Esophageal Achalasia in Parkinson's Disease: Diagnosis and Management of a Rare Case
Alexandros Ioannou, Francesco Torresan

TL;DR
A Parkinson's disease patient was diagnosed with esophageal achalasia and successfully treated with pneumatic dilatation.
Contribution
This paper presents a rare case linking Parkinson's disease with esophageal achalasia and highlights successful treatment.
Findings
Esophageal achalasia was diagnosed in a Parkinson's disease patient using high-resolution esophageal manometry.
Pneumatic dilatation was effective in treating the patient's esophageal achalasia symptoms.
Autonomic dysfunction in Parkinson's disease may involve degenerative loss of inhibitory neurons in the myenteric plexus.
Abstract
Autonomic dysfunction in Parkinson's disease involving the gastrointestinal track due to the presence of inclusions of a-synuclein in the vagus nerve and in the Meissner and Auerbach plexus of the enteric nervus system. Esophageal achalasia characterized by a degenerative loss of the inhibitory neurons in the myenteric plexus that causes a failure of the lower esophageal sphincter to relax leading to dysphagia, regurgitation, retrosternal pain and weight loss. We report a case of a Parkinson disease patient presented to our department due to upper gastrointestinal symptoms, diagnosed with esophageal achalasia by high resolution esophageal manometry and successfully treated with pneumatic dilatation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
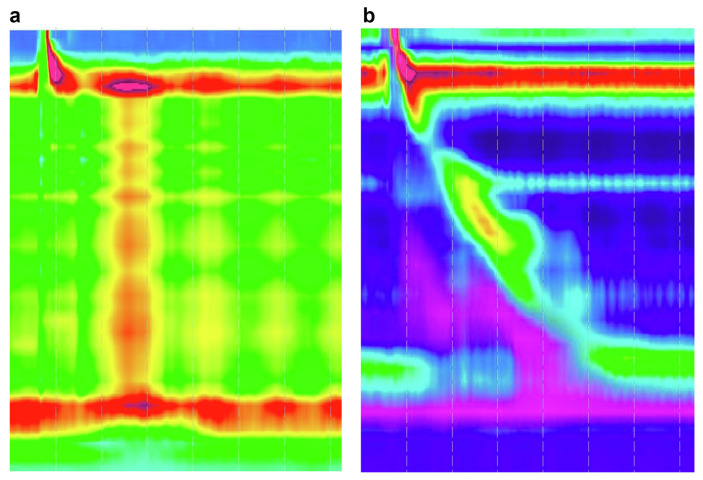 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Esophagitis · Dysphagia Assessment and Management · Esophageal and GI Pathology
Introduction
Parkinson's disease (PD) is the most common neurodegenerative condition affecting almost 1% of the aged population [1]. The two pathological hallmarks of PD are a progressive degeneration of the dopamine-containing neurons in the substantia nigra pars compacta combined with intraneuronal aggregates of eosinophilic inclusions, mainly phosphorylated a-synuclein [2,3]. Although PD is regarded as a movement disorder, non-motor manifestations, such as autonomic dysfunctions, particularly those involving the gastrointestinal (GI) tract (dysphagia and constipation), are increasingly recognized [4]. In particular, the enteric nervous system (ENS) is a prime target of the pathological process of PD. Indeed, autopsies of parkinsonian patients reveal the widespread presence of a-synuclein aggregates in myenteric and submucosal neurons throughout the GI tract [5].
Achalasia is an esophageal motility disorder with a prevalence of ~1: 10 000. Dysphagia consists of the main clinical manifestation followed by regurgitation, retrosternal pain and weight loss. A degenerative loss of the inhibitory neurons of the myenteric plexus causing absence of esophageal peristalsis and failure of relaxation of the lower esophageal sphincter represent main pathogenetic basis [6,7]. However, some studies highlighted that the location of denervation could be preganglionic and that postganglionic nerves could be intacted, suggesting a central origin for primary achalasia [8]. Epidemiologic studies suggest that achalasia appears to represent the clinical endpoint of several pathways. Not only aging but also different neurologic diseases may contribute to a loss in control of esophageal motility [9].
We report the case of a 63-year-old woman affected by Parkinson's disease that was referred to our department due to dysphagia, regurgitation, retrosternal pain, and weight loss of 15 kg in the last 2 months and diagnosticated with esophageal achalasia.
Case report
A 63-year-old female patient, diagnosed with PD four years ago, presenting mild rigidity and resting tremor successfully treated with levodopa/benserazide. The patient was also affected by non-motor PD symptoms, namely depression and mild constipation.
She was referred to our clinic, presented dysphagia in every meal for the last two months, daily regurgitation, daily retrosternal pain and weight loss of 15 kg. (Eckardt score:10). The patient performed: (i) an upper GI endoscopy without any particular finding; (ii) a Video Fluoroscopic Swallowing Exam with a minor difficulty of forming and swallowing the bolus; and (iii) a Rx esophagogram with appearance of barium height of >5 cm at 1 min. Moreover, an examination with a high-resolution esophageal manometry (Fig. 1(a)) that highlighted an esophageal achalasia type II manometric pattern according to Chicago Classification Criteria v4.0 (Integrated Relaxation Pressure (IRP) 34.1 mmHg, 80% panesophageal pressurization). The patient was initially treated with a 30 mm rigiflex balloon dilatation with minor benefit on regurgitation and chest pain, while dysphagia persisted in every meal (Eckardt score: 6). Therefore, a second dilatation with a 35 mm rigiflex balloon was performed. At the follow up visit, after a month of the second dilatation, the patient was in clinical remission without regurgitation, rare episodes of retrostrnal pain, occasional dysphagia and stable weight (Eckardt score: 2) Finally, a second high-resolution manometry was performed (Fig. 1(b)) that revealed improvement of the manometric parameters (IRP 14.3 mmHg).
