A Pathologist’s Dilemma: Placental Site Tumor and Its Differential Diagnosis
Chaimae Daoudi, Anass Haloui, Nada Akouh, Karich Nassira, Amal Bennani

TL;DR
This paper discusses the challenges in diagnosing a rare placental tumor and highlights the importance of distinguishing it from similar conditions for proper treatment.
Contribution
The paper provides a detailed case study and differential diagnosis tables to aid in identifying placental site tumors.
Findings
Accurate diagnosis of PSTT requires careful pathological and clinical evaluation.
Differential diagnosis tables help distinguish PSTT from other gestational trophoblastic tumors.
The case highlights the rarity and diagnostic challenges of PSTT.
Abstract
Placental site trophoblastic tumor (PSTT) is a rare neoplasm originating from intermediate trophoblastic cells at the site of placental implantation. Its diagnosis poses significant challenges, particularly in distinguishing it from other gestational trophoblastic tumors, such as epithelioid trophoblastic tumors, choriocarcinoma, and placental site nodules, as well as the benign exaggerated placental site. We present a case of a 29-year-old woman with persistent gestational trophoblastic disease following a complete hydatidiform mole. A detailed review of the differential diagnoses is provided in tables to aid in the diagnostic process, allowing for a clearer comparison and better understanding of these conditions. This report highlights the importance of accurately identifying PSTT by eliminating potential differential diagnoses through careful pathological and clinical evaluation.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
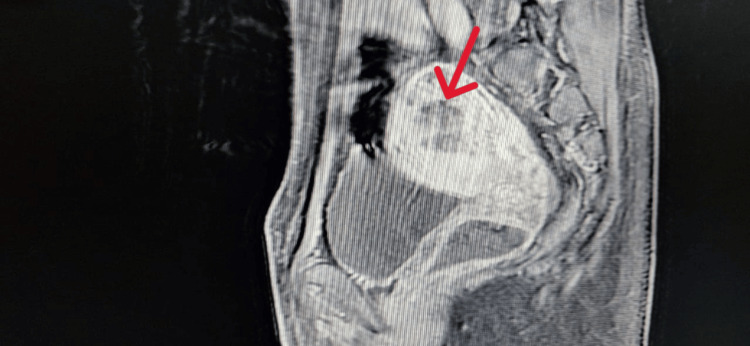 Figure 1
