (10.4) | |
| P | 0.902 | <0.000* | 0.563 | 0.858 | 0.017* | <0.000* | 0.409 | 0.287 | 0.512 | 0.063 | 0.163 | 0.434 | ||
| PER | Plate | 3 (20) | 54.7 (SD: 20.3) | 31.4 (SD: 11.7) | 2.33 (SD: 1.16) | 1.67 (SD: 0.58) | 1.33 (SD: 1.16) | 1.00 (SD: 1.73) | 0 (0) | 2 (66.7) | 1 (33.3) | 1 (33.3) | 1 (33.3) | 2 (66.7) |
| Screw | 5 (33) | 46.2 (SD: 13.7) | 33.0 (SD: 7.3) | 1.80 (SD: 1.30) | 1.60 (SD: 0.89) | 0.80 (SD: 1.30) | 0.80 (SD: 1.30) | 0 (0) | 3 (60) | 0 (0) | 0 (0) | 1 (20) | 0 (0) | |
| Non-fixation | 7 (46.7) | 57.3 (SD: 8.9) | 26.5 (SD: 9.4) | 1.71 (SD: 0.76) | 1.71 (SD: 0.95) | 1.00 (SD: 0.00) | 1.14 (SD: 0.38) | 0 (0) | 0 (0) | 2 (28.6) | 0 (0) | 4 (57.1) | 1 (14.3) | |
| P | 0.29 | 0.76 | 0.65 | 0.95 | 0.43 | 0.39 | NA | 0.037* | 0.037* | 0.375 | 0.418 | 0.065 | ||
| PA | Plate | 2 (40) | 51.0 (SD: 15.6) | 37.3 (SD: 12.2) | 1.50 (SD: 0.70) | 0.20 (SD: 0.00) | 1.00 (SD: 0.00) | 1.00 (SD: 0.00) | 0 (0) | 0 (0) | 0 (0) | 1 (50) | 1 (50) | 0 (0) |
| Screw | 3 (60) | 62.3 (SD: 9.0) | 41.2 (SD: 7.0) | 1.33 (SD: 0.58) | 1.67 (SD: 0.58) | 0.67 (SD: 0.58) | 1.33 (SD: 1.53) | 0 (0) | 0 (0) | 2 (66.7) | 1 (33.3) | 1 (33.3) | 0 (0) | |
| P | 0.25 | 0.56 | 0.74 | 0.41 | 0.41 | 1 | NA | NA | 0.3 | 0.7 | 0.7 | NA | ||
| Haraguchi Classification | ||||||||||||||
| Type 1 | Plate | 13 (29.5) | 52.2 (SD: 16.6) | 37.0 (SD: 10.6) | 1.38 (SD: 0.77) | 1.38 (SD: 0.77) | 1.00 (SD: 0.82) | 0.54 (SD: 0.52) | 0 (0) | 1 (7.7) | 2 (15.4) | 3 (23.1) | 4 (30.8) | 3 (23.1) |
| Screw | 14 (31.8) | 53.7 (SD: 14.1) | 34.2 (SD: 10.2) | 1.29 (SD: 0.91) | 1.21 (SD: 0.80) | 0.71 (SD: 0.61) | 0.79 (SD: 0.89) | 0 (0) | 2 (14.3) | 7 (50) | 1 (7.1) | 2 (14.3) | 2 (14.3) | |
| Non-fixation | 17 (38.6) | 53.4 (SD: 11.4) | 22.4 (SD: 6.9) | 2.00 (SD: 1.00) | 1.59 (SD: 0.62) | 1.35 (SD: 0.70) | 1.35 (SD: 0.70) | 1 (5.9) | 3 (17.6) | 8 (47.1) | NA | 6 (35.3) | 3 (17.6) | |
| P | 0.95 | 0.033* | 0.08 | 0.34 | 0.07 | 0.01* | 0.44 | 0.73 | 0.12 | 0.27 | 0.4 | 0.84 | ||
| Type 2 | Plate | 4 (36.4) | 52.3 (SD: 17.4) | 37.4 (SD: 8.1) | 2.00 (SD: 0.82) | 1.75 (SD: 0.50) | 0.75 (SD: 0.96) | 1.00 (SD: 1.41) | 0 (0) | 1 (25) | 3 (75) | 3 (75) | 3 (75) | 2 (50%) |
| Screw | 4 (36.4) | 58.5 (SD: 11.2) | 30.5 (SD: 21.4) | 1.25 (SD: 0.50) | 1.25 (SD: 0.50) | 1.00 (SD: 0.00) | 1.00 (SD: 0.00) | 0 (0) | 0 (0) | 3 (75) | 0 (0) | 2 (50) | 0 (0) | |
