Invasion of Diffuse Large B-Cell Lymphoma to Right Axillary Arterial Graft
Koki Yokawa, Yukihiro Imai, Taku Nakagawa, Makoto Kusakizako, Yosuke Tanaka, Tomonori Higuma, Kazunori Yoshida, Yoshihiro Oshima, Hidefumi Obo, Hidetaka Wakiyama

TL;DR
A rare case of diffuse large B-cell lymphoma invading an arterial graft in a patient with a history of aortic surgery is reported.
Contribution
This case highlights the rarity and diagnostic importance of DLBCL originating around a surgical graft.
Findings
DLBCL was diagnosed around a right axillary arterial graft in a 76-year-old male.
The patient's condition precluded chemotherapy and he passed away within 3 months.
Such lymphoma origin around grafts is extremely rare but important for differential diagnosis.
Abstract
A 76-year-old male patient, who had undergone right axillary artery bypass and arch replacement surgery for retrograde type A aortic dissection after thoracic endovascular aortic repair 2 years ago, was referred to our department with complaints of swelling and pain in the right subclavian region. A computed tomography scan suspected an abscess around the bypass graft; however, the culture was negative. Pathological examination indicated a diffuse large B-cell lymphoma (DLBCL) diagnosis. Chemotherapy was not indicated due to the patient’s condition, and he passed away after 3 months. DLBCL originating around a graft is extremely rare but crucial for differential diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
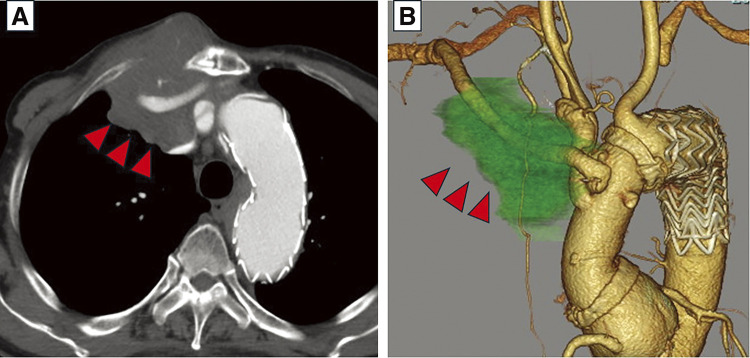 Figure 1
Figure 1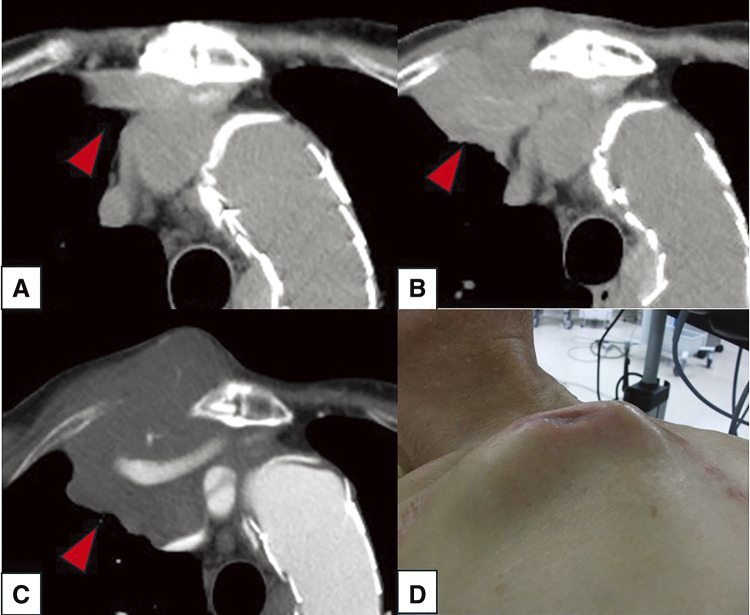 Figure 2
Figure 2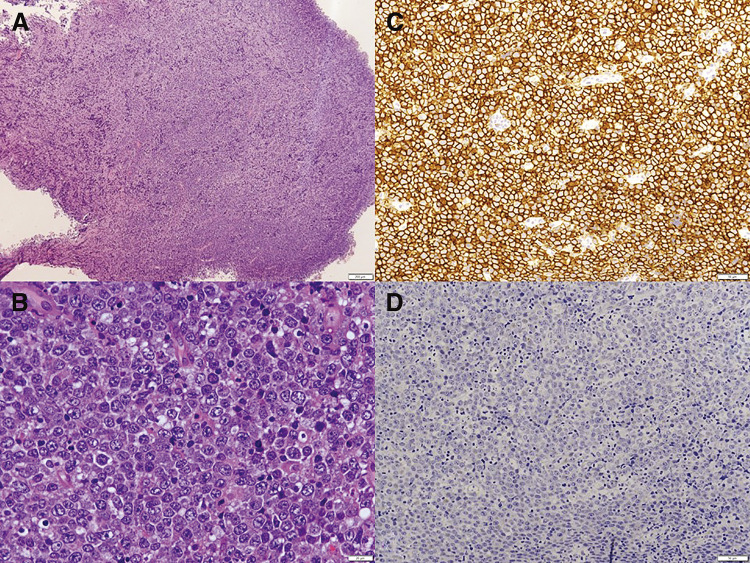 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · CNS Lymphoma Diagnosis and Treatment
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most representative type of aggressive lymphoma and is known to metastasize throughout the body. However, metastasis to the arterial system is extremely rare.