Figure 1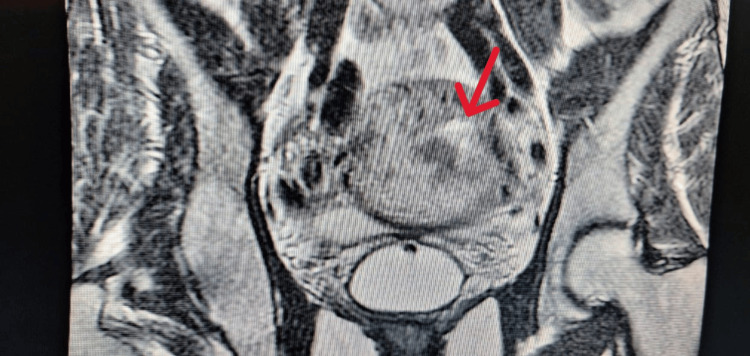 Figure 2
Figure 2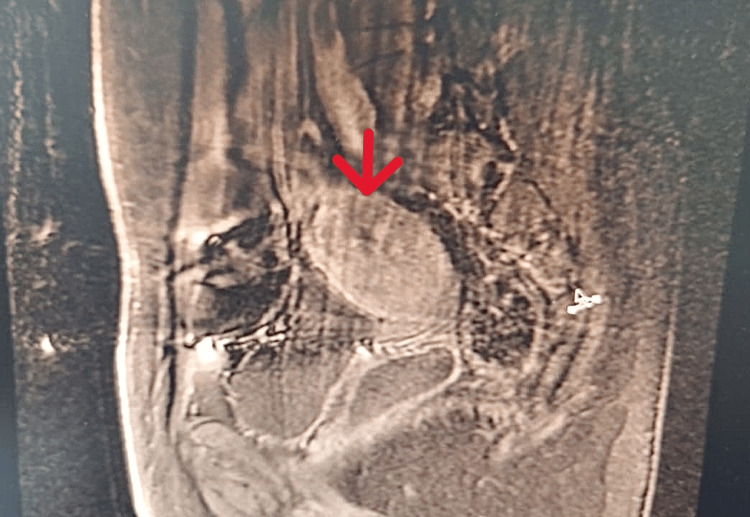 Figure 3
Figure 3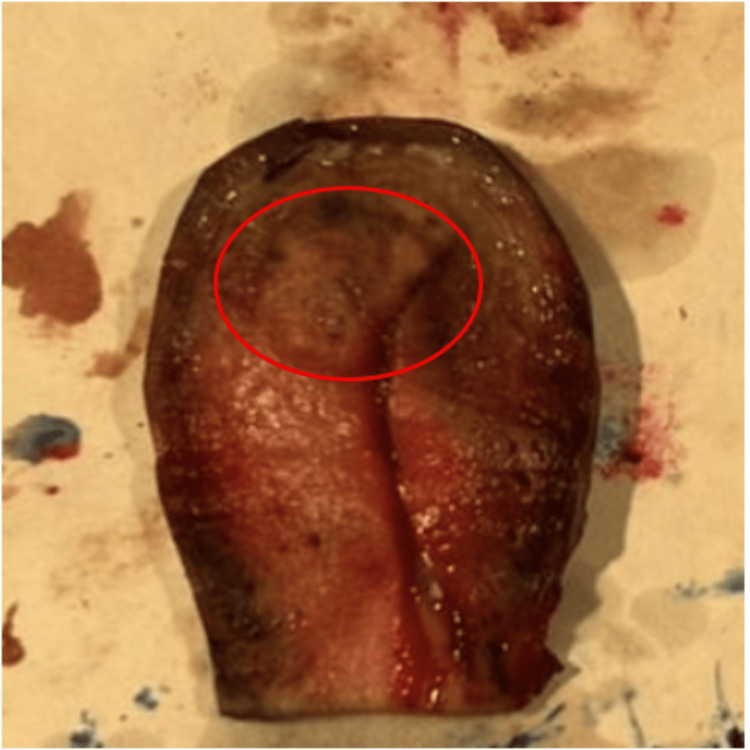 Figure 4
Figure 4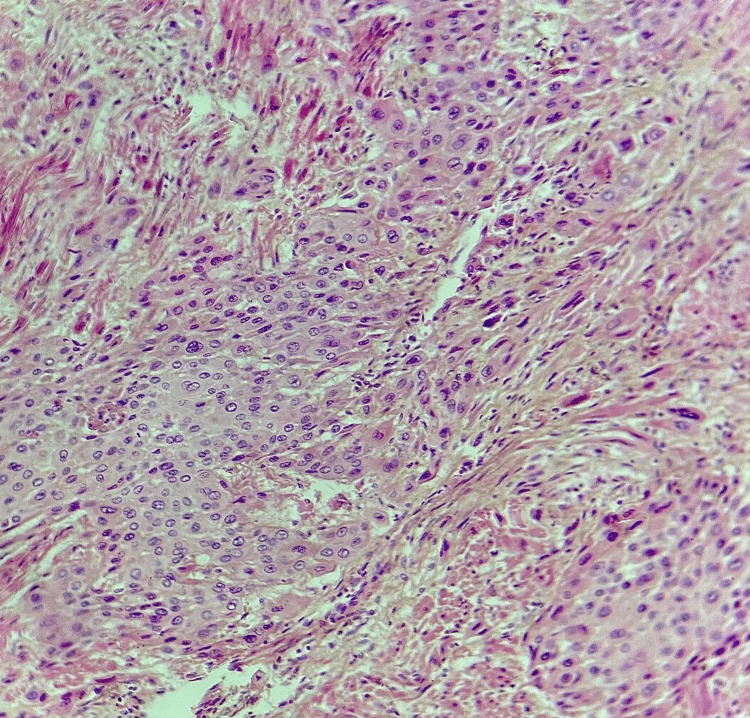 Figure 5
Figure 5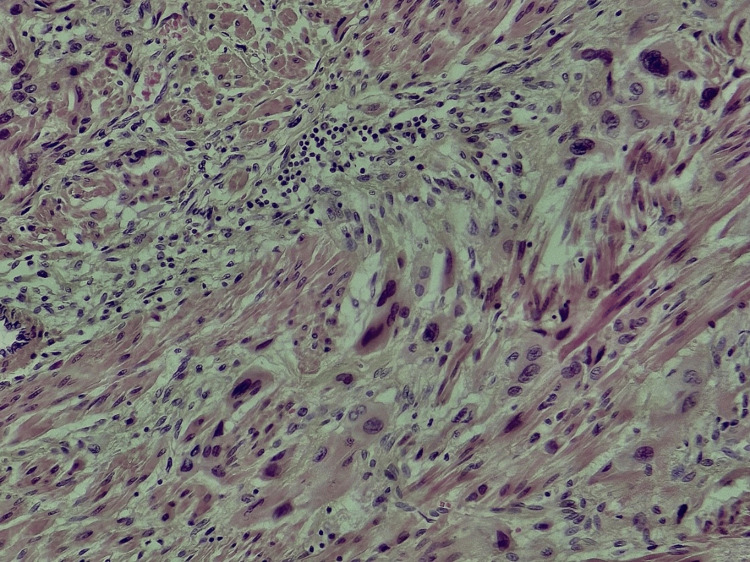 Figure 6
Figure 6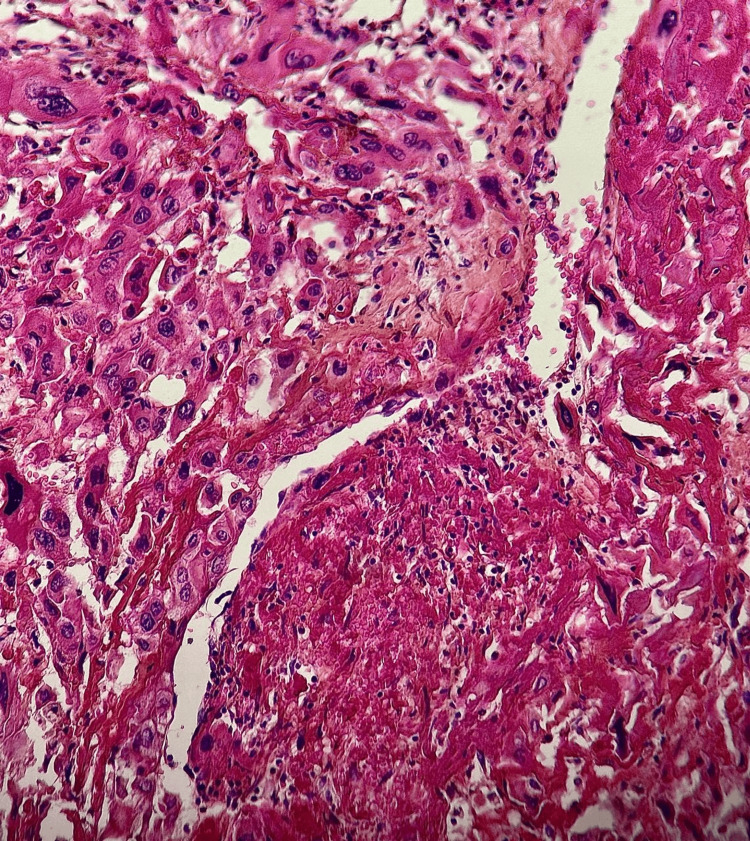 Figure 7
Figure 7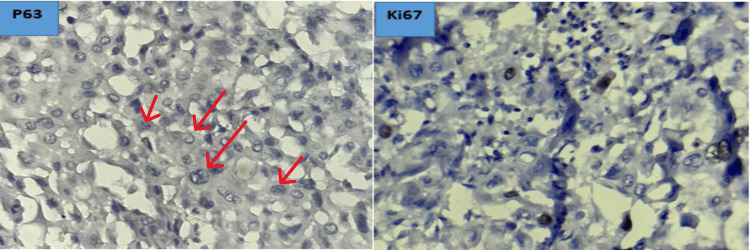 Figure 8
Figure 8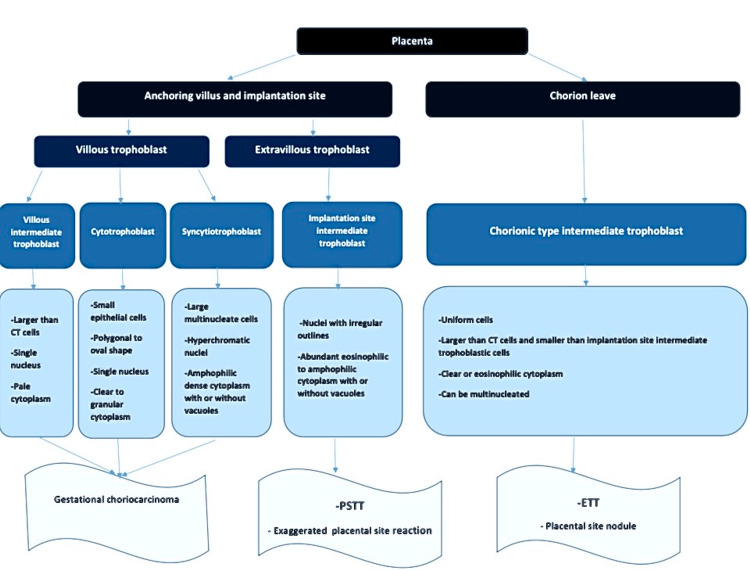 Figure 9
Figure 9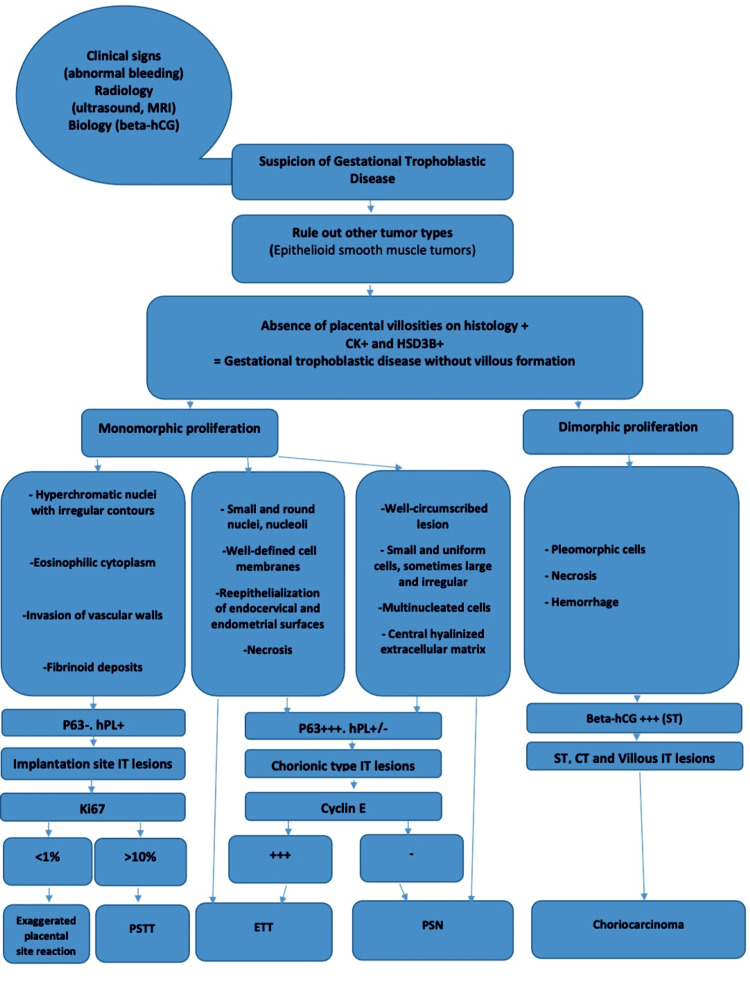 Figure 10
Figure 10| PSTT | ETT | Choriocarcinoma | Placental site nodule | Exaggerated placental site reaction | |
| Age | 20-63 years | 15-66 years | 29-31 years | Childbearing age | |
| Type of the last known pregnancy or GTD | Full-term pregnancy (2/3)/molar pregnancy/spontaneous abortion | Full-term pregnancy (67%)/spontaneous abortion/molar pregnancy | Hydatidiform mole (50%)/full-term pregnancy | Therapeutic abortion/cesarean delivery | Normal gestation/molar pregnancy |
| Latency | 12-18 months | 1-18 years | Weeks to several years | 2-108 months | |
| Clinical presentation | History of missed abortion/abnormal uterine bleeding/amenorrhea/uterine enlargement | Abnormal uterine bleeding | Abnormal uterine bleeding/hemorrhage (at ectopic or metastatic sites) | Incidental findings | Asymptomatic/abnormal uterine bleeding |
| Serum β-hCG | Mild to moderate (<2000 UI/ml) | Mild to moderate (<2000 UI/ml) | High (>10000 UI/ml) | Normal levels | Normal levels |
| PSTT | ETT | Choriocarcinoma | PSN /APSN | Exaggerated placental site reaction | |
