Helicobacter heilmannii Infection With Concurrent Gastric Cancer: A Case Report
Tomohiro Kamio, Yoshiyasu Kono, Masaya Iwamuro, Tomoki Yoshikawa

TL;DR
A rare case of gastric cancer linked to Helicobacter heilmannii infection is reported, highlighting its distinct features and potential role in cancer development.
Contribution
This case report adds to the understanding of H. heilmannii's role in gastric cancer and its unique clinical and histological features.
Findings
H. heilmannii infection was confirmed in a patient with multiple early gastric cancers and negative H. pylori test.
Cobblestone-like gastritis and lymphocyte-dominant infiltration were observed, distinct from H. pylori-associated gastritis.
Endoscopic submucosal dissection achieved curative resection without recurrence in this case.
Abstract
Helicobacter heilmannii (H. heilmannii), a zoonotic pathogen, is increasingly recognized as a cause of gastritis and a potential risk factor for gastric cancer, despite its rarity. Here, we report a case of multiple synchronous early gastric cancers in a female patient in her 40s with H. heilmannii-associated gastritis. She underwent an esophagogastroduodenoscopy (EGD) for the evaluation of gastric discomfort. Endoscopy revealed cobblestone-like gastritis. Histological examination confirmed a signet ring cell carcinoma. Helicobacter pylori (H. pylori) antibody test was negative, and spiral-shaped bacteria were detected by Giemsa staining and real-time polymerase chain reaction (PCR), confirming H. heilmannii infection. Endoscopic submucosal dissection achieved curative resection without recurrence. Helicobacter heilmannii-induced gastritis presents distinct features, including a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
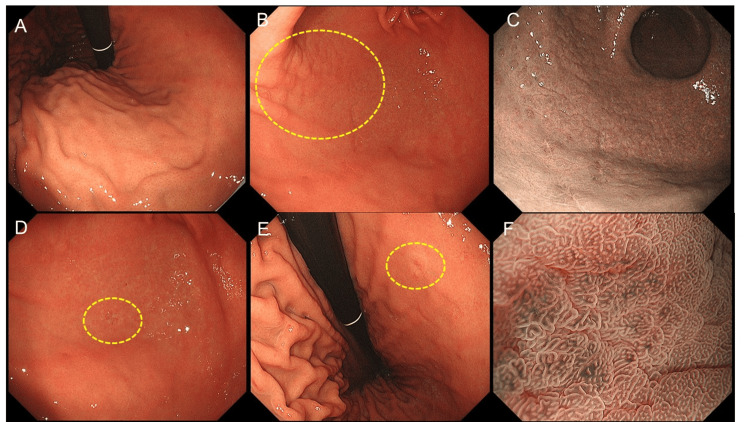 Figure 1
Figure 1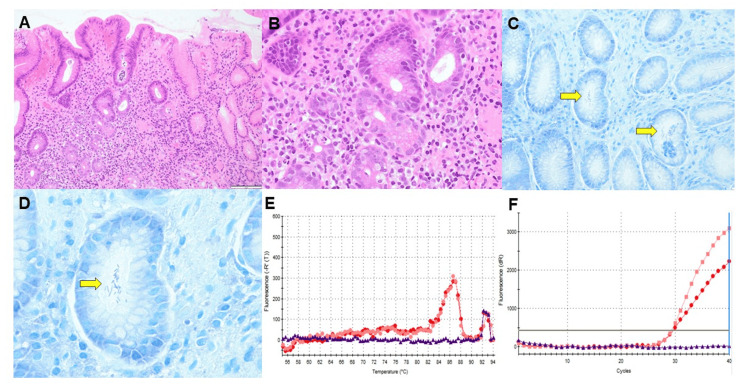 Figure 2
Figure 2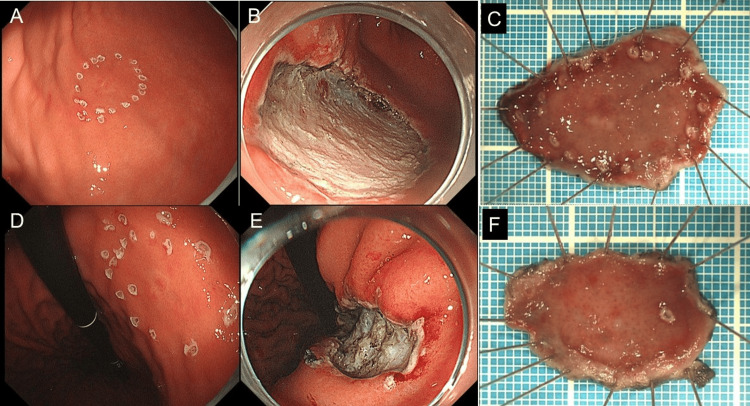 Figure 3
Figure 3| Test | Observed value | Reference range |
| WBC | 5.1×103/μL | 3.3-8.6×103/μL |
| RBC | 4.02×106/μL | 3.86-4.92×106/μL |
| Hb | 13.9 g/dL | 11.5-14.8 g/dL |
| PLT | 294×103/μL | 158-348×103/μL |
| PT | 102 % | 73-118 % |
| PT-INR | 0.99 | |
| APTT | 26.3 seconds | 26.9-38.1 seconds |
| TP | 7.0 g/dL | 6.6-8.1 g/dL |
| ALB | 4.4 g/dL | 4.1-5.1 g/dL |
| T.Bil | 0.5 mg/dL | 0.4-1.5 mg/dL |
| AST | 13 U/L | 13-30 U/L |
| ALT | 9 U/L | 7-23 U/L |
| ALP | 41 U/L | 38-113 U/L |
| LDH | 176 U/L | 124-222 U/L |
| Na | 142 mmol/L | 138-145 mmol/L |
| K | 3.5 mmol/L | 3.6-4.5 mmol/L |
| Cl | 106 mmol/L | 101-108 mmol/L |
| BUN | 10.8 mg/dL | 8.0-20.0 mg/dL |
| Cr | 0.58 mg/dL | 0.46-0.79 mg/dL |
| CRP | 0.02 mg/dL | < 0.15 mg/dL |
| CEA | 2.08 ng/mL | < 5.0 ng/mL |
| CA 19-9 | 31.9 U/mL | 0.0-35.4 U/mL |
| Serum anti-HP antibody titer | 3 U/mL | < 10 U/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Mycobacterium research and diagnosis · Toxin Mechanisms and Immunotoxins
Introduction
