Ambient Solar Radiation Predicts Psoriasis Treatment Intensity
Brad R. Woodie, Alan B. Fleischer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
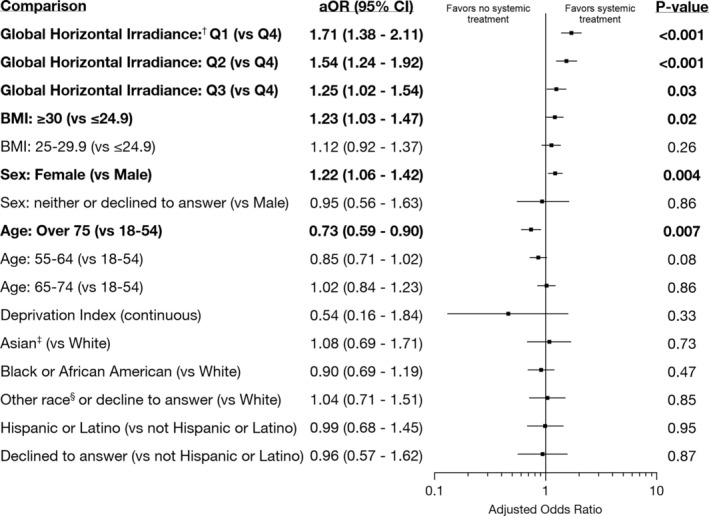 FIGURE 1
FIGURE 1| Characteristic | No systemic treatment or phototherapy ( | Systemic treatment or phototherapy ( |
|---|---|---|
| Deprivation Index, mean (SD) | 0.31 (0.06) | 0.30 (0.05) |
| Global horizontal irradiance: | 976 (75.9) | 310 (24.1) |
| Global horizontal irradiance: Q2 | 1179 (79.2) | 309 (21.8) |
| Global horizontal irradiance: Q3 | 887 (81.0) | 208 (19.0) |
| Global horizontal irradiance: Q4 | 1109 (84.7) | 201 (15.3) |
| Age: 18–54 | 1212 (78.4) | 334 (21.6) |
| Age: 55–54 | 877 (78.4) | 242 (21.6) |
| Age: 65–74 | 1200 (81.0) | 281 (19.0) |
| Age: > 75 | 862 (83.4) | 171 (16.6) |
| BMI: ≤ 24.9 kg/m2 | 961 (82.0) | 211 (18.0) |
| BMI: 25–29.9 kg/m2 | 1274 (80.7) | 304 (19.3) |
| BMI: ≥ 30 kg/m2 | 1916 (78.9) | 513 (21.1) |
| Female sex | 2299 (78.5) | 629 (21.5) |
| Male sex | 1752 (82.2) | 379 (17.8) |
| Other sex or decline to answer | 100 (83.3) | 20 (16.7) |
| Race | 96 (79.3) | 25 (20.7) |
| Race: Black or African American | 308 (80.6) | 74 (19.4) |
| Race: Other | 741 (80.6) | 178 (19.4) |
| Race: White | 3006 (80.0) | 751 (20.0) |
| Ethnicity: Hispanic or Latino | 545 (80.4) | 133 (19.6) |
| Ethnicity: Not Hispanic or Latino | 3424 (80.0) | 854 (20.0) |
| Ethnicity: Decline to answer | 182 (81.6) | 41 (18.4) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClimate Change and Health Impacts · Skin Protection and Aging · Psoriasis: Treatment and Pathogenesis
Introduction
1
Observations of seasonal variation in psoriasis severity (worsening in winter and improving in summer) suggest a beneficial effect of ambient solar radiation [1, 2]. Additionally, “climate therapy” using intentional sunlight exposure reduces psoriasis severity [3]. Interestingly, an analysis of psoriasis clinical trial participants by Okun and Okun [4] found no relationship between psoriasis severity and the ambient ultraviolet radiation at investigator sites. Also, Jacobson et al. [5] compared the psoriasis prevalence in extant studies by the mean country latitude and found no substantial correlation. Using a diverse sample of the United States, our study assessed the association of annual local solar radiation with psoriasis treatment intensity.