| Location | Uterine corpus/lower uterine segment. Extrauterine: very rare | Uterine corpus/lower uterine segment and cervix (50%)/fallopian tube/ovary/peritoneum | Uterus+++. Ectopic and metastatic locations have been reported: fallopian tube, ovary, cervix, lung, liver, kidney, and spleen | Uterus+++. Ectopic pregnancy locations (rare) | Uterus+++. Ectopic pregnancy locations (rare) |
| Shape | Nodular mass + well-circumscribed | Discrete nodular or cystic mass | Aggressive mass with an irregular contour | No lesion/solitary or multiple lesions | No macroscopic lesion |
| Consistency | Solid | Solid or cystic | Soft and friable | - | - |
| Color | White to yellow | Beige to brown | Dark red+++ | Yellow, beige | - |
| Size | 1-10 cm | 0.5-4 cm | From microscopic to extensive mass+++ | 4-10 mm | - |
| Invasion | Deep myometrium (50%)/serosa (10%). Rarely board ligament and adnexa | Deep myometrium. Surrounding structures | Deep myometrium invasion/uterine perforation | Superficial myometrium | - |
| Hemorrhage | Focal | +++ | +++ | - | - |
| Necrosis | Focal (50%) | +++ | +++ | + | - |
| PSTT | ETT | Choriocarcinoma | PSN/APSN | Exaggerated placental site reaction | |
| Architecture | Sheets+++ | Nests/cords/masses | Compact masses of mononuclear cells surrounded by multinuclear cells | Clusters/cords/single cells | Cords/small nests |
| Surrounding tissue | Infiltration of endometrium and myometrium | Well-circumscribed +/- peripheric focal infiltration | Infiltration and destruction | Well-circumscribed | Infiltration of endometrium and myometrium with preserved architecture |
| Type of cells | Implantation site IT | Chorionic-type intermediate trophoblast | ST/CT/IT | Chorionic-type intermediate trophoblast | Implantation site IT |
| Nuclei | Hyperchromatic Irregular contours. Nuclear grooves/pseudo inclusions | Small and round/nucleoli+++ | Pleomorphic/granular chromatin +/- nucleoli | Small and uniform++/+/-large, irregular, hyperchromatic +/-multinucleated cells | hyperchromatic + Irregular contours |
