Exploring root canal outcomes and periodontal disease in diabetic patients: A review
Abdo Mohammed Mohammed Abdulrazzaq, Ali Mohammed Alyami, Fayez Hamad Al Aqil, Abdullah Mohammed Al-khomsan, Sulaiman Mana Al Hutaylah, Hamad Mohammed Al khamssan, Meshal Hussain Alhammami

TL;DR
This review shows that diabetic patients have worse root canal outcomes and highlights the need for better treatment strategies.
Contribution
The paper compiles evidence showing diabetes impacts root canal success and periodontal disease outcomes.
Findings
Diabetic patients show significantly worse root canal outcomes compared to non-diabetic individuals.
Periodontal disease is more prevalent and severe in diabetic patients undergoing root canal treatments.
Abstract
This review of 14 studies (2000-2024) highlights a significant link between diabetes and poor root canal outcomes, emphasizing the need for specialized, evidence-based management to improve treatment efficacy in diabetic patients with periodontal diseases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
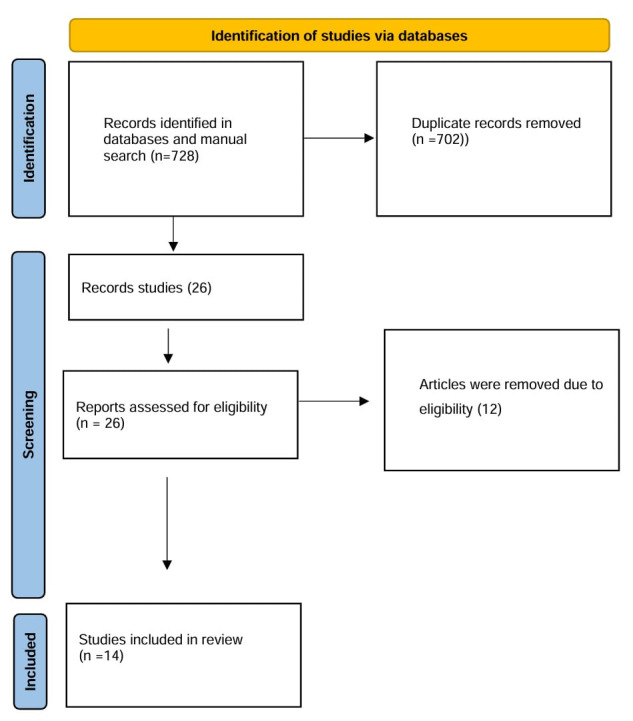 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Endodontics and Root Canal Treatments
Background:
Apical periodontitis (AP), an inflammatory root apex disease, often persists in poorly controlled diabetics due to impaired PMN function and delayed wound healing, leading to more periapical lesions [1]. Poorly controlled diabetes increases susceptibility to oral infections, including apical periodontitis, which correlates with higher endodontic treatment failure rates [2]. Diabetes is a key prognostic factor for root canal outcomes, necessitating better-controlled, long-term clinical trials [3]. Type 2 diabetes is linked to higher apical periodontitis rates and slower healing post-root canal therapy [4]. RCT with apical periodontitis was more prevalent in type 11 diabetics, affecting treatment timing and glycemic control [5]. In diabetics, abnormal glucose levels affect root canal outcomes, leading to more periapical lesions and complications [6]. Therefore, it is of interest to show that exploring root canal outcomes and periodontal disease in diabetic patients underscores the need for tailored treatment strategies, as diabetes may impair healing, increase infection risk and necessitate closer monitoring for complications.
Materials and Methods:
This review examines the evidence on root canal treatment and periodontal diseases in diabetic patients.
Articles identification:
A systematic PRISMA-based search in PubMed, ScienceDirect and Cochrane identified relevant studies on diabetes, root canal and periodontal disease.
Study screening:
The study selection followed PRISMA, with duplicates removed and full-text articles evaluated by two authors for inclusion.
Inclusion:
The review analysed studies from 2000-2024 on root canal treatment and periodontal diseases in diabetic patients.
Exclusion criteria:
Database results were screened, duplicates removed with EndNote and titles/abstracts reviewed to include relevant studies only.
Data extraction process:
Two investigators independently extracted data, resolving conflicts through consensus.
Quality assurance and bias evaluation:
Two authors assessed bias risk using the Hoy tool, focusing on key factors [7].
Ethics and dissemination:
Since this is a systematic review of published literature, no ethical approval was required. Findings were published and presented at conferences.
Results:
A search identified 728 studies; 702 were duplicates. After reviewing, 12 studies were excluded and 14 studies met the inclusion criteria for the final analysis. (Figure 1), (Table 1) and (Table 2).