Methods
2
We analyzed de‐identified participant data from the National Institutes of Health's All of Us Research Program version 7, which includes data from 2017 to 2022. Seven thousand seven hundred forty eight participants with a diagnosis of psoriasis were identified. To reduce the likelihood of patients requiring systemic immunosuppressive treatments for other conditions, we excluded participants with diagnoses of psoriatic arthritis, rheumatoid arthritis, systemic lupus erythematosus, atopic dermatitis, uveitis, Crohn's disease, and ulcerative colitis. Our final cohort included 5179 participants after excluding participants with missing values for 3‐digit ZIP code or body mass index (BMI) as obtained from the participant's electronic health record. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Treatment intensity was assessed by the presence or absence of a systemic psoriasis treatment or phototherapy (Table S1). Mean annual global horizontal irradiance (GHI) data (1998–2016) for the contiguous United States by ZIP code was obtained from the National Renewable Energy Laboratory [6]. Deprivation index (a composite score calculated by the All of Us Program using measures of poverty, education, housing, and lack of health insurance at the census tract level) was included to control for confounding related to differences in access to care.
Descriptive statistics of mean and standard deviation or frequency and percent were calculated. GHI was divided into quartiles: under 3.97 kWh/m^2^/day (Quartile 1, e.g. Seattle, Washington), 3.97 to 4.05 (Quartile 2, e.g. Chicago, Illinois), 4.05 to 4.92 (Quartile 3, e.g. Atlanta, Georgia), and over 4.92 (Quartile 4, e.g. Los Angeles, California). Multivariable logistic regression compared treatment odds by participant ZIP code GHI, adjusting for deprivation index, age, BMI, sex assigned at birth (hereafter “sex”), race, and ethnicity. Significance was set at two‐tailed p < 0.05, and analysis was performed using SAS Studio in the All of Us Researcher Workbench.
Results
3
Of the 5179 participants with psoriasis in the study, 1028 received systemic treatment or phototherapy (Table 1). Lower GHI of the participants' ZIP code was associated with higher odds of receiving systemic treatment or phototherapy (Figure 1). Obesity and female sex were also associated with higher odds of systemic treatment or phototherapy. Age over 75 was associated with lower odds of systemic therapy or phototherapy. We did not find an association between deprivation index, race, or ethnicity and treatment intensity.
Multivariable logistic regression for the odds of receiving a psoriasis systemic therapy or phototherapy. †Quartile 1 (Q1): Global horizontal irradiance (GHI) under 3.97 kWh/m2/day (e.g., Seattle, Washington). Q2: GHI of 3.97 to 4.05 (e.g., Chicago, Illinois). Q3: 4.05 to 4.92 (e.g., Atlanta, Georgia). Q4: Over 4.92 (e.g., Los Angeles, California). ‡Race and ethnicity were obtained from self‐report and were included in this analysis as a goal of All of Us to collect and report data from a diverse group of participants. §“Other” races included American Indian or Alaskan Native, Middle Eastern or North African, Native Hawaiian or Other Pacific Islander, and more than one population.
Discussion
4
Our study shows that lower levels of ambient solar radiation are associated with higher odds of receiving systemic therapy or phototherapy for psoriasis, with these treatments serving as possible indicators of more severe disease. The lack of association between severity and ultraviolet radiation seen by Okun and Okun [4] may have been due to clinical trial participants having stable moderate‐to‐severe psoriasis and being instructed to limit their environmental ultraviolet radiation exposure. Of note, the study by Jacobson et al. [5] of latitude and psoriasis prevalence excluded the United States and China due to the range of latitudes spanned by these countries. Solar irradiance also varies with factors beyond latitude, such as altitude and cloud coverage [6].
The associations of obesity, sex, and age with treatment seen in our study align with prior research. Obesity is associated with psoriasis severity, and weight loss leads to a reduction in the Psoriasis Area and Severity Index (PASI) [7]. Although male sex is associated with higher PASI scores, female sex is associated with a greater likelihood of receiving biologic treatment [8]. Increasing age is associated with a lower intensity of psoriasis treatment [9]. No significant association between the deprivation index and treatment status is encouraging from a health equity perspective.
