Fenestration and Bifurcation of the Internal Jugular Vein; Surprises During Head and Neck Surgery
Vibha Singh, Arijit Jotdar, Annanya Soni, Rudra Prakash, Kushal Singh

TL;DR
This paper reports three rare anatomical variations of the internal jugular vein encountered during head and neck surgeries, emphasizing the importance of pre-operative imaging to avoid surgical complications.
Contribution
The paper contributes three clinical case reports of IJV bifurcation and fenestration, highlighting their surgical implications.
Findings
Three cases of IJV anomalies (bifurcation and fenestration) were identified during head and neck surgeries.
Pre-operative imaging and anatomical knowledge are critical to prevent intra-operative complications.
The spinal accessory nerve and omohyoid muscle were found in variable positions relative to the IJV anomalies.
Abstract
The internal jugular vein (IJV) is one of the major vessels in the neck and serves as an important landmark for surgeons during head and neck surgery. Anomalies of the IJV are rare and seldom encountered by the surgeons. However, a comprehensive knowledge of these variations is essential for better surgical dissection and to prevent intra-operative mishaps. The variations can be in the forms of bifurcation, trifurcation, duplication, fenestration and posterior tributaries of the IJV. Here we describe three cases of bifurcation and fenestration of the IJV that we encountered in our surgical practice. In the first patient, we found an empty fenestration of the right internal jugular vein during a selective neck dissection for tongue carcinoma. The spinal accessory nerve was passing lateral to the IJV above the level of the fenestration. The second patient was operated for a left vagal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
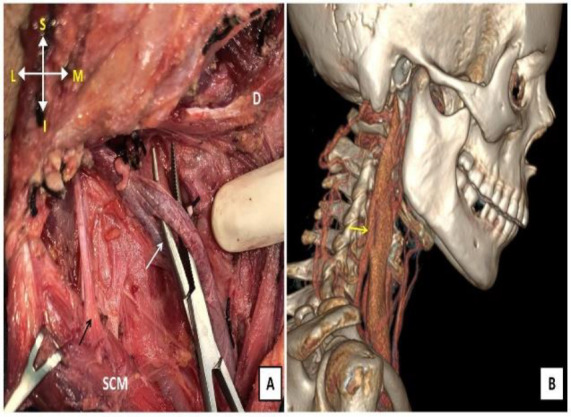 Fig 1
Fig 1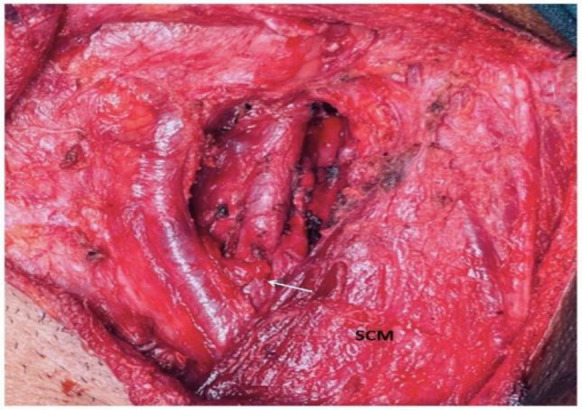 Fig 2
Fig 2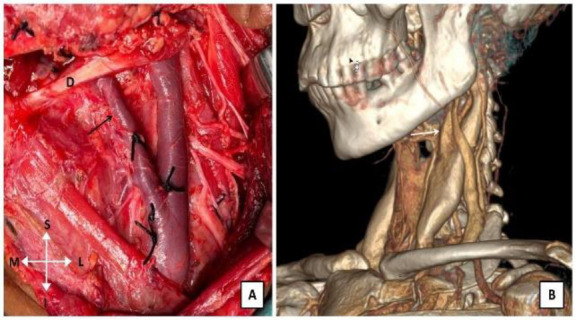 Fig 3
Fig 3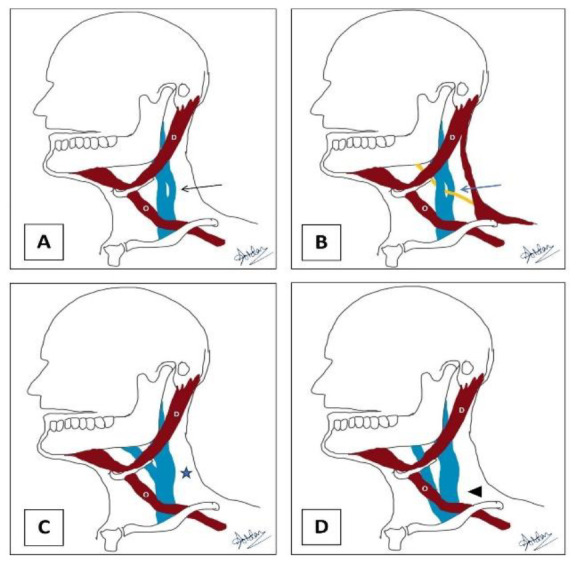 Fig 4
Fig 4| Sl No | Author | Study population | Reported cases of anatomical variations | Types of anatomical variations | Prevalence |
|---|---|---|---|---|---|
|
| Prades et al (4) | 750 | 3 | Duplication | 0.4% |
|
| Wang X et al (9) | 221 | 2 | Fenestration & duplication | 0.9% |
|
| Hashimoto et al (10) | 123 | 4 | Fenestration | 3.3% |
|
| Contrera et al (11) | 295 | 3 | Fenestration, duplication and bifurcation | 1% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAirway Management and Intubation Techniques · Venous Thromboembolism Diagnosis and Management
