Noonan syndrome and parasternal pericardiocentesis
Pitt O. Lim, May H. Ohn

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
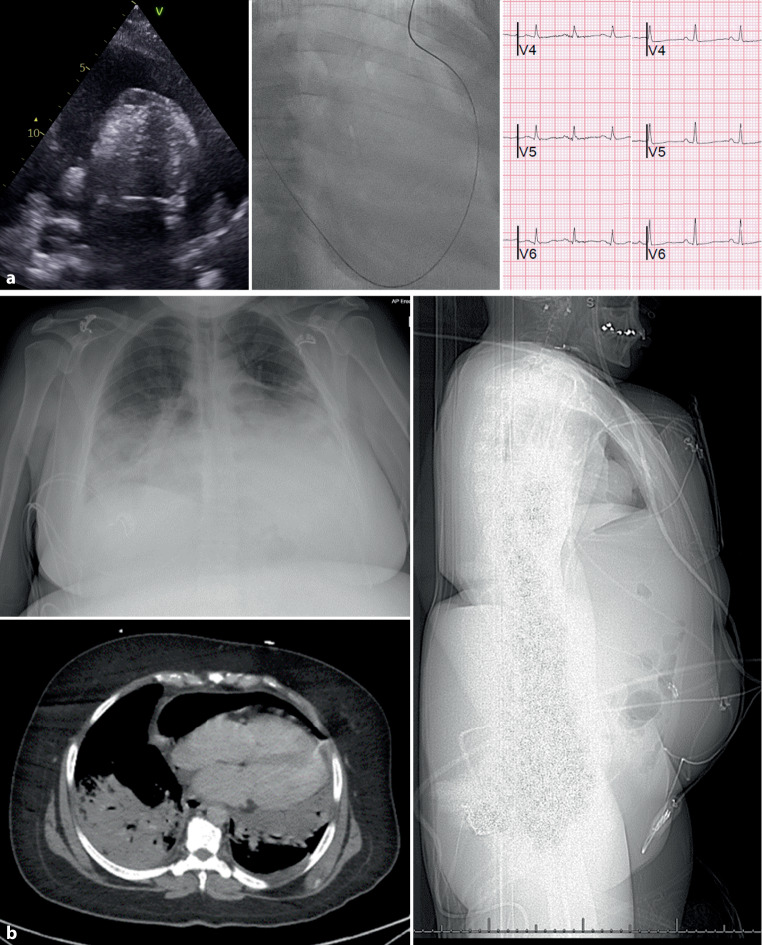 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProtein Tyrosine Phosphatases · Pericarditis and Cardiac Tamponade · Eosinophilic Disorders and Syndromes
A 47-year-old woman with Noonan syndrome and pneumococcal pneumonia presented with cough, breathlessness, and hypotension caused by cardiac tamponade (Fig. 1a). Due to associated abdominal organomegaly, she underwent the recently described two-step parasternal pericardiocentesis approach [1]. The pericardial pressure was 17 mm Hg (normal < 4 mm Hg). About 1 L of serosanguinous fluid was withdrawn, resulting in immediate symptomatic relief and a doubling of the electrocardiographic R‑wave amplitude—an intuitive phenomenon not widely reported in the medical literature. The drain was removed the following day and a chest X‑ray showed pneumopericardium (Fig. 1b). Her CT scan confirmed the diagnosis and additionally revealed right basal lung consolidation and hepatosplenomegaly, which made subcostal pericardiocentesis challenging. Although there are no published cases of Noonan syndrome and percutaneous pericardiocentesis. The mechanism of pneumopericardium remains unclear but may result from pneumonic intrathoracic suction or potentially air leakage caused by the drain slipping out, exposing a side hole which is 7.5 cm from the tip [2]. Her follow-up echocardiogram however showed no tamponade physiology.Fig. 1a Left Echocardiogram showing the large pericardial effusion causing cardiac tamponade. Middle Guidewire in the pericardial space using the 2‑step parasternal pericardiocentesis technique. Right Doubling of the electrocardiographic R wave amplitude following drainage of the pericardial effusion. b Top left Chest X‑Ray revealing pneumopericardium. Bottom left Coronal CT Scan demonstrating pneumopericardium, residual effusion, in addition to left basal lung consolidation. *Right *Sagittal CT Scan confirming hepatosplenomegaly, making subcostal pericardiocentesis inadvisable
The reference list from the paper itself. Each links out to its DOI / PubMed record.