Limitations include the All of Us Program being a volunteer‐based sample of only the United States. Also, we cannot account for people's movement to areas of different solar irradiance or outdoor activities that increase ultraviolet radiation exposure. Clothing coverage is another determinant of personal solar radiation exposure [10] for which we could not account. Nonetheless, we add to the literature on environmental components of psoriasis by suggesting that lower ambient solar radiation is associated with more frequent systemic psoriasis treatment.
Author Contributions
B.R.W. and A.B.F. authors were involved in conceptualization, methodology, formal analysis, writing, and editing. B.R.W. performed the data curation and prepared the original draft.
Ethics Statement
No ethical approval was needed for this study because participant data are deidentified.
Conflicts of Interest
A.B.F. is a consultant for Bluefin and Incyte (fees). He is an investigator for Amgen, Bayer, Biogen, CellDex, Galderma, Incyte, Leo, and UCB (research support). He is a speaker for Imedic Healthcare Solutions (Hyderabad India). B.R.W. declares no conflicts of interest.
Supporting information
Table S1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. L. Pascoe and A. B. Kimball , “Seasonal Variation of Acne and Psoriasis: A 3‐Year Study Using the Physician Global Assessment Severity Scale,” Journal of the American Academy of Dermatology 73, no. 3 (2015): 523–525, 10.1016/j.jaad.2015.06.001.26282801 · doi ↗ · pubmed ↗
- 2W. A. James , M. Zaino , S. R. Feldman , and A. B. Fleischer , “Letter to the Editor: Does Ambient Ultraviolet Radiation Affect Psoriasis Severity,” Journal of Psoriasis and Psoriatic Arthritis 8, no. 1 (2023): 5–6, 10.1177/24755303221131255.39296951 PMC 11361478 · doi ↗ · pubmed ↗
- 3L. T. N. Nilsen , E. Søyland , and A. L. Krogstad , “Estimated Ultraviolet Doses to Psoriasis Patients During Climate Therapy,” Photodermatology, Photoimmunology & Photomedicine 25, no. 4 (2009): 202–208, 10.1111/j.1600-0781.2009.00443.x.19614899 · doi ↗ · pubmed ↗
- 4T. S. D. Okun and M. M. Okun , “No Evidence That Variations in Ambient Solar Ultraviolet Radiation and Psoriasis Severity Are Associated,” Journal of Psoriasis and Psoriatic Arthritis 7, no. 2 (2022): 67–70, 10.1177/24755303221079810.39296826 PMC 11361520 · doi ↗ · pubmed ↗
- 5C. C. Jacobson , S. Kumar , and A. B. Kimball , “Latitude and Psoriasis Prevalence,” Journal of the American Academy of Dermatology 65, no. 4 (2011): 870–873, 10.1016/j.jaad.2009.05.047.21920244 · doi ↗ · pubmed ↗
- 6M. Sengupta , Y. Xie , A. Lopez , A. Habte , G. Maclaurin , and J. Shelby , “The National Solar Radiation Data Base (NSRDB),” Renewable and Sustainable Energy Reviews 89 (2018): 51–60, 10.1016/j.rser.2018.03.003. · doi ↗
- 7P. Jensen , C. Zachariae , R. Christensen , et al., “Effect of Weight Loss on the Severity of Psoriasis: A Randomized Clinical Study,” JAMA Dermatology 149, no. 7 (2013): 795–801, 10.1001/jamadermatol.2013.722.23752669 · doi ↗ · pubmed ↗
- 8C. P. Hernández‐Fernández , G. Carretero , R. Rivera , et al., “Effect of Sex in Systemic Psoriasis Therapy: Differences in Prescription, Effectiveness and Safety in the BIOBADADERM Prospective Cohort,” Acta Dermato‐Venereologica 101, no. 1 (2021): adv 00354, 10.2340/00015555-3711.33269405 PMC 9309850 · doi ↗ · pubmed ↗