A rare mediastinal mass treated by submucosal tunneling endoscopic resection
Weizhao Wang, Mengxian Ju, Jun Liu, Pinghong Zhou, Lu Wang, Chaowu Chen, Chao Sun

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
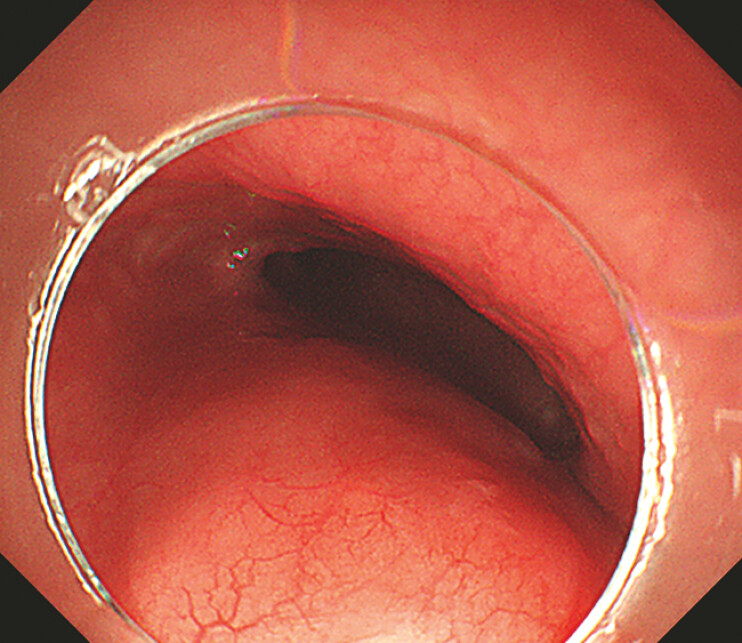 Fig. 1
Fig. 1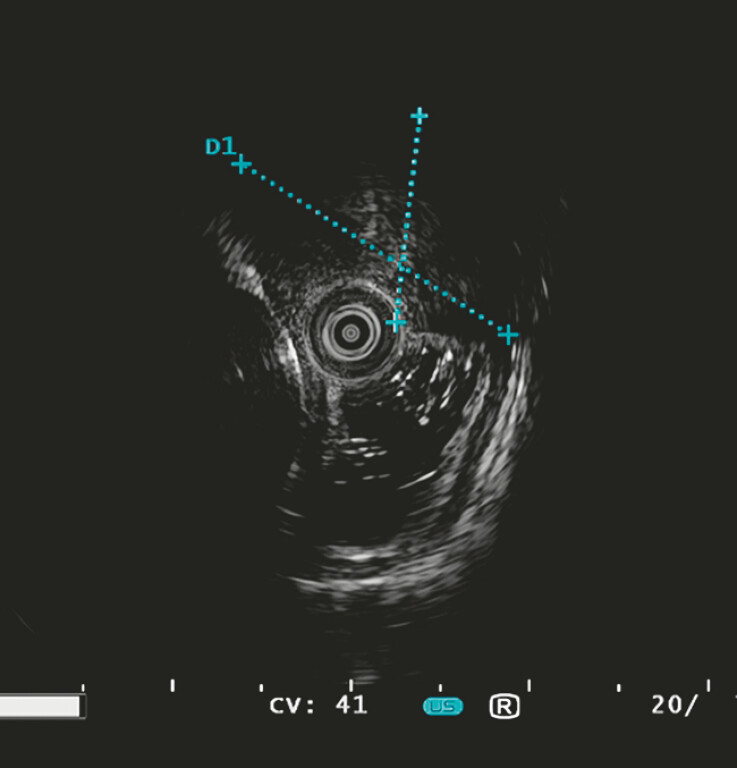 Fig. 2
Fig. 2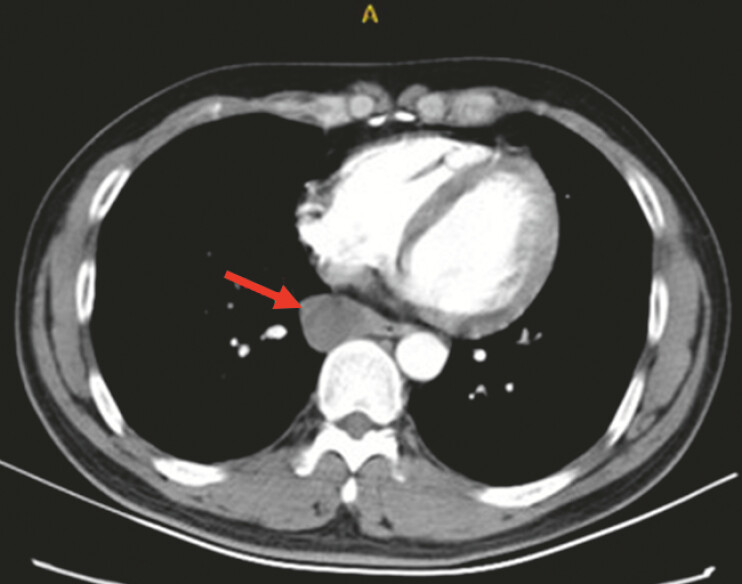 Fig. 3
Fig. 3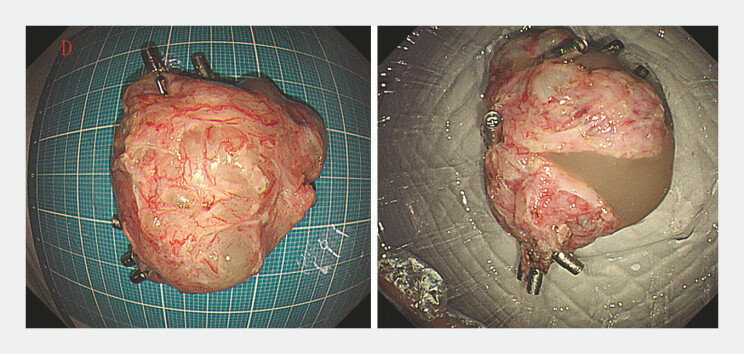 Fig. 4
Fig. 4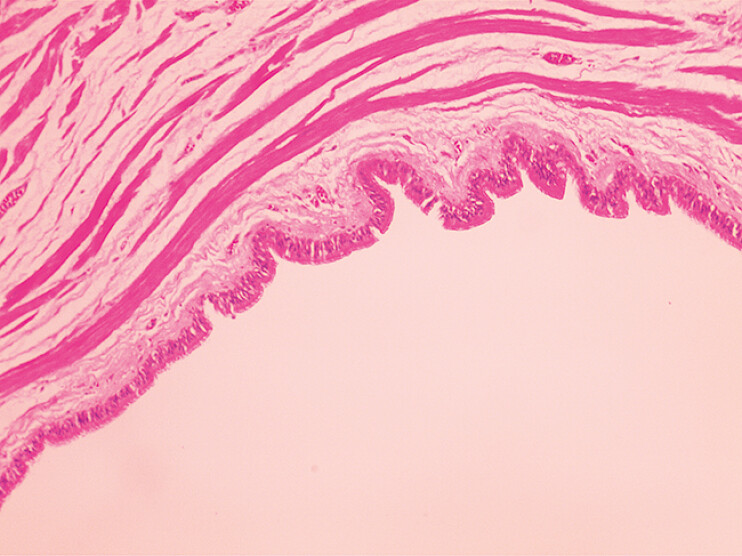 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Metastasis and carcinoma case studies
A 46-year-old man presented with a sensation of obstruction during eating and gastroscopy revealed a submucosal mass in the lower esophagus. The mass was located about 35–38 cm from the incisors, had a smooth surface, and measured 3.0 × 5.0 cm ( Fig. 1 ). Endoscopic ultrasound examination revealed a hypoechoic mass protruding into the esophageal and mediastinal cavities, which was poorly demarcated from the muscularis propria, and was considered to have originated from either the muscularis propria or the mediastinum as a space-occupying lesion ( Fig. 2 ). A enhanced computed tomography scan showed a hypodense mass of homogeneous density adjacent to the lower esophagus, about 3.0 cm in diameter, poorly demarcated from the esophagus and mediastinum, with unremarkable enhancement ( Fig. 3 ). The patient’s full blood count, liver, renal, and coagulation function, and tumor markers were within reference values. The preoperative diagnosis was of “submucosal tumor of the esophagus” or “mediastinal occupation.” Endoscopic resection (submucosal tunneling endoscopic resection [STER]) was performed after obtaining consent from the patient.
Gastroscopic image showing a mass with a smooth surface in the esophageal wall, located 35–38 cm from the incisors.
Endoscopic ultrasound image showing a hypoechoic mass protruding into the esophageal and mediastinal cavities, which was poorly demarcated from the muscularis propria.
Enhanced computed tomography scan showing a hypodense mass of homogeneous density adjacent to the lower esophagus, about 3.0 cm in diameter, poorly demarcated from the esophagus and mediastinum, with unremarkable enhancement.
