Roux stasis syndrome with a diverticulum: lumen-apposing metal stent placement to straighten the lumen and restore the flow
Sid Ahmed Alioua, Jérôme Rivory, Florian Rostain, Pierre Chenet, Alexandru Lupu, Thierry Malaval, Mathieu Pioche

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
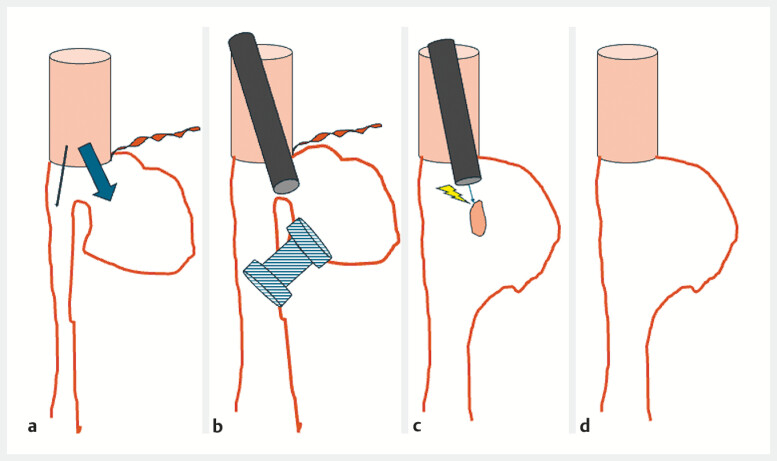 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDysphagia Assessment and Management · Esophageal and GI Pathology · Tracheal and airway disorders
Roux-en-Y esophagojejunostomy is commonly performed after total gastrectomy, especially in oncological and bariatric surgery. However, it is often associated with complications 1 2 , one of which is Roux stasis syndrome, characterized by symptoms of nausea, vomiting, and postprandial bloating due to impaired digestive flow at the anastomotic site or within the Roux limb 3 . These symptoms can have a significant impact on a patientʼs quality of life and require innovative approaches when conventional treatments fail.
This case presents a patient who developed chronic Roux stasis syndrome three years after undergoing a Roux-en-Y esophagojejunostomy. An excessively long blind jejunal limb had created a diverticulum ( Fig. 1 a ), which exacerbated her symptoms due to stasis and misdirected food flow into the diverticulum rather than the lumen. Conservative therapies did not provide adequate relief, so endoscopic intervention was considered.
Schematic description of the procedure. a Initial aspect with a blind jejuna loop and the main lumen. b Placement of a lumen-apposing metal stent between the terminal part of the jejunum and the main lumen. c Mucosal bridge section remaining after removal of the stent. d Final aspect after section of the spur.
A lumen-apposing metal stent (LAMS) was used to address the anatomical and functional abnormalities causing Roux stasis syndrome. A 20-mm LAMS was used to improve flow by creating communication between the two segments ( Fig. 1 b , Video 1 ), resulting in immediate symptomatic relief. The stent will be removed in three months with simultaneous resection of the residual mucosal spur ( Fig. 1 c ).
Roux stasis syndrome with a diverticulum: lumen-apposing metal stent placement to straighten the lumen and restore the flow.Video 1
LAMS provides an effective, minimally invasive approach to the treatment of Roux stasis syndrome, offering an alternative to surgery in selected cases. Future studies are needed to validate its long-term efficacy and role in broader management strategies for this syndrome.
Endoscopy_UCTN_Code_TTT_1AS_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wei M Wang N Yin Z Short-term and quality of life outcomes of patients using linear or circular stapling in esophagojejunostomy after laparoscopic total gastrectomy J Gastrointest Surg 2021251667167610.1007/s 11605-020-04806-032989689 · doi ↗ · pubmed ↗
- 2Lu J Wu Z Liu G The clinical effectiveness of establishing a proximal jejunum pouch after laparoscopic total gastrectomy: A propensity score-based analysis Asian J Surg 20224542543010.1016/j.asjsur.2021.07.00234315672 · doi ↗ · pubmed ↗
- 3Gustavsson S Ilstrup DM Morrison P Roux-Y stasis syndrome after gastrectomy Am J Surg 198815549049410.1016/s 0002-9610(88)80120-x 3344916 · doi ↗ · pubmed ↗