Helicobacter pylori (H. pylori) is well known for its role in chronic gastritis, peptic ulcers, and gastric cancer, and its eradication is the recommended strategy for gastric cancer prevention. In recent years, however, other species of *Helicobacter *that are not H. pylori, are collectively known as non-*H. pylori Helicobacter *(NHPH), have also been implicated in gastric disease [1-3]. Among these, *Helicobacter heilmannii *(H.heilmannii) is a zoonotic pathogen found in animals such as dogs, cats, and pigs. Human infection is rare, accounting for an estimated 0.1% to 0.6% of *Helicobacter *infections in developed countries; however, it is increasingly associated with chronic gastritis and may play a role in gastric carcinogenesis [4, 5].
Helicobacter heilmannii-associated gastritis presents distinct endoscopic and histological features compared with H. pylori, including a cobblestone-like appearance in the gastric antrum and lymphocyte-dominant infiltration with less neutrophilic activity. These unique features can aid in diagnosis, as conventional H. pylori tests such as rapid urease testing are typically negative in NHPH cases. Although the mechanisms linking *H. heilmannii *to gastric cancer are not fully understood, cobblestone-like gastritis has been suggested as a potential risk factor, particularly for undifferentiated carcinomas [6].
Here, we present a rare case of multiple synchronous early gastric cancers in a patient with H. heilmannii-associated gastritis, highlighting the importance of recognizing NHPH infections in gastric cancer risk assessment, even in H. pylori-negative patients. This report aimed to add to our understanding of the potential role of H. heilmannii in gastric carcinogenesis.
Case presentation
The patient was a female in her 40s. She had a medical history of total hysterectomy for cervical cancer. The patient had no family history of any cancer. She had never smoked and occasionally consumed alcohol. She had been raising dogs and cats for several decades. She complained of epigastric discomfort, and esophagogastroduodenoscopy (EGD) was performed to investigate the cause of the symptom. A flat, pale lesion measuring 5 mm was identified at the anterior wall of the greater curvature of the gastric angle. The histological diagnosis based on forceps biopsy was a signet ring cell carcinoma. The patient was referred to our hospital for further evaluation and treatment.
No unusual physical or laboratory findings were observed. Serum H. pylori antibody test results were negative, and tumor markers (CEA, CA-19-9) were within the normal range (Table 1). A contrast-enhanced CT scan revealed no obvious metastasis.
The EGD was performed again at our hospital and showed the presence of a regular arrangement of collecting venules up to the lesser curvature of the gastric angle, with no atrophic changes in the gastric body mucosa (Figure 1A). Fissure-like mucosa was observed in the gastric antrum, and small elevations were prominent at the anterior wall of the greater curvature of the gastric antrum, showing a cobblestone-like appearance of gastritis (Figures 1B-1C). In addition to the lesion detected at the previous hospital (Figure 1D), another flat, pale-colored lesion, 5 mm in diameter, was found at the posterior wall of the lesser curvature of the gastric angle (Figure 1E). The magnified narrow-band image of the cancerous lesion is shown in Figure 1F. Histological diagnosis using forceps biopsy revealed signet ring cell carcinoma.