| Cytoplasm | Eosinophilic to amphophilic/clear | Granular eosinophilic/clear + well-defined cell membranes | Mononucleated cells: eosinophilic/clear. Multinucleated cells: markedly eosinophilic | Small cells: clear. Large cells: eosinophilic to amphophilic | Eosinophilic and abundant |
| Mitoses | 2-4/10 HPF | 0-9 mitoses/10 HPF | +++ | Low mitotic activity in PSN <5 mm. Increased in PSN >5 mm. | Absent |
| Necrosis | - | +++ | +++ | - | - |
| Hemorrhage | +/- | +++ | - | - | |
| Vascular features | Infiltration of vessel walls with fibrinoid deposition | Central blood vessel in tumor nests +/- fibrinoid deposits | Vasculogenic mimicry* | - | infiltration of vessel walls |
| Calcifications | - | +++ | - | - | - |
| Other characteristics | - | Re-epithelialization of endocervical/endometrial surfaces (specific). Eosinophilic hyaline-like material (resembles keratin). Decidualized stromal cells | - | Central hyalinized extracellular matrix | Chorionic villi are present |
| PSTT | ETT | Choriocarcinoma | PSN/APSN | Exaggerated placental site reaction | |
| CK | Diffuse positivity | Diffuse positivity | Diffuse positivity | Diffuse positivity | Diffuse positivity |
| HSD3B1 | Diffuse positivity | Diffuse positivity | Diffuse positivity | Diffuse positivity | Diffuse positivity |
| P63 | Negative | Positive | Focally positive | Positive | Negative |
| HPL | Positive | Negative/focally positive | Focally positive | Negative/focally positive | Positive |
| β-hCG | Negative/focally positive (syncytiotrophoblast-like cells) | Negative/focally positive (<2%) | Diffuse positivity (ST) | Negative/focal and weak positivity | Negative/focally positive |