Explanation:
Smadi (2017) found higher AP prevalence, ET and AP/ET ratio in diabetics (13.5% vs 11.9%, p = 0.001), with poorly controlled DM showing significantly higher AP lesions (p = 0.001). Karolina et al. (2022) reported diabetics had higher AP prevalence post-RCT (OR = 1.51, P < .01) and a threefold increased risk of AP (OR = 3.38, P < .01). Juan et al. (2016) observed higher RFT prevalence with RPLs in diabetics (OR = 1.42, 95% CI = 1.11-1.80, P = 0.0058). Manuele et al. (2014) found no significant differences in success rates (62% test group, 80% control group, p > 0.05). Selen Nihal et al. (2019) showed significant differences in AP and cardiovascular disease between DM and control groups (p < 0.05), but no differences within DM subgroups (p > 0.05). José López et al. (2011) reported higher AP prevalence (OR = 3.9, P = .002) and more root-filled teeth (OR = 2.3, P = .043) in diabetics. Francisco et al. (2020) found T1DM patients had significantly higher RCT (OR = 10.435, P = .000) and AP prevalence (OR = 3.508, P = .011). Patrícia et al. (2012) reported higher AP prevalence in untreated diabetic teeth (10%) vs nondiabetic (7%, P = .03).
Analysis:
Gupta et al. (2020) reported higher AP prevalence in diabetics (OR = 1.42) and clinical studies (OR = 6.36). Liu et al. (2023) found diabetics had higher AP prevalence post-RCT (OR = 1.51, P < .01), with increased risk at the patient level (OR = 3.38, P < .01) and subgroup analysis showed significance (P < .05). Arya et al. (2017) observed reduced periapical scores post-treatment, with diabetics showing less healing (43%) vs. non-diabetics (80%) at 12 months (P < .05). Laukkanen et al. (2019) found RCT success rates were lower in DM patients (73.2%) vs. controls (85.6%) (P = 0.043). José et al. (2021) reported lower RCT success in diabetics (P < .001). Animal studies by Ashraf et al. (2003) showed increased glycemia (P < .001), AP area (P < .05) and lower VEGF (P < .05). Diabetes history was associated with reduced RCT success (P < .01), highlighting the need for tailored endodontic approaches.
Discussion:
The literature consistently shows a significant association between diabetes mellitus, particularly type 2 diabetes (T2DM) and increased prevalence of apical periodontitis (AP). Diabetic patients, especially those with T2DM, experience higher rates of AP compared to non-diabetics, as evidenced by cross-sectional studies (e.g., Smadi, 2017; Selen Nihal et al. 2019) and systematic reviews (Karolina et al. 2022; Juan et al. 2016). This highlights the need for specialized endodontic care for diabetic patients. Diabetes also affects endodontic treatment outcomes, with studies indicating higher rates of root canal treatment (RCT) failure in diabetics. Research by José et al. (2011) and Francisco et al. (2020) shows a higher incidence of AP in root-filled teeth among diabetics. Further studies by Gupta et al. (2020) and Liu et al. (2023) emphasize compromised immune response and chronic inflammation in diabetes, contributing to higher rates of radiolucent periapical lesions. These findings are consistent across diverse regions, including Jordan, Brazil, Lithuania, Portugal and Turkey, reinforcing the robust association between diabetes and AP. Studies using various methodologies converge on similar conclusions regarding the negative impact of diabetes on endodontic outcomes. Diabetes also impairs periapical healing, as demonstrated by Arya et al. (2017) and Laukkanen et al. (2019), with reduced healing and lower success rates in diabetic patients. Additionally, studies like Ashraf et al. (2003) show that diabetic patients with endodontically treated teeth have a higher prevalence of periodontal disease, further complicating treatment outcomes. The clinical implications call for tailored care, including frequent follow-ups, patient education and potentially specialist referrals. However, research limitations, including confounding comorbidities and lack of standardized treatment protocols, suggest the need for more controlled studies and comprehensive patient assessments to improve endodontic care in diabetics.
Conclusion:
This research clarified the adverse effects of root canal treatment and the increased Incidence of apical periodontitis (AP) in diabetic patients. By integrating and critically assessing existing evidence, the study identified key knowledge gaps and provided valuable insights into the challenges diabetic individuals face during root canal procedures. This synthesis was essential in developing evidence-based guidelines for managing diabetic patients needing root canal treatment. The findings underscore the necessity of customized treatment planning, including risk assessment, tailored treatment plans, comprehensive pre- and post-treatment care, on-going education and further research. Additionally, they emphasize the importance of addressing diabetes-specific complications to enhance clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lima S.M.F Int Endod J.2013467002344200310.1111/iej.12072 · doi ↗ · pubmed ↗
- 2Gupta A Int Endod J. 20205314723265419110.1111/iej.13366 · doi ↗ · pubmed ↗
- 3Nagendrababu V Int Endod J. 2020534553172124310.1111/iej.13253 · doi ↗ · pubmed ↗
- 4Budreikaite K Stomatologija. 20222410037154421 · pubmed ↗
- 5López-López JJ Endod. 2011375982149665510.1016/j.joen.2011.01.002 · doi ↗ · pubmed ↗
- 6Fouad A.F Burleson JJ Am Dent Assoc. 2003134431255595610.14219/jada.archive.2003.0016 · doi ↗ · pubmed ↗
- 7Hoy DJ Clin Epidemiol. 2012659342274291010.1016/j.jclinepi.2011.11.014 · doi ↗ · pubmed ↗
- 8Smadi LJ Contemp Dent Pract. 2017183582851227210.5005/jp-journals-10024-2046 · doi ↗ · pubmed ↗