The patient's endoscopic imagesThe scope used for the examination was the GIF-H290Z (Olympus Corporation, Tokyo, Japan)(A) Endoscopic image showing the regular arrangement of collecting venules in the gastric body without atrophic changes, typical in non-Helicobacter pylori Helicobacter infections. (B) White-light image and (C) narrow-band image showing a cobblestone-like appearance of the gastric antrum, with small elevated lesions and a fissured mucosal pattern, suggesting chronic gastritis due to Helicobacter heilmannii infection. (D) Endoscopic image showing the lesion previously diagnosed as a signet ring cell carcinoma at another hospital. (E) Endoscopic image showing the second flat, pale lesion (5 mm in diameter) located at the posterior wall of the lesser curvature of the gastric angle. This lesion was also diagnosed as a signet ring cell carcinoma. (F) Magnified image-enhanced endoscopic images of the lesion using narrow-band imaging.
A biopsy of the non-neoplastic area of the gastric antrum showed mild atrophic changes in the gastric mucosa according to the updated Sydney system [7] (evaluation of the antrum only), with mild infiltration of inflammatory cells compared with H. pylori-infected gastritis (Figures 2A-2B). Giemsa staining revealed large spiral bacteria in the pyloric gland area (Figures 2C-2D), suggesting NHPH infection, which was confirmed by real-time polymerase chain reaction (PCR) as H. heilmannii (Figures 2E-2F). Based on these findings, the patient was diagnosed with early gastric cancer that developed concurrently with cobblestone gastritis caused by H. heilmannii infection.
Histological images and polymerase chain reaction (PCR) amplification curves(A) and (B): Histopathological images of the non-cancerous gastric antrum showing mild atrophic changes according to the updated Sydney classification system, with mild inflammatory infiltration compared with typical Helicobacter pylori-associated gastritis. (C) and (D): Giemsa-stained sections revealing large spiral-shaped bacteria within the pyloric gland area, confirming Helicobacter heilmannii (H. heilmannii) infection. (E) and (F) Real-time PCR results confirming the presence of H. heilmannii DNA in the gastric biopsy specimen, establishing a definitive diagnosis of H. heilmannii infection.
The patient underwent endoscopic submucosal dissection for the two lesions (Figure 3). The pathological findings were pT1a, pUL0, Ly0, V0, pHM0, pVM0, and pStage IA in both lesions, resulting in successful curative resection.
Endoscopic images during gastric endoscopic submucosal dissection and photographs of the resected specimen(A) Endoscopic image after marking of the first lesion; (B) Endoscopic image of the ulcer after resection of the first lesion; (C) Image of the resected specimen of the first lesion; (D) Endoscopic image after marking of the second lesion; (E) Endoscopic image of the ulcer after resection of the second lesion; (F) Image of the resected specimen of the second lesion
Discussion
Non-*H. pylori Helicobacter *infections are uncommon in humans, with H. heilmannii being a notable example associated with gastric diseases [1-3]. Unlike H. pylori, which is well established as a causative factor for various gastric conditions, the role of NHPH, particularly H. heilmannii, in gastric carcinogenesis remains unclear owing to its rarity and difficulty in detection. This case of multiple synchronous early gastric cancers occurring in H. heilmannii-infected gastritis provides insights into the potential association between NHPH and gastric cancer.
Helicobacter heilmannii is known to naturally infect animals, especially dogs, cats, and pigs. Human infections likely result from close contact with these animals, which is consistent with our patient's long-term pet ownership [4, 5]. Endoscopically,* H. heilmannii* infection often presents distinct characteristics from H. pylori infection, including the absence of atrophy in the gastric body and a unique cobblestone-like appearance or fissured mucosa in the antrum [8-11]. These features were evident in the present case, in which cobblestone gastritis was observed along with two early-stage carcinomas in the gastric angle. This has been postulated to arise from immune responses specifically induced by H. heilmannii, leading to inflammation and altered gastric mucosal architecture [6].
Although the exact mechanisms underlying H. heilmannii-induced gastric cancer remain unknown, several hypotheses have been proposed. First, chronic inflammation and immune modulation due to persistent bacterial infections may contribute to an environment conducive to carcinogenesis. *Helicobacter heilmannii *infection often results in lymphocyte-dominant infiltration, a pattern that is distinct from the neutrophil-rich response typically observed in H. pylori infection [12, 13]. This type of inflammation can predispose patients to carcinogenesis, particularly in the presence of cobblestone-like gastritis, which is associated with undifferentiated gastric cancer. Second, co-infection with H. pylori has been suggested as a potential factor in some cases, although this was not observed in our patient. Studies have indicated that the co-existence of multiple *Helicobacter *species increases the risk of malignancy, possibly through synergistic inflammatory effects or enhanced mucosal damage [14]. However, given the negative *H. pylori *antibody results in this patient, it is more likely that carcinogenesis was directly associated with H. heilmannii infection.
