Metastatic non-small cell lung cancer with BRCA2 mutation—a therapeutic challenge
Saad Salim Naviwala, Waqas Ahmed Khan, Daania Shoaib, Taha Nafees, Muzammil Shakeel, Yasmin Abdul Rashid

TL;DR
A patient with lung cancer and a BRCA2 mutation had poor outcomes with PARP inhibitor therapy, suggesting more research is needed for effective treatments.
Contribution
This case study explores the therapeutic challenge of BRCA2-mutated non-small cell lung cancer and highlights the need for further research.
Findings
The patient with BRCA2-mutated lung cancer did not respond to second-line Olaparib therapy.
BRCA mutations in non-small cell lung cancer are rare but may represent a potential therapeutic target.
Further large-scale studies are needed to improve treatment outcomes for BRCA-mutated NSCLC.
Abstract
Non-small cell lung cancer, specifically adenocarcinoma, is amenable to targeted therapy for genetic alterations. The role of BRCA mutations in pathogenesis and the efficacy of PARP inhibitors in these cases are still unclear. This case involves a 61-year-old male patient with a past history of Hodgkin’s Lymphoma and a heavy smoking history who developed lung adenocarcinoma and was found to have a BRCA2 mutation. Following disease progression on first-line chemotherapy and a detailed case discussion in the multidisciplinary team meeting, second-line Olaparib was started, but the patient's condition worsened rapidly, and he died from the illness. This case highlights the fact that BRCA mutations, though less common, are a potential target that should be explored further. Further large-scale studies are crucial to understanding and improving treatment outcomes for patients with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
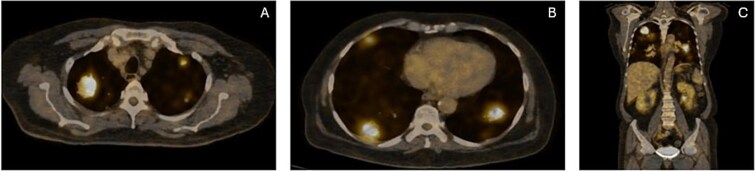 Figure 1
Figure 1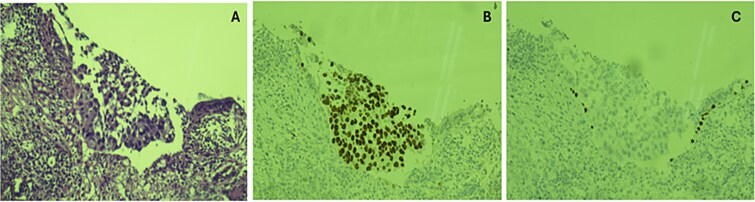 Figure 2
Figure 2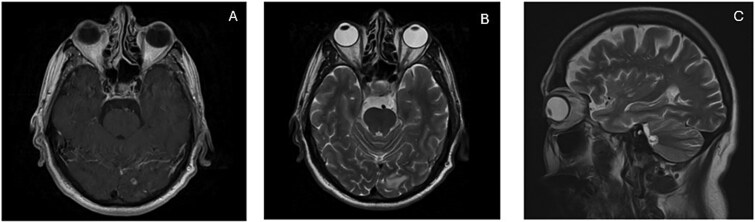 Figure 3
Figure 3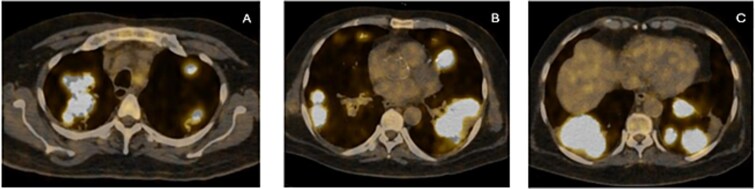 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · BRCA gene mutations in cancer · PARP inhibition in cancer therapy
Introduction
Lung cancer is the second most frequently diagnosed cancer worldwide and remains a significant global health concern. It accounted for about 2.2 million new cases and 1.8 million deaths in 2020 [1]. Since it is the organ that is most exposed to exogenous carcinogens, cancers that arise often demonstrate very high somatic mutation loads [2]. More than half of all lung adenocarcinomas have been found to carry at least one mutation. Recent advancements in identifying and targeting oncogenic driver mutations have significantly changed the standard of care and improved outcomes for non-small cell lung carcinoma (NSCLC), especially adenocarcinomas [3]. Next Generation Sequencing (NGS) is now increasingly utilized, allowing the detection of a wide range of somatic and germline mutations involved in the tumorigenesis of NSCLC [4]. Defects in the breast cancer tumor suppressor gene family (BRCA 1 & 2) are linked to several types of cancers and are well known to operate via the DNA homologous recombination and reparation mechanism. Poly Adenosine Diphosphate-Ribose Polymerase (PARP) inhibitors block DNA repair and lead to the accumulation of DNA breaks during the replication process with impaired repair and eventual cell death [5]. Although lung cancer is not typically associated with BRCA mutations, 1% of lung adenocarcinomas can harbor such alterations, with BRCA2 being the predominant subtype [6].