| Non-fixation | 3 (27.3) | 24.1 (SD: 6.7) | 48.7 (SD: 9.6) | 2.00 (SD: 0.00) | 2.00 (SD: 1.00) | 1.00 (SD: 0.00) | 1.00 (SD: 0.00) | 0 (0) | 0 (0) | 2 (66.7) | 0 (0) | 2 (66.7) | 0 (0) | |
| P | 0.58 | 0.15 | 0.16 | 0.33 | 0.7 | 0.7 | NA | 0.38 | 0.96 | 0.07 | 0.76 | 0.12 | ||
| Type 3 | Non-fixation | 6 (100) | 41.2 (SD: 13.0) | 16.5 (SD: 49.7) | 1.17 (SD: 0.41) | 1.17 (SD: 0.41) | 1.17 (SD: 0.41) | 1.00 (SD: 0.00) | 0 (0) | 0 (0) | 2 (33.3) | NA | 4 (66.7) | 1 (16.7) |
| Fragment Size | ||||||||||||||
| Large | Plate | 16 (25) | 50.8 (SD: 18.5) | 38.7 (SD: 8.6) | 1.44 (SD: 0.73) | 1.44 (SD: 0.73) | 0.87 (SD: 0.81) | 0.69 (SD: 0.79) | 0 (0) | 1 (6.3) | 5 (31.3) | 6 (37.5) | 7 (43.8) | 5 (31.3) |
| Screw | 32 (50) | 52.3 (SD: 13.9) | 35.9 (SD: 7.5) | 1.47 (SD: 0.84) | 1.47 (SD: 0.76) | 0.84 (SD: 0.68) | 0.88 (SD: 0.79) | 0 (0) | 4 (12.5) | 19 (59.4) | 2 (6.3) | 7 (21.9) | 3 (9.4) | |
| Non-fixation | 16 (25) | 51.4 (SD: 14.5) | 30.7 (SD: 5.3) | 1.87 (SD: 1.20) | 1.81 (SD: 0.91) | 1.38 (SD: 0.72) | 1.25 (SD: 0.68) | 2 (12.5) | 2 (12.5) | 5 (31.3) | NA | 6 (37.5) | 2 (12.5) | |
| P | 0.96 | 0.01* | 0.51 | 0.35 | 0.06 | 0.04* | 0.05 | 0.79 | 0.08 | 0.01* | 0.25 | 0.13 | ||
| Small | Plate | 2 (4.3) | 47.0 (SD: 8.5) | 23.0 (SD: NA) | 2.00 (SD: 1.41) | 1.50 (SD: 0.71) | 1.50 (SD: 0.71) | 0.50 (SD: 0.71) | 0 (0) | 1 (50) | 2 (100) | 0 (0) | 2 (100) | 2 (100) |
| Screw | 5 (10.9) | 37.6 (SD: 16.6) | 20.0 (SD: 6.1) | 1.80 (SD: 0.84) | 1.80 (SD: 0.84) | 1.00 (SD: 0.71) | 0.80 (SD: 0.45) | 0 (0) | 0 (0) | 2 (40) | 1 (20) | 1 (20) | 0 (0) | |
| Non-fixation | 39 (84.8) | 49.2 (SD: 12.8) | 18.4 (SD: 4.0) | 1.59 (SD: 0.75) | 1.41 (SD: 0.60) | 1.18 (SD: 0.45) | 1.13 (SD: 0.41) | 0 (0) | 3 (7.7) | 20 (51.3) | NA | 18 (46.2) | 4 (10.3) | |
| P | 0.29 | 0.23 | 0.71 | 0.48 | 0.41 | 0.02* | NA | 0.09 | 0.34 | 0.71 | 0.26 | 0.67 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Sports injuries and prevention · Tendon Structure and Treatment
Introduction
Ankle fractures account for approximately 9% of all fractures, with posterior malleolar fractures (PMFs) comprising 10% to 44% of these injuries. The most common mechanism is supination-external rotation (SER) [1,2]. In ankle fractures, untreated PMFs may lead to posttraumatic osteoarthritis, characterized by abnormalities such as joint step-offs, narrowing of the ankle joint space, and osteophyte formation [3].
