Case Report: Intraoperative Fascial Traction for Increasing Intra-Abdominal Volume in Loss-of-Domain Incisional Hernias: A Report of Two Cases
Hakan Gök

TL;DR
This case report describes using intraoperative fascial traction to safely repair complex hernias with reduced abdominal space, offering a promising new surgical technique.
Contribution
The paper introduces intraoperative fascial traction as a novel technique for managing incisional hernias with loss of domain.
Findings
Intraoperative fascial traction successfully increased intra-abdominal volume in two patients with loss of domain.
The technique facilitated primary fascial closure without serious complications in both cases.
IFT shows potential to reduce risks of intra-abdominal hypertension and compartment syndrome.
Abstract
The primary goal in incisional hernia repair is achieving primary fascial closure and reinforcing the area with a synthetic mesh. However, when Loss of Domain (LoD) is present, serious complications such as intra-abdominal hypertension (IAH) and abdominal compartment syndrome (ACS) may arise. Various strategies have been employed to overcome these challenges and increase the reduced intra-abdominal volume, including preoperative botulinum toxin (BTA) injection, progressive pneumoperitoneum (PPP), various component separation techniques, and their combinations. Intraoperative fascial traction (IFT) has recently been added to this armamentarium. The two cases presented here aim to demonstrate the potential benefits of this innovative technique and offer a different perspective to surgeons dealing with such challenging cases. The two patients presented here had previously undergone open…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
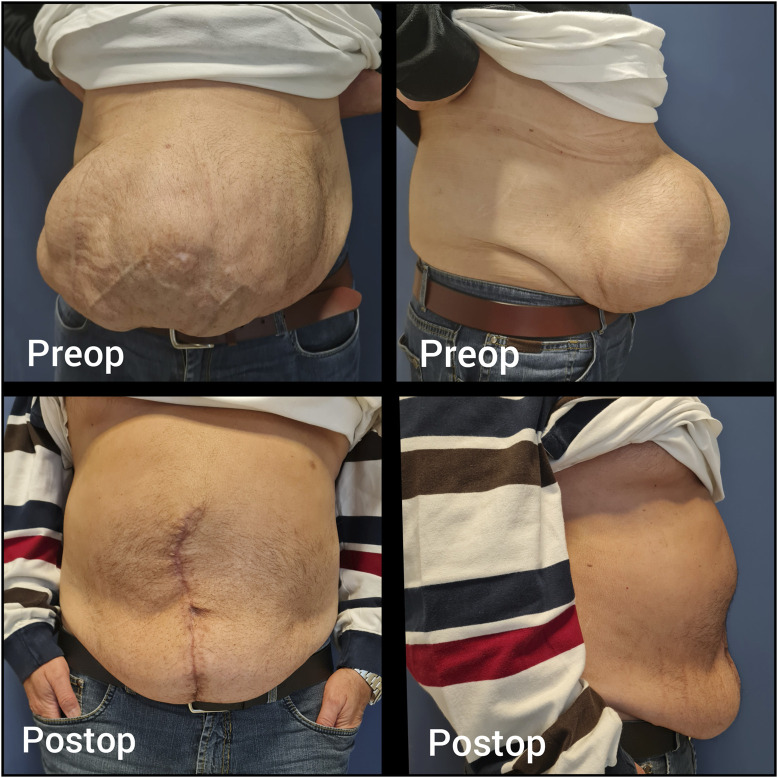 FIGURE 1
FIGURE 1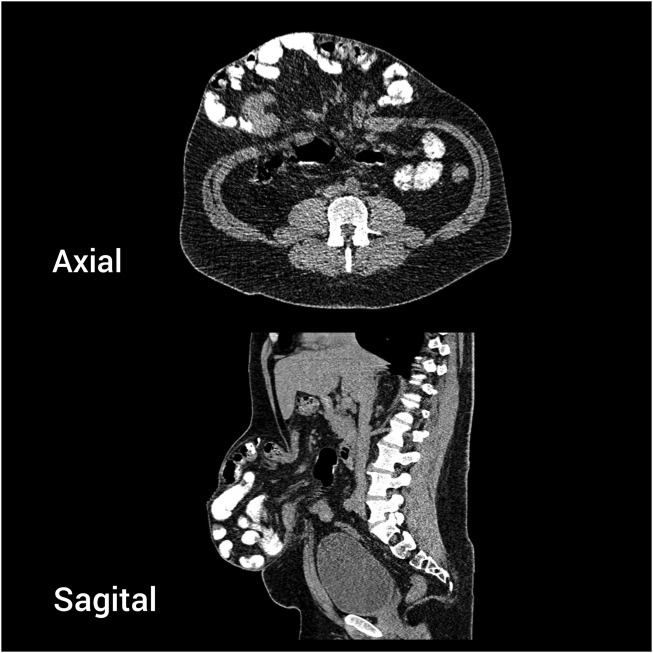 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3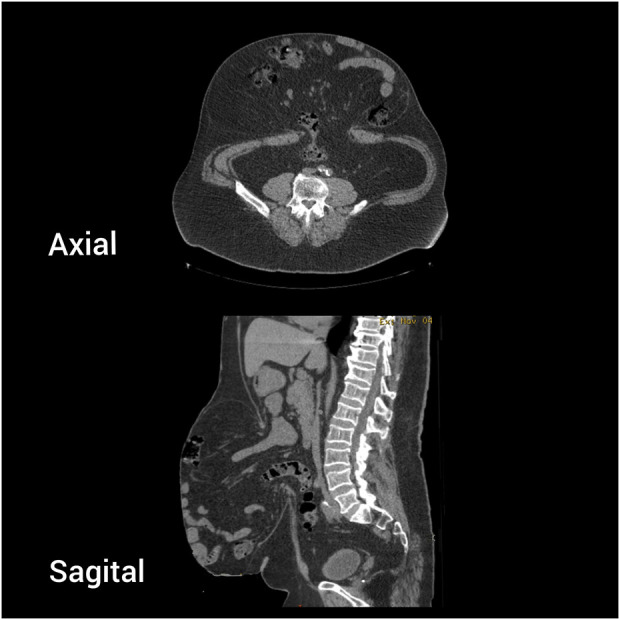 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Intestinal and Peritoneal Adhesions · Pelvic and Acetabular Injuries
Introduction
The treatment of incisional hernias with an associated loss of domain (LoD) presents significant challenges. These patients often suffer from comorbidities such as diabetes, obesity, chronic obstructive pulmonary disease (COPD), and cardiac conditions, which individually or in combination can complicate hernia repair [1–5]. Preoperative optimisation, including weight reduction, diabetes control, smoking cessation, and respiratory physiotherapy, is crucial in improving outcomes [5–7].