Here, we present the case of metastatic lung adenocarcinoma with progressive disease found to have a BRCA2 mutation on genetic testing.
Case presentation
A 61-year-old gentleman with diabetes mellitus, hypertension, coronary artery disease, and an ECOG performance status score of 2 presented in March 2023 with a persistent cough, copious sputum, and a 20 kg weight loss over three months. He had a history of Hodgkin lymphoma treated in 1998, but no reliable records were available. He was an active smoker with a 50-pack-year history. His sister had non-Hodgkin’s lymphoma. He was of average build with normal vital signs and an unremarkable systemic examination. He brought along initial investigations from a different healthcare facility, all within reference ranges. However, a chest X-ray revealed multiple nodular densities bilaterally, with a large deposit in the right upper lobe raising a suspicion of malignancy.
Based on this, he was advised further diagnostic workup. A PET scan demonstrated multiple hypermetabolic lesions in both lung fields, with the largest in the right upper lobe having an SUVmax of 10.1, and regional lymphadenopathy (Fig. 1). An image-guided biopsy of the right upper lobe mass was carried out, and histopathology revealed adenocarcinoma of the lung (TTF-1 positive, p40 negative), as demonstrated in Fig. 2. He was advised next-generation sequencing (NGS) at diagnosis, but due to affordability issues, we had to go for a limited panel of EGFR and ALK testing only, both of which turned out to be negative. Staging was completed with an MRI brain with contrast, which revealed a solitary occipital lobe deposit measuring 6.5 × 4.2 mm, with surrounding vasogenic edema (Fig. 3).
(A, B & C) Axial and coronal sections on the PET scan revealing bilateral pulmonary deposits.
(A) Section showing nest of neoplastic cells with pleomorphic nuclei and eosinophilic cytoplasm. (B) TTF 1 showing nuclear positivity. (C) Lack of expression of p40 in tumor cells.
(A & B) MRI brain with and without contrast demonstrating occipital lobe deposit with surrounding edema. (C) Progressive disease with new deposit at cerebellar vermis.
As first-line therapy, he was started on a combination of carboplatin (AUC 4) and pemetrexed 400 mg/m^2^. A PET scan after four cycles showed partial metabolic response, while MRI brain showed near resolution of the cerebral deposit. After completing six cycles of the combination regimen, he was switched to pemetrexed maintenance at 500 mg/m^2^. Disease assessment scans after two cycles of maintenance therapy revealed progression in the primary tumor along with new hepatic and brain deposits (Fig. 4). He underwent stereotactic radiosurgery for the brain deposit. While awaiting the report of next-generation sequencing (NGS) sent on liquid biopsy, he was started on carboplatin AUC 2 and paclitaxel 80 mg/m^2^ every week. FoundationOne NGS testing revealed a BRCA2 N1544fs*24 genomic alteration.
(A, B & C) Axial sections on PET showing gross disease progression after first-line treatment.
The multidisciplinary team discussed further care, and he was started on Olaparib 300 mg twice daily. However, his condition worsened rapidly, and he was hospitalized with pleural effusion and hypoxic respiratory failure. He was eventually transitioned to best supportive care and died in October 2023.