Traditionally, surgical fixation of PMFs is recommended when the fragment involves more than 25% of the articular surface, as measured on lateral radiographs [3-5]. However, this size-based criterion may oversimplify the clinical decision-making process, and consequently, the optimal timing and methodology for PMF fixation remain controversial [6,7]. With respect to biomechanics, plating provides better stability for PMFs [8,9], and Bartoníček et al. [10] first proposed the use of a buttress plate to provide stable fixation. However, its clinical superiority over conventional screw fixation requires further investigation.
Haraguchi et al. classified rotational-type PMFs on the basis of CT images at the tibial plafond level, and three subtypes were recognized [11]. Studies suggest that morphology, rather than size, is an independent predictor of patient outcomes and should guide the choice of fixation method [12]. Notably, no current studies have conclusively identified the best surgical method for each morphological subtype.
The primary aim of this study was to refine the conventional criterion of >25% articular involvement by taking fracture morphology into treatment algorithms for PMFs. We hypothesized that morphological characteristics, obtained from either computed tomography (CT) or extrapolated from plain radiographs, would serve as a more ideal guide to appropriate fixation methodology.
Materials and methods
Study design and period
With the approval of the Institutional Review Board, National Cheng Kung University Hospital, we conducted a retrospective study of patients with procedural codes 64272C and 64273C, which are specific to surgical fixation of multimalleolar fractures, between 2016 and 2019 at our hospital.
Inclusion and exclusion criteria
We screened medical records and radiographs to identify adult candidates suffering unilateral ankle fractures involving the posterior malleolus during the study period, as shown in Figure 1. The exclusion criteria were pilon fractures, clinical follow-up of less than six months, prior trauma to the ipsilateral lower limb, prior or concurrent neuromuscular dysfunction affecting the evaluation, and concurrent tumor or infection status.
Flow diagram of eligible patients and exclusions, resulting in the study population
Surgical interventions
All surgical fixation procedures were performed by 12 trained orthopedic surgeons experienced in trauma surgery. Patients received either posterior-anterior (PA) or anterior-posterior (AP) lag screws, plate fixation, or non-fixation treatment for the PMFs.
For the plate group, patients were positioned in either the prone or lateral decubitus position, depending on the surgeon’s preference and the location of the fracture fragment. Fixation was performed through either a posterolateral or posteromedial approach, selected to optimize visualization and access to the fracture site. Various plates were used for internal fixation of the displaced PMFs as a buttress, including the Synthes Variable Angle LCP Ankle Trauma System (Paoli, PA, USA), the Aplus Distal Fibula Double Hook Locking Plate System (Taipei, Taiwan), and the Hung Chun Plate System O103 (Taipei, Taiwan).
In the screw group, the posterior malleolus was accessed through medial, lateral, or posterolateral incisions. Medial or lateral incisions were used for AP screw fixation. For lag screws, the anterior cortex was overdrilled to achieve the lag effect. The posterior fragment was identified by retracting the Achilles tendon medially and the peroneal tendons laterally. One to two lag screws were placed from posterior to anterior into the distal tibial metaphysis. The lateral or medial malleolus was repaired after the posterior fracture was fixed. Fragment positions and screws were confirmed via C-arm radiographs before wound closure in all patients.
For the non-fixation group, patients had trimalleolar fractures but only underwent fixation for the medial and/or lateral malleolus, leaving the PMF unfixed. The posterior malleolar fragment was allowed to heal through conservative management.
