Impact of selegiline on 123I-meta-iodobenzylguanidine myocardial scintigraphy
Katsuya Nishida

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
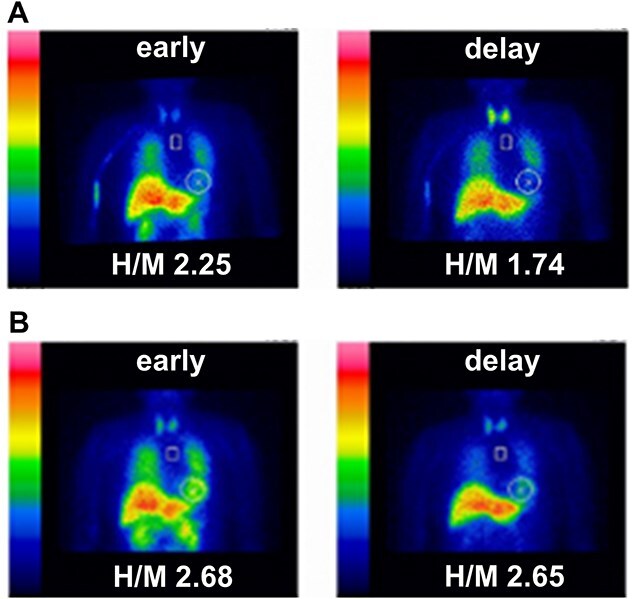 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Advanced MRI Techniques and Applications · Medical Imaging Techniques and Applications
73-year-old female with hypertension, but no history of diabetes or cardiac disease, presented with a two-year history of progressive left-dominant parkinsonism, characterized by left-sided rigidity, bradykinesia, and mild constipation. Head magnetic resonance imaging revealed no significant abnormalities, and dopamine transporter single photon emission computed tomography showed decreased accumulation. The patient was initially diagnosed with Parkinson’s disease (PD) and treated with selegiline, a monoamine oxidase B (MAO-B) inhibitor. Selegiline is used in the management of PD to improve motor symptoms by inhibiting MAO-B, thereby increasing dopamine concentration in the brain. ^123^I-meta-iodobenzylguanidine (MIBG) myocardial scintigraphy under selegiline treatment demonstrated decreased cardiac uptake and heart-to-mediastinum (H/M) ratio (early value 2.25 and delay value 1.74; the cut-off value for the H/M ratio was 2.20 [1]), consistent with PD (Fig. 1A). The H/M ratio was calculated by dividing the average heart count by the average mediastinum count. Discontinuation of selegiline led to the normalization of the H/M ratio (early value 2.68 and delay value 2.65), and the appearance of cerebellar ataxia and dysuria led to a change in the clinical diagnosis to multiple system atrophy (MSA) (Fig. 1B).
MIBG myocardial scintigraphy has been widely validated as a tool for differentiating PD from MSA due to its ability to detect cardiac sympathetic denervation in PD, which is typically absent in MSA [2, 3]. However, the results can be affected by various medications [4]. While some studies have investigated the effects of medications on MIBG scintigraphy, no previous reports have specifically addressed the impact of selegiline on the H/M ratio. To our knowledge, this is the first report describing the impact of selegiline on MIBG myocardial scintigraphy. This study implies that selegiline may decrease the H/M ratio and impact the accuracy of clinical diagnosis, especially in cases of atypical parkinsonism such as MSA. Theoretically, there is no decrease of the H/M ratio in MSA, thus resulting in false-positive under selegiline treatment. Accurate clinical diagnosis is important because the prognoses of Parkinson's disease and MSA are different. Verifying concurrent medications is crucial before MIBG myocardial scintigraphy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nakajima K, Matsumoto N, Kasai T. et al. Normal values and standardization of parameters in nuclear cardiology: Japanese Society of Nuclear Medicine working group database. Ann Nucl Med 2016;30:188–99. 10.1007/s 12149-016-1065-z.26897008 PMC 4819542 · doi ↗ · pubmed ↗
- 2Matsubara T, Kameyama M, Tanaka N. et al. Autopsy validation of the diagnostic accuracy of 123I-Metaiodobenzylguanidine myocardial scintigraphy for lewy body disease. Neurology 2022;98:e 1648–59. 10.1212/WNL.0000000000200110.35256483 PMC 9052572 · doi ↗ · pubmed ↗
- 3Orimo S, Ozawa E, Nakade S. et al. 123I-metaiodobenzylguanidine myocardial scintigraphy in Parkinson's disease. J Neurol Neurosurg Psychiatry 1999;67:189–9410.1136/jnnp.67.2.189.10406987 PMC 1736461 · doi ↗ · pubmed ↗
- 4Jacobson AF, Travin MI. Impact of medications on m IBG uptake, with specific attention to the heart: comprehensive review of the literature. J Nucl Cardiol 2015;22:980–9310.1007/s 12350-015-0170-z.25975946 · doi ↗ · pubmed ↗