| Cyclin E | Diffuse positivity | Negative/focally positive | |||
| Ki67 | >10% | >12% | >50% of mononucleated cells | <8% | <1% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Trophoblastic Disease Studies · Prenatal Screening and Diagnostics · Ectopic Pregnancy Diagnosis and Management
Introduction
Placental site trophoblastic tumor (PSTT) is a rare neoplasm that constitutes approximately 1-2% of all gestational trophoblastic tumors, with an incidence estimated at one to five cases per 100,000 pregnancies [1,2]. It comprises neoplastic implantation site intermediate trophoblastic cells [3]. Some researchers propose that this tumor originates from neoplastic cytotrophoblastic cells, which subsequently differentiate into the intermediate trophoblastic cells characteristic of the implantation site [4].
First described in 1895, this tumor was initially referred to as “atypical chorioepithelioma.” Over time, its understanding evolved, and it was reclassified under its current terminology to reflect its unique histological and biological characteristics better [3].
PSTTs are distinct from other types of gestational trophoblastic diseases due to their clinical behavior and cellular origins, necessitating specific diagnostic and therapeutic approaches [5].
This article provides an in-depth analysis of the clinical, macroscopic, histological, and immunohistochemical aspects of PSTT and its differential diagnoses, beginning with a case report.
Case presentation
We report a case of a 29-year-old woman (G3P2) diagnosed with a hydatidiform mole in 2021. She underwent two aspirations; pathological results favored a complete hydatidiform mole. Persistent metrorrhagia following aspirations led to a third procedure, which confirmed the diagnosis of a persistent hydatidiform mole.