Radiographic evaluation
We obtained lateral and mortise radiographs, both pre-surgery and post-surgery, for evaluation. For pre-operative evaluation, the traditional measurement method on lateral plain radiographs was used, as shown in Figure 2. Based on the size of the fracture fragment and 25% involvement of the joint surface, the patients were further classified into large fracture and small fracture groups. We assessed morphological characteristics using the Weber and Lauge-Hansen (L-H) classification systems, derived from high-quality lateral and mortise radiographic views, which have demonstrated reasonable correlation with CT in fracture characterization. In cases where CT imaging was available, fractures were further subclassified according to the Haraguchi classification into three types: type 1, characterized by a posterolateral-oblique fragment; type 2, involving medial extension into the posteromedial tibial plafond; and type 3, consisting of a small shell-type fragment limited to the posterior lip of the tibia.
Measurement of fragment size via lateral viewThe percentage of the involved articular surface is calculated as II / (I + II). Based on the fracture fragment size and 25% joint surface involvement, patients were classified into large and small fracture groups.
The severity of postoperative arthritis was evaluated via the modified Kellgren-Lawrence (K-L) grade, as provided by Kraus et al. [13]. Standard anteroposterior and lateral radiographs of the affected ankle were reviewed by two independent observers. Joint space narrowing (JSN) was defined based on the visual reference atlas published by Kraus et al., without comparison to the contralateral side. K-L grading incorporated JSN, osteophytes, talar tilt, and subchondral sclerosis in a composite score (range 0-4). We also evaluated the step-off of the posterior malleolus as an outcome measure. Postoperative radiographs used for this evaluation were obtained at a minimum of six months post-surgery and no later than eight months for all included patients.
Statistical analysis
All the statistical analyses were performed via SPSS Statistics for Windows, Version 17 (Released 2008; SPSS Inc., Chicago, United States). Continuous variables are presented as the means ± standard deviations. The Kruskal-Wallis test was used to compare grading between groups. For intergroup comparisons of continuous variables that did not follow a normal distribution, the Mann-Whitney U test was utilized. The Pearson chi-square test was used to compare categorical variables between the groups. Statistical significance was set at p < 0.05.
Results
During the study period, a total of 110 patients were included in this study. The patients' demographic characteristics are shown in Table 1. CT images were available for 62 patients and were classified according to the Haraguchi classification system; 44 patients had Haraguchi type 1 fractures, 11 patients had type 2 fractures, and 7 patients had type 3 fractures. Including those with CT images, all 110 patients were classified according to the L-H and Weber classification systems utilizing the radiographs. L-H SER and Weber B fractures accounted for the majority of fractures. Patients were further stratified based on fragment size and joint surface involvement, leading to the classification of 64 cases as large fractures and 46 as small fractures.
Joint space narrowing and fixation methods
As shown in Table 2, for the most common fracture morphologies, L-H SER and Weber B plate fixation resulted in the least JSN on both lateral and AP views, showing a significant difference compared to other treatments. The most severe JSN was observed in patients who underwent non-fixation treatment, followed by those treated with screw fixation.
When accounting for fragment size, despite having larger fragments, the plate fixation group still had the least JSN, whereas conservative treatment led to the most severe narrowing even with smaller posterior malleolar fragments.
Outcomes based on Haraguchi classifications
For Haraguchi type 1 patients, those posterior malleolar fragments that were left non-fixed had a smaller percentage of articular involvement (p=0.033) but ended up with significantly more severe JSN on AP view (p=0.001) as detailed in Table 2. There were no significant differences between treatments for Haraguchi type 2, and as all Haraguchi type 3 fractures were managed non-operatively, no interventional comparison was performed for this group.
Patients with Weber C fractures and L-H pronation-external rotation (PER) fractures who underwent plate fixation had significantly lower step-off rates compared to those treated with screws or non-fixation management (p=0.002, p=0.037). Notably, among patients with Weber C fractures, 9 out of 10 who underwent screw fixation experienced step-off deformities at follow-up, whereas only one out of six patients in the plate fixation group exhibited step-off.
Others
Regarding the need for secondary surgery, no significant differences were observed among the three treatment groups across different fracture morphologies. However, in cases involving large fracture areas, plate fixation was associated with a higher likelihood of requiring a second procedure for implant removal compared to screw fixation (p=0.01).