The primary goal in hernia repair is to achieve a durable and recurrence-free outcome. In incisional hernias, this goal is best accomplished by ensuring the closure of the anterior fascia, followed by reinforcement with a mesh, which minimises complications and recurrence [8–10]. However, in cases where LoD is present, the situation becomes more complex [11].
LoD refers to a condition where a significant portion of intra-abdominal organs resides outside the abdominal cavity within the hernia sac, leading to a reduced intra-abdominal volume. Preoperative imaging with a CT scan and volumetric analysis are essential to assess the presence and extent of LoD [12, 13]. In these patients, the challenge lies in reintegrating the displaced organs into the original abdominal cavity without causing intra-abdominal hypertension (IAH), which can impair organ perfusion and pulmonary function or, in severe cases, lead to abdominal compartment syndrome (ACS) [14–18].
To address these challenges, various techniques have been developed to increase intra-abdominal volume. Preoperative interventions such as botulinum toxin A (BTA) injection, progressive pneumoperitoneum (PPP), and anterior or posterior component separation can be employed individually or in combination based on patient-specific needs [19–28].
In recent years, intraoperative fascial traction (IFT) has emerged as a promising technique for managing patients with large defects and LoD. This approach not only facilitates primary fascial closure but also contributes to increasing intra-abdominal volume, thereby mitigating the risks of postoperative complications [29–31].
In this report, we present two case studies of patients with incisional hernias and LoD, where IFT was successfully employed to enhance intra-abdominal volume and achieve primary fascial closure.
Case Reports
Case 1
A 49-year-old male patient underwent open umbilical hernia repair with mesh 17 years ago. The hernia recurred shortly after surgery and progressively enlarged over time. The patient had a BMI of 30, type 2 diabetes, and a history of smoking one pack of cigarettes per day. Physical examination revealed a large, irreducible recurrent umbilical hernia (Figure 1). CT imaging showed a 6 × 7 cm hernia defect and a large sac containing small bowel loops under the skin, resembling an hourglass appearance (Figure 2). The Tanaka Index was calculated at 30%.
Case 1 - Preoperative and postoperative clinical appearance.
Case 1 - Preoperative CT scan. Axial and sagittal view.
One month prior to surgery, 200 U of botulinum toxin A (Botox^®^, Allergan Inc., United States) was injected bilaterally under ultrasound guidance into the external oblique (EO), internal oblique (IO), and transversus abdominis (TA) muscles. The patient was advised to quit smoking. However, a urinary nicotine test was not performed before surgery.