Initially, the β-human chorionic gonadotropin (β-hCG) level was 145 mIU/mL, and the patient began chemotherapy with methotrexate, which resulted in the negativization of the β-hCG level (3 mIU/mL).
However, one year later, her β-hCG levels began to rise (155 mUI/ml), leading to a fourth aspiration, which was initially misdiagnosed as a pregnancy. However, the pathology results did not show evidence of pregnancy or any signs of a mole.
The patient underwent a pelvic MRI, which was suggestive of persistent trophoblastic disease (Figures 1, 2).
MRI sagittal T1-weighted image showing a globular uterus with a posterior and left lateral corporeal multilocular mass that is poorly defined and hypointense (red arrow).
MRI coronal T2-weighted image showing heterogeneous hyperintensity of the mass (red arrow).
She was then referred to oncology, where she underwent a polychemotherapy protocol (etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine (EMA-CO)) consisting of six cycles, with the last cycle administered on December 20, 2023. Subsequent monitoring showed a decrease in β-hCG levels (3.81 mUI/ml), followed by a plateau (5.6-9 mUI/ml).
The follow-up MRI showed near-stability of the lesion process infiltrating the myometrium, consistent with persistent trophoblastic disease, leading to the decision to perform a hysterectomy (Figure 3).
Radiological image revealing the persistence of the lesion process after chemotherapy (red arrow).
Macroscopic examination revealed a whitish lesion at the uterine fundus, with septations and a soft consistency (Figure 4).
Macroscopic view showing a nodular lesion at the uterine fundus.