Discussion
To determine how different fractures respond to various treatments for PMFs, the authors conducted a retrospective image analysis of various fracture morphologies. Our findings indicated that plate fixation provided the best treatment outcomes among the three fracture types: Lauge-Hansen classification SER, Weber B, and Haraguchi type 1. Additionally, although there were no significant differences in outcomes for patients with PER or PA morphology within the L-H classification, a trend suggested that plate fixation still resulted in better outcomes than other treatment methods did.
In 2020, Blom et al. noted that clinical outcomes for PMF type 2 patients are generally worse than those for patients with type 1 or type 3 [12]. Therefore, it was assumed that PMF type 2 would benefit the most from plate fixation (Figure 3). However, our results suggest that plate fixation is associated with better outcomes only for Haraguchi type 1 fractures. Although previous studies have suggested that PMF type 2 fractures benefit the most from plate fixation, our findings indicate that the fractures most likely to benefit from plate fixation are Haraguchi type 1, L-H SER, and Weber B, as these were the most common fracture patterns within their respective classifications. While Haraguchi type 2 fractures did not show a statistically significant advantage, a trend favoring plate fixation was observed in this study. This may be attributed to the limited sample size. Based on the study's primary outcomes, we recommend plate fixation for all fracture types, except for fractures like Haraguchi type 3, which represents a small shell morphology and may not derive the same level of benefit.
Surgical fixation of a Haraguchi type 2 posterior malleolar fracture using a plateA 58-year-old male sustained a fall from a height of 2 meters, resulting in a right ankle fracture involving the posterior malleolus. Preoperative radiographs (A and B) showed the fracture, with white arrows indicating the affected area. Although the lateral view (B, yellow dotted arrow) suggested minimal involvement of the articular surface, a CT scan (C, D) revealed medial extension of the fracture, classifying it as Haraguchi type 2. To address this, a posteromedial approach with plate fixation was chosen for internal fixation. Postoperative imaging confirmed the successful restoration of the articular surface (F).A, B: Preoperative AP and lateral radiographic views; C: 3D reconstruction based on a CT scan; D: Transverse section of the CT scan at the plafond level; E, F: Postoperative AP and lateral views
In this study, large PMF fragments were more likely to receive surgical intervention, adhering to traditional guidelines for fixing PMFs when they involve more than 25% of the tibial plafond. However, both large and small fragment groups demonstrated similar outcomes across the different treatments, with no significant differences between them. This finding underscores that fragment size alone is insufficient for determining the optimal treatment strategy. While a >25% articular surface involvement on lateral radiographs is traditionally considered the threshold for fixation, our results suggest that morphology provides more clinically relevant insights. For example, although both may be classified as small fragments, a Haraguchi type 2 fragment that extends medially - commonly seen in PER fractures - has greater biomechanical significance than a thin posterior shell typically observed in type 3 fractures. Therefore, even when CT is unavailable, morphology assessed using standardized lateral and mortise radiographs may better guide the choice between plate fixation, screw fixation, or non-fixation compared to relying solely on fragment size [14].
In addition to morphology, fracture fragment displacement is critical in determining the need for surgical fixation in PMFs. Traditionally, a displacement threshold of greater than 2 mm on lateral radiographs has been used as a key indication for fixation, along with fragment size exceeding 25-30% of the tibial plafond. However, defining an absolute cut-off for displacement in clinical imaging remains challenging, particularly in cases with complex fracture morphology. Standard lateral radiographs provide only a two-dimensional evaluation, which may not accurately reflect the true extent of displacement in axial or coronal planes. This issue is even more pronounced in three-dimensional imaging, where a reliable method for quantifying displacement is lacking. Future studies should focus on developing standardized displacement measurement protocols and incorporating three-dimensional assessment techniques to enhance surgical decision-making for PMFs.
Our results support the use of plates in certain patients. Although patients who undergo plate fixation generally have larger posterior fragments, this method provides better stability and outcomes, including lower step-off rates and reduced JSN, than screws do, particularly in Haraguchi type 1, L-H SER, and Weber B fractures. The advantages of plate fixation stem from multiple factors. Karaca et al. [15] highlighted the importance of anatomical reduction and rigid internal fixation for the posterior malleolus to achieve satisfactory clinical and functional outcomes. Proper reduction of the articular surface is crucial for preventing post-traumatic arthritis.