After establishing a submucosal tunnel to reach the tumor site, we found that the mass was located at a deeper level. Therefore, we incised the muscularis propria and the outer esophagus into the mediastinum to completely remove the mass. Intraoperatively, mucus and jelly-like fluid were seen oozing from the mass. The tumor was successfully removed under gastroscopic guidance ( Video 1 ), with the resected specimen measuring 4.0 × 5.0 cm ( Fig. 4 ). Histopathologic examination revealed the tumor to be a cyst with a wall composed of fibrous tissue lined with ciliated columnar epithelium, and a mediastinal cyst was diagnosed ( Fig. 5 ). The patient remained asymptomatic over 12 months of follow-up.
A mediastinal cystic mass is successfully resected using the submucosal tunneling endoscopic resection procedure, with only minor bleeding experienced during the procedure.Video 1
Photographs of the resected specimen, which measured 4.0 × 5.0 cm and was a cystic mass containing a large amount of mucus and jelly-like fluid.
Histopathologic appearance showing that the tumor was a cyst, with its wall composed of fibrous tissue lined with ciliated columnar epithelium.
Mediastinal cysts are cystic benign lesions that occur in the mediastinum, grow slowly, rarely become malignant, and are treated mainly by surgery 1 2 3 . To the best of our knowledge, this if the first report of a mediastinal cyst being treated by gastroscopy in the English literature. This case reminds endoscopists that mediastinal cysts can protrude into the lumen of the esophagus and may be misdiagnosed as submucosal tumors of the esophagus. Although imaging and ultrasound can provide some information, the final diagnosis usually depends on histopathologic examination of the resected specimen, and our approach provides a new idea for minimally invasive treatment of mediastinal cysts.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Le Pimpec-Barthes F Cazes A Bagan P Mediastinal cysts: clinical approach and treatment Rev Pneumol Clin 201066526210.1016/j.pneumo.2009.12.00920207297 · doi ↗ · pubmed ↗
- 2Cooley-Rieders K Van Haren RM Mediastinal thymic cysts: a narrative review Mediastinum 202263310.21037/med-22-2536582977 PMC 9792833 · doi ↗ · pubmed ↗
- 3Gokce A Valiyev E Turk MS Single-center experience of management of mediastinal cyst – a case series Surg J (N Y)20228 e 141e 14410.1055/s-0042-174942935783027 PMC 9246518 · doi ↗ · pubmed ↗