Histopathologically, H. heilmannii-infected gastritis tends to display milder inflammatory cell infiltration with larger, spiral-shaped bacteria that can be identified using special stains such as Giemsa. In contrast to H. pylori-related gastritis, lymphocytic predominance in the inflammatory infiltrate has been noted. This distinct pattern is valuable in differential diagnosis, particularly in cases where typical H. pylori-related features are absent but the risk of gastric cancer remains high. Additionally, genetic predispositions such as hereditary diffuse gastric cancer were considered; however, no family history or clinical findings supporting a genetic cancer predisposition were identified.
Diagnosing H. heilmannii infection is challenging because of the limited sensitivity of conventional tests, such as rapid urease and urea breath tests, which are optimized for *H. pylori *detection. Although useful, real-time PCR and culture methods are not routinely used in clinical practice [15, 16]. Thus, there is a need for enhanced awareness of the signs of NHPH infection among clinicians, especially given the unique endoscopic features of H. heilmannii.
Therapeutically, *H. heilmannii *eradication regimens are generally based on *H. pylori *protocols. However, the effectiveness and long-term impact of eradication on disease prevention remain unclear [17]. Given the zoonotic nature of H. heilmannii, re-infection may occur if there is environmental exposure, such as close contact with animals. Therefore, eradication treatment considerations should include patient lifestyle and potential re-exposure risks.
Conclusions
In conclusion, this case emphasizes the importance of considering NHPH infection, particularly* H. heilmannii*, in cases of gastric cancer with non-H. pylori-related gastritis features. The appearance of cobblestone-like gastritis combined with chronic inflammation may contribute to the development of gastric cancer, underscoring the need for vigilance in diagnosing and managing NHPH infections. Further studies are necessary to clarify the oncogenic potential of* H. heilmannii* and to establish effective diagnostic and therapeutic protocols for NHPH-associated gastric diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastritis due to spiral shaped bacteria other than Helicobacter pylori: clinical, histological, and ultrastructural findings Gut Heilmann KL Borchard F 137140321991186453010.1136/gut.32.2.137PMC 1378794 · doi ↗ · pubmed ↗
- 2Non-Helicobacter pylori Helicobacter species in the human gastric mucosa: a proposal to introduce the terms H. heilmannii sensu lato and sensu stricto Helicobacter Haesebrouck F Pasmans F Flahou B Smet A Vandamme P Ducatelle R 3393401620112176227610.1111/j.1523-5378.2011.00849.x · doi ↗ · pubmed ↗
- 3Helicobacter heilmannii sp. nov., isolated from feline gastric mucosa Int J Syst Evol Microbiol Smet A Flahou B D'Herde K 2993066220122142193210.1099/ijs.0.029207-0 · doi ↗ · pubmed ↗
- 4A case of acute gastric mucosal lesions associated with Helicobacter heilmannii infection Helicobacter Yoshimura M Isomoto H Shikuwa S 322326720021239021310.1046/j.1523-5378.2002.00103.x · doi ↗ · pubmed ↗
- 5A case of Helicobacter heilmannii-associated primary gastric mucosa-associated lymphoid tissue lymphoma achieving complete remission after eradication Clin J Gastroenterol Okamura T Iwaya Y Yokosawa S 3845620132618140310.1007/s 12328-012-0355-9 · doi ↗ · pubmed ↗
- 6The relationship between helicobacter pylori infection and nodular antral gastritis in pediatric patients J Natl Med Assoc Yorulmaz A Emiroğlu HH GümüşMD Emiroğlu M 44045011420223576443110.1016/j.jnma.2022.05.011 · doi ↗ · pubmed ↗
- 7Helicobacter pylori chronic gastritis updated Sydney grading in relation to endoscopic findings and H. pylori Ig G antibody: diagnostic methods J Microsc Ultrastruct Hassan TM Al-Najjar SI Al-Zahrani IH Alanazi FI Alotibi MG 167174420163002322410.1016/j.jmau.2016.03.004PMC 6014253 · doi ↗ · pubmed ↗
- 8Helicobacter heilmannii infection: clinical, endoscopic and histopathological features in Japanese patients Pathol Int Okiyama Y Matsuzawa K Hidaka E Sano K Akamatsu T Ota H 3984045520051598221410.1111/j.1440-1827.2005.01844.x · doi ↗ · pubmed ↗