Histological examination of the samples taken from the lesion revealed a well-defined tumor proliferation composed of intermediate trophoblastic-like cells arranged in clusters, cords, and nests (Figure 5). More peripherally, the cells become isolated, fusiform, and infiltrate between smooth muscle cells (Figure 6). The tumor cells were polygonal with nuclei that were typically round to ovoid, occasionally with irregular contours, and contained vesicular or hyperchromatic chromatin. They were surrounded by abundant cytoplasm that varied between amphophilic and eosinophilic staining.
Histological image showing tumor proliferation arranged in clusters, cords, and nests (hematoxylin-eosin-saffron, x10).
At the periphery, tumor cells infiltrate between the smooth muscle fibers (hematoxylin-eosin-saffron, x20).
Multinucleated cells were occasionally present. The tumor cells frequently wrapped around vascular structures, replacing the vessel wall, and were associated with eosinophilic fibrinoid deposits encircling the vessels (Figure 7).
Tumor cells are polygonal with vesicular nuclei and eosinophilic cytoplasm, replacing the vascular walls in some areas with the presence of fibrinoid deposits surrounding the vascular structures (hematoxylin-eosin-saffron, x10).
Mitoses were observed at a rate of approximately five per 10 high-power fields (HPF).
An immunohistochemical study showed negative labeling of tumor cells with the anti-P63 antibody. The Ki-67 proliferation index of the tumor was estimated at 10% (Figure 8).
Immunohistochemical images showing the absence of anti-P63 labeling (red arrows) and an estimated tumor proliferation index of 10% (hematoxylin, x40).
The patient is currently under regular monitoring of β-hCG levels, which remain negative to date.
Discussion
PSTT affects women of childbearing age, typically between 32 and 35 years, and usually follows a normal pregnancy, though it can also occur after a molar pregnancy, spontaneous abortion, or ectopic pregnancy [2,3]. It often presents with amenorrhea or abnormal bleeding accompanied by abdominal enlargement, which may lead the patient to believe she is pregnant, as was the case with our patient [3]. The β-hCG level is typically low (<1000 mIU/L) [2,3]. PSTT can be diagnosed even after a few months to 20 years of the most recent pregnancy [6].
Through the clinical history and β-hCG levels, the pathologist can gain an initial orientation that may help in suspecting certain types of trophoblastic tumors while excluding others. Table 1 outlines the different clinical aspects of gestational trophoblastic tumors.
Macroscopically, PSTT appears as a distinct nodular mass, which may sometimes have a polypoid shape [3]. It typically measures between 1 and 10 cm, with a whitish-to-yellowish appearance on the cut surface [5]. In approximately 50% of cases, the mass invades the myometrium, reaches the serosa in 10%, and may occasionally extend to the broad ligament and adnexa [5,3]. Areas of hemorrhage and necrosis are observed in about 50% of cases [5].
Table 2 summarizes the different macroscopic features of gestational trophoblastic tumors.
Gestational trophoblastic tumors differ in their cells of origin. Figure 9 summarizes the histological characteristics of the cells that compose the placenta and provides insight into the origins of various trophoblastic tumors [3,6].
Histological characteristics of placental cells and origins of trophoblastic tumors.CT: cytotrophoblast; PSTT: placental site trophoblastic tumor; ETT: epitheloid trophoblastic tumor.
The histological aspect is the cornerstone for differentiating gestational trophoblastic tumors. Table 3 helps compare the histological features of these tumors and allows for a systematic analysis.
The cells of PSTT stain positively for pan-cytokeratin, epithelial membrane antigen (EMA), cytokeratin 18, placental alkaline phosphatase (PLAP), human leukocyte antigen-G (HLA-G) (diffuse staining), Mel-CAM (membranous staining), inhibin (focal), CD10, and HSD3B1, consistent with the general profile of trophoblastic cells [5,10]. They are negative for p63 and show diffuse and intense hPL staining, characteristic of the specific profile of implantation site intermediate trophoblasts (IT) [5,10]. β-hCG is detectable in rare syncytiotrophoblastic cells and some intermediate trophoblastic cells [10]. KI67 expression is estimated at 10-30% [6].
Each gestational trophoblastic tumor has an immunohistochemical panel that guides it toward its identification. Table 4 presents the various immunohistochemical markers of these tumors.
Unlike other trophoblastic tumors, PSTT is relatively resistant to chemotherapy, and surgery remains the main treatment option for patients with diseases confined to the uterus [2].