Discussion
Over the past decade, notable advances have been observed in managing lung cancer, particularly non-small cell lung cancer (NSCLC). Despite significant improvements, the all-stage five-year survival rate is 23%, and less than 10% for metastatic disease at presentation [7]. Genetic alterations, including but not limited to EGFR, KRAS, ALK, MET, and ROS1, are crucial for selecting appropriate treatments, understanding resistance, and have shown promising outcomes with targeted therapy [8].
BRCA1 and BRCA2 tumor suppressor genes are primarily linked with hereditary breast and ovarian cancers and with other malignancies to a lesser extent. BRCA mutations have diagnostic and therapeutic applications in breast and ovarian cancers, including genetic testing, improved screening, and targeted therapies such as PARP inhibitors. However, the association and impact of BRCA mutations in lung cancer, particularly NSCLC, have not been as comprehensively studied [9]. Several case reports have documented varied responses in patients receiving PARP inhibitors for lung cancer with BRCA mutations. A retrospective study by Fang et al. showed that Chinese patients with BRCA1/BRCA2 mutations had a median progression-free survival (PFS) of 6 months with PARP inhibitors after multiple lines of therapy [10].
In our report, the patient did not receive therapy targeting the BRCA mutation beyond two weeks due to a worsening condition and thus was not assessed for response. Although data are limited, PARP inhibitors appear to be a viable option for patients who have progressed on or are unable to receive chemotherapy and do not have other targetable alterations aside from a BRCA mutation. Several case reports show a PFS of 6 to 10 months using PARP inhibitors in this setting.
Further research into the implications of BRCA mutations and the response to therapies such as PARP inhibitors and platinum-based chemotherapy in lung cancer is essential to broaden the therapeutic options and potentially improve patient outcomes. Additionally, it is crucial to determine whether somatic BRCA mutations identified in lung cancer warrant genetic counselling, reflex testing for germline mutations, and family screening to ensure comprehensive patient management and preventive care for relatives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. 10.3322/caac.21660.33538338 · doi ↗ · pubmed ↗
- 2La Fleur L, Falk-Sörqvist E, Smeds P. et al. Mutation patterns in a population-based non-small cell lung cancer cohort and prognostic impact of concomitant mutations in KRAS and TP 53 or STK 11. Lung Cancer 2019;130:50–8. 10.1016/j.lungcan.2019.01.003.30885352 · doi ↗ · pubmed ↗
- 3Liu S-YM, Zheng M-M, Pan Y. et al. Emerging evidence and treatment paradigm of non-small cell lung cancer. J Hematol Oncol 2023;16:11–12. 10.1186/s 13045-023-01436-2.PMC 1010854737069698 · doi ↗ · pubmed ↗
- 4Cainap C, Balacescu O, Cainap SS. et al. Next generation sequencing Technology in Lung Cancer Diagnosis. Biol (Basel) 2021;10:3–10. 10.3390/biology 10090864.PMC 846799434571741 · doi ↗ · pubmed ↗
- 5Tutt AN, Lord CJ, Mc Cabe N. et al. Exploiting the DNA repair defect in BRCA mutant cells in the design of new therapeutic strategies for cancer. Cold Spring Harb Symp Quant Biol 2005;70:139–48. 10.1101/sqb.2005.70.012.16869747 · doi ↗ · pubmed ↗
- 6Hu X, Yang D, Li Y. et al. Prevalence and clinical significance of pathogenic germline BRCA 1/2 mutations in Chinese non-small cell lung cancer patients. Cancer Biol Med 2019;16:556–64. 10.20892/j.issn.2095-3941.2018.0506.31565484 PMC 6743617 · doi ↗ · pubmed ↗
- 7Bailey H, Lee A, Eccles L. et al. Treatment patterns and outcomes of patients with metastatic non-small cell lung cancer in five European countries: a real-world evidence survey. BMC Cancer 2023;23:603. 10.1186/s 12885-023-11074-z.37386452 PMC 10311888 · doi ↗ · pubmed ↗
- 8Fois SS, Paliogiannis P, Zinellu A. et al. Molecular epidemiology of the main Druggable genetic alterations in non-small cell lung cancer. Int J Mol Sci 2021;22:612. 10.3390/ijms 22020612.33435440 PMC 7827915 · doi ↗ · pubmed ↗