Gastric Tropism: Localized Gastric Amyloidosis Presenting as Gastrointestinal Bleeding
Nader Mekheal, Lefika Bathobakae, Alisa Farokhian, Yana Cavanagh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
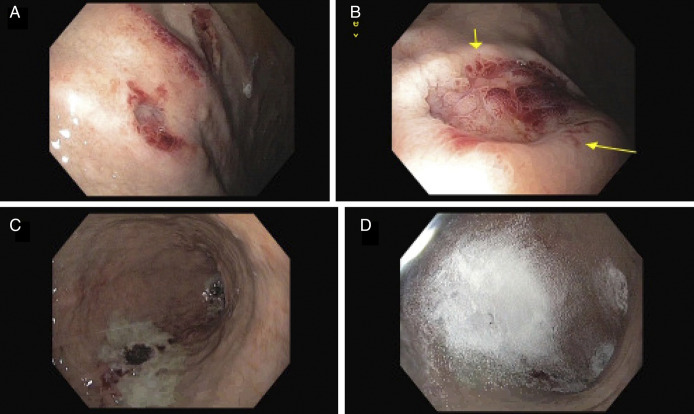 Figure 1
Figure 1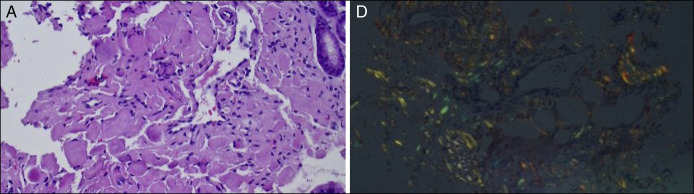 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Parathyroid Disorders and Treatments · Dermatological and Skeletal Disorders
CASE REPORT
A 78-year-old woman with a history of hypertension, chronic constipation, and diverticulosis presented to the emergency department complaining of coffee-ground emesis and dark stools for 1 day. In the emergency department, the patient was tachycardic but hemodynamically stable. Triage laboratory results revealed hemoglobin of 7.6 g/dL, which improved to 9.4 g/dL after 2 units of packed red blood cells. A computed tomography angiogram of the abdomen and pelvis showed an area of contrast pooling in the jejunum, concerning for active bleeding. The radiologist concluded that it was an artifact from the inferior vena cava filter.
Esophagogastroduodenoscopy showed diffuse bluish discoloration in the gastric fundus/greater curvature with overlying crated lesions (Figure 1). Gastric body lesion measured 15 mm in diameter and actively oozing blood. Hemostasis was achieved using epinephrine injection, hemospray, and argon plasma coagulation. Histopathology of gastric specimens confirmed the presence of the amyloid deposits (Figure 2).
Endoscopic images showing a crated gastric lesion (yellow arrows) with bluish discoloration and stigmata of recent bleeding (A and B). Hemostasis was achieved using epinephrine sclerotherapy, hemospray, and argon plasma coagulation (C and D).
Hematoxylin & eosin staining demonstrating deposition of amyloid fibrous connective tissues in the interstitium with inflammatory cell infiltration (A). Congo red staining showing positivity for amyloid protein (D).
Follow-up tests, including renal ultrasound, echocardiogram, radiography, and urine studies, were unremarkable. The patient was discharged on pantoprazole, with outpatient follow-up for repeat esophagogastroduodenoscopy and possible endoscopic ultrasound. Localized gastric amyloidosis is a rare condition characterized by the deposition of amyloid proteins in the stomach, without systemic involvement.^1,2^ It is an exceptionally rare cause of upper gastrointestinal bleeding, with few cases documented in the medical literature.^2^
DISCLOSURES
Author contributions: N. Mekheal conceptualized the idea of this image article. L. Bathobakae and A. Farokhian assisted with data curation and writing of the manuscript. Y. Cavanagh edited, fact-checked, and proofread the final version of this case report. L. Bathobakae is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin XY Pan D Sang LX Chang B. Primary localized gastric amyloidosis: A scoping review of the literature from clinical presentations to prognosis. World J Gastroenterol. 2021;27(12):1132–48.33828390 10.3748/wjg.v 27.i 12.1132 PMC 8006099 · doi ↗ · pubmed ↗
- 2Oh GM Park SJ Kim JH . Localized gastric amyloidosis successfully treated with endoscopic submucosal dissection A case report. Medicine (Baltimore). 2021;100(51):e 28422.34941190 10.1097/MD.0000000000028422 PMC 8702132 · doi ↗ · pubmed ↗