As reported by Lukinovic et al. [12], PSTT and ETT treatment is guided by two factors: an interval of ≥48 months from the causative pregnancy and stage IV disease. Stage I tumors (confined to the uterus) arising within <48 months are treated with total abdominal hysterectomy, along with retroperitoneal and pelvic lymphadenectomy if suspicious lymph nodes are present, with no need for adjuvant therapy. However, for tumors from a pregnancy >48 months ago or stage II-IV, aggressive platinum-based chemotherapy, including experimental options like high-dose chemotherapy or immunotherapy, is recommended and residual masses following treatment should be surgically removed [13]. Survival is approximately 100% for non-metastatic disease and 50-60% for metastatic disease [12].
The treatment of choriocarcinoma is based on chemotherapy, with a survival rate of 90% for non-metastatic forms and 70% for metastatic forms [10].
There is no targeted treatment for exaggerated placental site, though regular monitoring of β-hCG levels is required [14]. An exaggerated placental site is likely a physiological process that resolves after curettage and is not linked to a higher risk of persistent gestational trophoblastic disease [3].
The treatment of placental site nodules (PSNs) consists of the surgical excision of the nodule, and, for atypical PSNs, follow-up with pelvic MRI imaging is necessary [9].
Finally, Figure 10 summarizes the approach a pathologist may follow when gestational trophoblastic pathology is suspected [3,10].
Methodology in pathological diagnosis of gestational trophoblastic disease.PSTT: placental site trophoblastic tumor; ETT: epitheloid trophoblastic tumor; PSN: placental site nodule; APSN: atypical placental site nodule; IT: intermediate trophoblasts; ST: syncytiotrophoblast; CT: cytotrophoblast; beta-hCG: beta-human chorionic gonadotropin.
Conclusions
Gestational trophoblastic diseases are disorders that can occur following term pregnancies, miscarriages, or molar pregnancies. The pathologist plays a crucial role in distinguishing the type of disease, which is essential for therapeutic decision-making, surveillance, and prognosis prediction. This highlights the need for a thorough analysis combining clinical findings, radiology, gross examination, histology, and immunohistochemistry. Such an integrative approach is critical to ensure accurate diagnosis and appropriate management of these conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Placental site trophoblastic tumor J Cancer Res Clin Oncol Behtash N Karimi Zarchi M 1613420081770142710.1007/s 00432-007-0208-y PMC 12161738 · doi ↗ · pubmed ↗
- 2Placental site trophoblastic tumor: a case report and review of the literature J Radiol Case Rep Lucas R Cunha TM Santos FB 142292015 https://pubmed.ncbi.nlm.nih.gov/26622924/10.3941/jrcr.v 9i 4.2146 PMC 463836526622924 · doi ↗ · pubmed ↗
- 3Blaustein's Pathology of the Female Genital Tract, 7th Edition Kurman RJ Ellenson LH Ronnett BM New York, NY Springer 2019
- 4Gestational trophoblastic neoplasia—pathogenesis and potential therapeutic targets Lancet Oncol Shih IM 6426200710.1016/S 1470-2045(07)70204-817613426 · doi ↗ · pubmed ↗
- 5Placental site trophoblastic tumor (PSTT): a case report and review of the literature Pathologica Zampacorta C Pasciuto MP Ferro B 11111611520233711462910.32074/1591-951X-873PMC 10462996 · doi ↗ · pubmed ↗
- 6Female Genital Tumours: WHO Classification of Tumours, 5th Edition Kurman RJ Ellenson LH Ronnett BM Geneva, Switzerland World Health Organization 2020 https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Female-Genital-Tumours-2020
- 7Placental site trophoblastic tumour and epithelioid trophoblastic tumour Best Pract Res Clin Obstet Gynaecol Hancock BW Tidy J 1311487420213313921210.1016/j.bpobgyn.2020.10.004 · doi ↗ · pubmed ↗
- 8Pathology of gestational trophoblastic disease (GTD)Best Pract Res Clin Obstet Gynaecol Kaur B 3287420213421902110.1016/j.bpobgyn.2021.02.005 · doi ↗ · pubmed ↗