Studies have shown that both screws and plates can achieve adequate reduction [16,17]. Non-fixation treatment, however, is not recommended for a majority of PMF subtypes [10]. Xing et al. [18] analyzed 30 patients with dislocated trimalleolar fractures and complex PMFs, finding satisfactory outcomes after three months. Patients treated with plate fixation had better Short Musculoskeletal Function Assessment Questionnaire (SMFA) discomfort scores and showed trends toward improved functional and mobility subscores [19].
However, plates have certain drawbacks. In addition to being more expensive, plates placed close to the distal tibia may protrude at the most distal part, causing irritation to surrounding soft tissues, such as the flexor hallucis longus. Unlike screws, plates cannot sink the head, which may lead to discomfort. Our study also revealed a higher rate of implant removal requests among patients with PMFs fixed with plates.
Limitations
Several limitations warrant consideration in the interpretation of our findings. First, the insufficient sample size of patients with specific fracture morphologies prevented their inclusion in the analysis. Additionally, procedural heterogeneity arose due to variations in surgical techniques among the 12 participating surgeons, and the plates used were not specifically designed for posterior malleolar fixation. Although individual follow-up durations were not presented in a dedicated table, all patients underwent clinical evaluation for a minimum of six months postoperatively, with the majority followed for approximately one year. Radiographic assessments, focusing on early degenerative changes, were conducted within a standardized early postoperative window, rather than evaluating long-term functional outcomes. Future studies incorporating prospective mid- to long-term follow-ups, advanced imaging techniques, and anatomically designed plates are warranted to provide stronger evidence in clinical practice.
Conclusions
This retrospective radiographic assessment highlights the significance of fracture morphology, rather than fragment size, in guiding surgical strategies for PMFs. Plate fixation provides superior joint stability and outcomes compared to screws or non-fixation but is associated with a higher removal rate. Personalized approaches based on fracture patterns can enhance patient care. Future research should prioritize advanced imaging, mid-to-long-term follow-ups, and anatomically designed plates to strengthen clinical evidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Population-based epidemiology of 9767 ankle fractures Foot Ankle Surg Elsoe R Ostgaard SE Larsen P 34392420182941377110.1016/j.fas.2016.11.002 · doi ↗ · pubmed ↗
- 2Reconciliation between lateral X-ray and axial computed tomography regarding posterior malleolus fracture anatomy and medial malleolus involvement: a pilot study J Foot Ankle Surg Black AT Stowers JM Bohm AR Katchis SD Spielfogel W Weiner LS 5075116020213350971510.1053/j.jfas.2020.07.006 · doi ↗ · pubmed ↗
- 3Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures J Trauma Jaskulka RA Ittner G Schedl R 15651570291989258556910.1097/00005373-198911000-00018 · doi ↗ · pubmed ↗
- 4Trimalleolar fractures of the ankle. An end result study Clin Orthop Relat Res Mc Daniel WJ Wilson FC 37451977402247 · pubmed ↗
- 5Long-term results of ankle fractures with a posterior malleolar fragment J Foot Ankle Surg De Vries JS Wijgman AJ Sierevelt IN Schaap GR 2112174420051594060010.1053/j.jfas.2005.02.002 · doi ↗ · pubmed ↗
- 6Posterior malleolus fractures: worth fixing Bone Joint J Solan MC Sakellariou A 141314199920172909297810.1302/0301-620X.99B 11.BJJ-2017-1072 · doi ↗ · pubmed ↗
- 7In defence of the posterior malleolus Bone Joint J White TO 56656910020182970110010.1302/0301-620X.100B 5.BJJ-2017-1440.R 1 · doi ↗ · pubmed ↗
- 8A biomechanical comparison of posterior malleolar fracture fixation using screws and locking plates in Trimalleolar fractures: a finite element study BMC Musculoskelet Disord Chang CW Chen YN Jhong GH Su KC Li CT 1312620253992070710.1186/s 12891-025-08385-6PMC 11806853 · doi ↗ · pubmed ↗