During surgery, complete adhesiolysis was performed, followed by a Rives-Stoppa dissection. A 15 × 20 cm medium-weight macroporous mesh was placed in the retrorectus space. IFT using the Fasciotens device (Fasciotens^®^ GmbH, Germany) was applied, enabling successful primary fascial closure without pathological increases in intra-abdominal pressure (IAP). This was checked on the anaesthesia machine by monitoring the peak plateau pressures. The patient developed postoperative paralytic ileus, which resolved with non-operative operative treatment. The patient was discharged without any other complications on postoperative day 5. At the 1-year follow-up, no recurrence was observed (Figure 1).
Case 2
A 64-year-old male patient underwent open umbilical hernia repair with mesh 5 years ago. Recurrence occurred 2 months after surgery, and the hernia progressively enlarged over time. The patient had a BMI of 36.7 and well-controlled hypertension on medication. Physical examination revealed a large, irreducible recurrent umbilical hernia (Figure 3). CT imaging showed a 9 × 12 cm hernia defect and a large sac containing small bowel loops under the skin (Figure 4). The Tanaka Index was calculated at 51%.
Case 2 - Preoperative and postoperative clinical appearance.
Case 2 - Preoperative CT scan. Axial and sagittal view.
One month prior to surgery, 200 U of botulinum toxin A (Botox^®^, Allergan Inc., United States) was injected bilaterally under ultrasound guidance into the EO and IO muscles.
During surgery, complete adhesiolysis was performed, followed by a Rives-Stoppa dissection. An 18 × 30 cm medium-weight macroporous mesh was placed in the retrorectus space. IFT using the Fasciotens device (Fasciotens^®^ GmbH, Germany) was applied, allowing successful primary fascial closure without pathological increases in IAP. The patient was discharged without complications on postoperative day 1. At the time of writing, the patient was in the first postoperative week, with no complications or recurrence observed (Figure 3).
Discussion
Incisional hernias represent one of the most challenging aspects of abdominal wall hernias. They are not static; they grow over time and significantly impair quality of life [1, 2]. Their repair is complex, with recurrence rates reported as high as 5%–63% [1, 3, 10].
The primary method for reducing recurrence and complications in incisional hernia repair is achieving primary fascial closure [6, 8–10]. Additionally, reinforcement of the repair with a mesh placed in the retromuscular plane significantly reduces recurrence rates. However, in large hernias with LoD returning herniated organs to the abdominal cavity may lead to IAH, potentially resulting in ACS [14–18]. This pathological condition can impair respiratory function, compromise organ perfusion, and may lead to fatal outcomes.
To prevent this, various options are available to increase intra-abdominal volume. These include the use of BTA, which relaxes and elongates the external oblique (EO), internal oblique (IO), and transversus abdominis (TA) muscles, thus increasing abdominal volume [19–23] Although BTA provides a limited volume increase, it significantly contributes to achieving primary fascial closure by simplifying the complexity of the repair, it may downstage the procedure, reducing the need for anterior or posterior component separation (PCS) and transversus abdominis release (TAR), and allowing the repair to be completed with the Rives-Stoppa technique alone [9, 21]. BTA application has become nearly standard for midline hernias classified as EHS W3 (wider than 10 cm) [32]. In our two cases, we utilised BTA both to assist with primary fascial closure and increase intra-abdominal volume.
Another effective method for increasing intra-abdominal volume is the use of component separation techniques (CST). Two primary techniques are widely practiced today: Ramirez’s anterior component separation (ACS) [27] and Novitsky’s PCS with TAR [8]. Both techniques are effective in achieving primary fascial closure in midline hernias. However, they are technically demanding. While ACS carries risks of surgical site occurrences (SSO) such as hematoma, seroma, infection, and skin necrosis, PCS-TAR may result in seroma, infection, or challenging-to-repair EIT Ambivium hernias [10, 33–38]. Therefore, expertise in these techniques and careful case selection are essential.
Progressive pneumoperitoneum (PPP) is another effective method to increase intra-abdominal volume [24–26, 39]. In this technique, a catheter is placed into the abdominal cavity, and ambient air is gradually insufflated over 7–10 days preoperatively to expand the abdominal cavity. While effective, PPP is associated with significant complications such as patient intolerance, respiratory insufficiency, bowel injury, and thromboembolic events [26, 39, 40]. It is also time-consuming and costly.
Recently, the use of IFT has gained popularity, with multicenter studies reporting successful outcomes, particularly in achieving primary fascial closure [29–31]. This technique involves placing 12 traction sutures on the medial edge of each rectus muscle and applying a vertical force (12–20 kg) over 30 min, progressively medializing the rectus complex while also increasing intra-abdominal volume.
In our two cases with midline incisional hernias and LoD, we successfully utilised IFT. For the first case, where the defect was only 6 cm wide, one might argue that it could have been easily closed without requiring any additional intervention to achieve the goal. However, the focus was solely on increasing volume. In the second case, both volume increase and primary fascial closure were achieved without causing IAH.