Discussion
Dysphagia is a common symptom in PD patients that deteriorate their quality of life. Its etiology is multifactorial and its management challenging [10]. Dysphagia has been usually attributed to oropharyngeal dysfunction detected fluoroscopically and rarely to disordered esophageal motility [11]. Several studies using water-perfused manometry have identified esophageal motility abnormalities in parkinsonian patients [12,13]. Recently, Su et al. evaluated 33 patients, that were affected by PD and experienced dysphagia, by performing high resolution esophageal manometry. According to the Chicago classification criteria a variety of esophageal abnormalities were identified but no patient presented esophageal achalasia [14]. Suttrup et al. studied using high resolution manometry 65 PD patients with dysphagia in different stages of their disease highlighting that esophageal body impairment is frequent in all stages of the disease and possibly reflects a-synucleinopathy in the enteric nervus system [15]. On the other hand, several studies suggest a central origin for primary achalasia involving the dorsal motor nuclei of the vagus and the ambiguous nuclei, the anatomical structures controlling esophageal motility. The causes of these neural lesions remain unknown. Neurotropic virus, such as herpes zoster, selectively attacking neurons of the vagal nucleus were involved [7].
Multiple recent studies suggest an early occurrence of the upper gastrointestinal dysfunction in PD patients [10,16]. Qualman et al. identified Lewy Bodies in degenerating ganglion cells of the esophageal myenteric plexus in achalasia patients [17]. Additionally, Wakabayashi et al. revealed esophageal Lewy Bodies in PD patients with dysphagia, while weren't present in PD patients without dysphagia and controls [5]. These findings suggest that a subset of achalasia and PD patients with dysphagia may have similar mechanisms of neuronal degeneration responsible for the esophageal dysfunction.
Some case reports in the literature suggest a link between PD and achalasia [18,19]. An epidemiological study by Becker et al. revealed that PD was more frequent in parents of achalasia patients than in control subject parents. Case-control studies stratifying for age provides useful data regarding the relation between PD and achalasia given that PD represents an age-related disorder. Notably, Sonnenberg et al. [9] revealed that in elderly achalasia patients, PD was one of the comorbid disorders observed [20]. Currently there are data neither about the high resolution manometric presentation at the diagnosis nor about the results of the treatment with pneumatic dilatation on the manometric tracing of patients with PD and esophageal achalasia.
In our case, a 63-year-old female patient that was diagnosed with PD, four years before, was referred to our department due to upper gastrointestinal symptoms. Performing a high-resolution manometry, the gold standard exam for esophageal motility disorders, highlighted the presence of esophageal achalasia type II according to the Chicago classification criteria v4.0. The patient was treated successfully with pneumatic dilatation.
Learning pointsParkinson's disease (PD) frequently involves gastrointestinal (GI) tract (dysphagia, gastroparesis, and constipation) deteriorating patients' quality of life.Dysphagia in PD is a clinically relevant symptom, usually caused due to Upper Esophageal Sphincter disfunction affecting the oral and pharyngeal phase of swallowing. Esophageal achalasia represents a very rare cause of dysphagia in PD.High resolution esophageal manometry is the gold standard for the study of esophageal impairment in PD and may therefore define an effective therapeutic treatment in patients with specific esophageal motor disfunction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Rijk MC Tzourio C Breteler MM Prevalence of parkinsonism and Parkinson's disease in Europe: the EURO-PARKINSON collaborative study. European Community Concerted Action on the Epidemiology of Parkinson's disease J Neurol Neurosurg Psychiatry 1997 62 10 5 9010393 10.1136/jnnp.62.1.10PMC 486688 · doi ↗ · pubmed ↗
- 2Schulz-Schaeffer WJ The synaptic pathology of alpha-synuclein aggregation in dementia with Lewy bodies, Parkinson's disease and Parkinson's disease dementia Acta Neuropathol 2010 120 131 43 20563819 10.1007/s 00401-010-0711-0PMC 2892607 · doi ↗ · pubmed ↗
- 3Giancola F Torresan F Repossi R Bianco F Latorre R Ioannou A Downregulation of neuronal vasoactive intestinal polypeptide in Parkinson's disease and chronic constipation Neuro Gastroenterol Motil 2017 May 29 5 10.1111/nmo.12995 PMC 539395127891695 · doi ↗ · pubmed ↗
- 4Poewe W Non-motor symptoms in Parkinson's disease Eur J Neurol 2008 15 Suppl 1 14 20 18353132 10.1111/j.1468-1331.2008.02056.x · doi ↗ · pubmed ↗
- 5Wakabayashi K Takahashi H Takeda S Ohama E Ikuta F Parkinson's disease: the presence of Lewy bodies in Auerbach's and Meissner's plexuses Acta Neuropathol 1988 76 217 21 2850698 10.1007/BF 00687767 · doi ↗ · pubmed ↗
- 6Boeckxstaens GE Zaninotto G Richter JE Achalasia Lancet 2014 383 83 93 23871090 10.1016/S 0140-6736(13)60651-0 · doi ↗ · pubmed ↗
- 7Park W Vaezi MF Etiology and pathogenesis of achalasia: the current understanding Am J Gastroenterol 2005 100 1404 14 15929777 10.1111/j.1572-0241.2005.41775.x · doi ↗ · pubmed ↗
- 8Cohen S Fisher R Tuch A The site of denervation in achalasia Gut 13 556 558 5069732 10.1136/gut.13.7.556PMC 1412277 · doi ↗ · pubmed ↗