Introduction
The internal jugular vein (IJV) is one of the most significant vascular landmarks for surgeons during head and neck surgery. As a continuation of the sigmoid sinus, this major vessel enters the neck through the jugular foramen and drains into the Subclavian vein to form the Brachiocephalic vein (1). It is an important landmark for the Spinal accessory nerve (SAN), Vagus nerve, Carotid artery and cervical lymph nodes (2).
This large calibre vessel also serves as the route for central venous access and is hence important for anaesthetists and intensivists. Anatomical variations of the IJV are uncommon and are mostly reported by anaesthetists during imaging for central venous access (1). The Internal jugular vein receives both major and minor tributaries in the neck. Any major surgery in the neck involves the handling of this vessel. Therefore, an in-depth knowledge of its normal anatomy and associated variations is essential to avoid any untoward incident during surgical dissection. Any such anatomical variation of the IJV and adjacent vital structures especially the spinal accessory nerve can be diagnosed preoperatively by meticulous examination of the imaging studies including CT scans and MRI scans, which are routinely performed for any head and neck surgery. However, due to its rarity, the variations of the IJV are sometimes overlooked and remain undetected preoperatively.
Case Report
Case 1:
A 48-year-old lady presented in the department of Otorhinolaryngology with a non-healing ulcer over the right lateral border of the tongue. Biopsy from the lesion yielded a well-differentiated squamous cell carcinoma. The patient was staged as cT_2_N_1_M_0_ after all necessary investigations. She underwent Wide local excision with selective neck dissection (I-IV) with primary repair.
During neck dissection, we found that the right internal jugular vein split into two branches just below the level of the hyoid bone. Both the branches fused again to form a single trunk of the IJV at the level of the cricoid cartilage. No significant neurovascular structure was found passing between the branches making it an empty fenestration (Figure 1). The spinal accessory nerve was found separately above the level of fenestration. Fibrofatty tissue was gently dissected from both the branches and neck dissection was completed. The intraoperative period was uneventful with no injury to the internal jugular vein and spinal accessory nerve. Postoperatively virtual CT scan was reviewed which confirmed an empty fenestration of the right internal jugular vein.