During retrorectus dissection, when the posterior rectus sheath is separated from the muscle, the rectus muscles lose their cylindrical structure, elongate, and expand the retrorectus space. Therefore, as observed in the second case, the available space for mesh placement is greater than the preoperatively measured rectus widths on the CT scan. However, for a 9 cm defect, an 18 cm wide mesh may appear to provide insufficient overlap. In cases of large defects, there is an ongoing debate among hernia surgeons regarding the necessity of posterior component separation and TAR to achieve adequate mesh overlap. While some advocate for TAR, other centers have reported excellent outcomes without it, and both approaches have been supported by published data [8, 31, 39].
IFT is an easy-to-perform and effective technique. No significant complications specific to the technique or device have been reported to date [41, 42]. It can be combined with BTA, CST, and PPP techniques.
It is essential to recognise that no single technique can be universally applied to all hernias. Tailoring is key. Each case must be evaluated individually to determine the most suitable approach, utilizing one or a combination of the aforementioned techniques to optimise patient outcomes.
Limitations
This study presents the early outcomes of two cases, with one patient having a follow-up period of 1 year and the other only 1 week. Given the limited sample size and short follow-up duration, these findings cannot be generalised. Further studies with larger cohorts and long-term follow-up are needed to draw more definitive conclusions.
Conclusion
The management of incisional hernias, particularly those with large defects and LoD, requires a comprehensive and individualised approach. Achieving primary fascial closure remains the cornerstone of repair, but addressing the dual challenges of fascial closure and restoring intra-abdominal volume necessitates the integration of innovative techniques such as BTA, CST, PPP, and IFT.
IFT, in particular, offers promising advantages by effectively increasing intra-abdominal volume and facilitating primary fascial closure with minimal complications. The two cases presented underscore the potential of this innovative technique in achieving successful outcomes. By tailoring the surgical approach to the specific needs of each patient, combining one or more of these advanced techniques, surgeons can optimise outcomes, reduce recurrence rates, and improve overall patient quality of life.
However, further research and larger studies are essential to fully establish the long-term efficacy and benefits of IFT in this challenging patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoffmann HKöckerling F Adolf D Mayer F Weyhe D Reinpold W Analysis of 4,015 Recurrent Incisional Hernia Repairs from the Herniamed Registry: Risk Factors and Outcomes. Hernia (2021) 25(1):61–75. 10.1007/s 10029-020-02263-x 32671683 · doi ↗ · pubmed ↗
- 2van Ramshorst GH Eker HH Hop WC Jeekel J Lange JF. Impact of Incisional Hernia on Health-Related Quality of Life and Body Image: A Prospective Cohort Study. Am J Surg (2012) 204(2):144–50. 10.1016/j.amjsurg.2012.01.012 22579232 · doi ↗ · pubmed ↗
- 3Bhardwaj P Huayllani MT Olson MA Janis JE. Year-Over-Year Ventral Hernia Recurrence Rates and Risk Factors. JAMA Surg (2024) 159(6):651–8. 10.1001/jamasurg.2024.0233 38536183 PMC 10974689 · doi ↗ · pubmed ↗
- 4Sara CG Podda M Ribas S Montori G Botteri E Agresta F What Defines an Incisional Hernia as ‘complex’: Results from a Delphi Consensus Endorsed by the European Hernia Society (EHS). Br J Surg (2024) 111(1):znad 346. 10.1093/bjs/znad 346 37897716 · doi ↗ · pubmed ↗
- 5Sanders DL Pawlak MM Simons MP Aufenacker T Balla A Berger C Midline Incisional Hernia Guidelines: The European Hernia Society. Br J Surg (2023) 110(12):1732–68. 10.1093/bjs/znad 284 37727928 PMC 10638550 · doi ↗ · pubmed ↗
- 6Ayuso SA Elhage SA Salvino MJ Sacco JM Heniford BT. State-of-the-art Abdominal Wall Reconstruction and Closure. Langenbecks Arch Surg (2023) 408(1):60. 10.1007/s 00423-023-02811-w 36690847 · doi ↗ · pubmed ↗
- 7Ayuso SA Elhage SA Fischer JP Heniford BT. The Role of Prehabilitation in Abdominal Wall Reconstruction: It Is More Than “Watch and Wait”. Ann Surg (2024) 5(2):e 449. 10.1097/AS 9.0000000000000449 PMC 1119188238911618 · doi ↗ · pubmed ↗
- 8Novitsky YW Elliott HL Orenstein SB Rosen MJ. Transversus Abdominis Muscle Release: A Novel Approach to Posterior Component Separation during Complex Abdominal Wall Reconstruction. Am J Surg (2012) 204(5):709–16. 10.1016/j.amjsurg.2012.02.008 22607741 · doi ↗ · pubmed ↗