Case 2:
A 19-year-old gentleman presented with a gradually progressive swelling over the left side of the neck for the last one year. Fine needle aspiration cytology pointed towards a spindle cell neoplasm. MRI scan was suggestive of a vagal schwannoma.
The patient was taken up for trans-cervical excision of vagal schwannoma under general anaesthesia. Intraoperatively, the left common carotid artery and the left internal jugular vein were found to be pushed medially by the tumour.
Another major vessel was found to be running vertically over the tumour, which could be traced back up to the skull base. On incising the carotid sheath, we found a bifurcation of the left internal jugular vein just above the level of the cricoid cartilage (Figure 2). The tumour was carefully separated from the internal jugular vein, thereby preserving both of its branches.
Case 3:
A 60-year-old lady presented with a gradually progressive swelling of the left parotid region for the last one year. A fine needle aspiration cytology from the swelling was suggestive of carcinoma ex pleomorphic adenoma of the left parotid gland. The patient was staged cT_3_N_0_M_0_ after all necessary investigations. She underwent left total conservative parotidectomy with left-sided modified radical neck dissection (level I–V). During the dissection of cervical lymph nodes, two branches of the left internal jugular vein were found arising deep into the digastric muscle. Both the branches continued separately up to the level of the cricoid cartilage and then fused above the omohyoid muscle confirming a bifurcation of the left internal jugular vein (Figure 3). This was further established by a careful examination of the virtual CT scan.
Discussion
Anomalies of the internal jugular vein are rare and often remain undetected pre-operatively during head and neck surgery. This may be in the forms of bifurcation, duplication, fenestration, trifurcation and posterior tributary of the internal jugular vein (1).
Mumtaz S et al in a literature review of 27 articles consisting of 1197 cases, reported only 40 cases of anatomical variations of the internal jugular vein. Among these cases, bifurcation was found only in four cases, and fenestration in sixteen cases. Although rare, the prevalence of the IJV anomalies is variable in different studies (Table 1).
Some ambiguity exists among the head and neck surgeons regarding the terms ‘bifurcation’ and ‘duplication’ of the IJV. Some authors suggest the term ‘bifurcation’ when the IJV splits above the level of the omohyoid muscle (1). In our case series, the second and third cases had a bifurcation of the internal jugular vein as both branches fused above the level of the omohyoid muscle (Figure 4). The relation of the spinal accessory nerve (SAN) with the internal jugular vein needs special mention in this context. In most of the cases, the spinal accessory nerve passes lateral to the IJV (56 – 90%) followed by medial to the IJV (10 – 44%) (3,4). However, in extremely rare cases, the SAN may pass through a fenestration in the IJV with only a few reported cases in the literature (5-7). Empty fenestration of the internal jugular vein is even rarer. In such cases, no neurovascular bundle or important structure passes through the fenestration of the IJV (Figure 4). Sometimes the ipsilateral internal carotid artery may coil through a fenestration in the IJV (8). In our case series, the first patient had an empty fenestration in the IJV with the spinal accessory nerve passing lateral to it.
The internal jugular vein is one of the largest vessels encountered during head and neck surgeries. Anomalies of the IJV are usually incidental findings during neck explorations. Non-meticulous dissection intraoperatively in such cases can lead to injury to the IJV as well as to the spinal accessory nerve. This can result in significant post-operative morbidity to the patient. It can also cause a blood-filled operative field thereby increasing the intraoperative time.
These anomalies can be identified pre-operatively on careful examination of the imaging. The surgeon should be aware and vigilant about these anatomical variations of the IJV that can improve the surgical dissection and the overall postoperative outcome. It can also be helpful in radical neck dissection where the IJV needs to be sacrificed. In this article, we reported three cases of rare anatomical variations of the internal jugular vein.
Conclusion
Anatomical variations of the internal jugular vein are rare and often found incidentally during head and neck surgeries. A meticulous evaluation of the pre-operative imaging studies may help the surgeons to be vigilant and cautious during dissection around the internal jugular vein in such situations.
A. Empty fenestration of the right internal jugular vein (white arrow). The spinal accessory nerve is passing lateral to the IJV above the level of the fenestration (black arrow). The sternocleido- mastoid (SCM) and digastric (D) muscles are also seen in the surgical field. B. Reconstructed virtual CT scan of the patient showing the empty fenestration of the right internal jugular vein (yellow arrow).
Bifurcation of the left internal jugular vein (white arrow). Both the tributaries fused above the level of the omohyoid forming the main trunk of the internal jugular vein.
A. Bifurcation of the left internal jugular vein (black arrow). Both the branches fuse above the level of the omohyoid muscle to form the main trunk of the IJV. The digastric muscle (D) is seen in the surgical field. B. Reconstructed virtual CT scan of the patient showing bifurcation of the left internal jugular vein (white arrow).
Schematic diagram representing the anatomical variations of the internal jugular vein; A. Empty fenestration of the internal jugular vein (black arrow). B. Fenestration in the internal jugular vein transmitting the spinal accessory nerve through it (blue arrow). C. Bifurcation of the IJV above the level of the omohyoid muscle (O), marked by a blue star. D. Duplication of the IJV below the level of the omohyoid muscle, marked by a black arrowhead.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mumtaz S Singh M Surgical review of the anatomical variations of the internal jugular vein: an update for head and neck surgeons Ann R Coll Surg Engl.2019 Jan 101123032228910.1308/rcsann.2018.0185 PMC 6303832 · doi ↗ · pubmed ↗
- 2Rivard AB Kortz MW Burns B Anatomy, Head and Neck: Internal Jugular Vein Stat Pearls (Internet)2023 Treasure Island (FL)Stat Pearls Publishing 30020630 · pubmed ↗
- 3Ibrahim B Berania I Moubayed SP Christopoulos A Ayad T Internal Jugular Vein Duplication: Anatomic Relationship With the Spinal Accessory Nerve J Oral Maxillofac Surg.2016 Jul 7471502.e 110.1016/j.joms.2016.03.00227055229 · doi ↗ · pubmed ↗
- 4Prades JM Timoshenko A Dumollard JM Durand M Merzougui N Martin C High duplication of the internal jugular vein: clinical incidence in the adult and surgical consequences, a report of three clinical cases Surg Radiol Anat.2002 May 2421291219702310.1007/s 00276-002-0020-y · doi ↗ · pubmed ↗
- 5Franchi T Patterson A Rare Intraoperative Finding of the Spinal Accessory Nerve Piercing a Fenestration in the Internal Jugular Vein: A Case Report and Review of the Modern Literature J Maxillofac Oral Surg.2023 Mar 2212622643670365310.1007/s 12663-021-01613-1PMC 9871109 · doi ↗ · pubmed ↗
- 6Takaoka S Yamagata K Okubo-Sato M Fukuzawa S Uchida F Ishibashi-Kanno N Bukawa H Anatomical Variant of Spinal Accessory Nerve Passing through Fenestrated Internal Jugular Vein Case Rep Dent.2022 Mar 70879703537884210.1155/2022/7087970 PMC 8976659 · doi ↗ · pubmed ↗
- 7Guarino P Tesauro P Giordano L Caporale CD Presutti L Mattioli F Surgical and radiological perspectives for the spinal accessory nerve passing through a fenestrated internal jugular vein: case series and literature review J Surg Case Rep.2024 Apr 2024410.1093/jscr/rjae 099PMC 1101488138617811 · doi ↗ · pubmed ↗
- 8Iftikhar H Ikram M Coiling of internal carotid through 'eye of the needle' internal jugular vein: a dual great vessel anomaly Ann R Coll Surg Engl.2021 May 1035 e 1563368242910.1308/rcsann.2020.7074 PMC 10335181 · doi ↗ · pubmed ↗