Case Report
A 76-year-old male patient was referred to our department with a chief complaint of swelling and pain in the right anterior chest that persisted for 1 week. He had undergone zone 2 thoracic endovascular aortic repair (TEVAR) and left common carotid artery to left axillary artery bypass surgery for a thoracic aortic aneurysm 6 years ago. He had an aortic valve replacement and tricuspid annuloplasty for aortic regurgitation and tricuspid regurgitation 5 years ago. He underwent right axillary artery to ascending aorta bypass surgery and partial arch replacement for retrograde type A aortic dissection after TEVAR in our department 2 years ago. The graft used for the bypass to the right axillary artery was the 8 mm side branch of J Graft (Japan Lifeline Co., Ltd., Tokyo, Japan) used for the partial arch replacement. The patient had chronic atrial fibrillation, in addition to the aortic and cardiac surgeries, and was on anticoagulant therapy. Additionally, he received radiation therapy for laryngeal cancer 12 years ago. An adenoma was found in the left thyroid lobe, and he had hypothyroidism, which was under follow-up.
The laboratory test revealed only an elevated inflammatory response (C-reactive protein: 2.45 mg/dL) and mild renal dysfunction (creatinine:1.13 mg/dL; estimated glomerular filtration rate: 49%). The white blood cell count was 6333/mL, with monocytes accounting for 13.3%. Lactate dehydrogenase and alkaline phosphatase levels were elevated, measuring 308 and 409 U/L, respectively. Trans-thoracic echocardiography detected left ventricular enlargement (LVDd/Ds: 56.4 mm/39.3 mm), moderate mitral insufficiency, and a decreased ejection fraction (48%). No prosthetic valve dysfunction was observed. Computed tomography (CT) examination revealed a rapidly enlarging mass around the prosthetic graft in the right anterior chest (Figs. 1 and 2).
Fig. 1 Preoperative CT revealing a mass surrounding the graft to the right axillary artery. (A) Axial CT imaging showing tumor progression (indicated by red arrowheads). (B) 3D CT image highlighting the tumor with red arrowheads and light green coloring. CT: computed tomography
Fig. 2 Changes in the mass on preoperative computed tomography scan. The red arrowhead indicates the enlargement of the anterior mediastinal mass during this course. (A) 13 months before admission, (B) 1 month before admission, (C) current admission, and (D) preoperative external findings.
CT examination could not rule out a prosthetic graft infection; thus, we decided to proceed with urgent open drainage surgery of the anterior chest. Intraoperative results revealed no obvious abscess formation, but a grayish-white, friable, gelatinous mass. Completely resecting this tumorous lesion was challenging; hence, the wound was managed in an open state until obtaining a definitive diagnosis. Bacterial infection was ruled out, but findings were indicative of malignant lymphoma. The bacterial culture of the excised specimen was negative, and pathological examination confirmed a DLBCL diagnosis. Histopathological examination of resected tissue indicated diffuse infiltration of large lymphocytes with granular chromatin and scattered mitoses. Small lymphocytes and nuclear dust were scattered between large lymphocytes. Immunohistochemistry revealed positive staining for CD20, bcl2, and MUM1, whereas CD3, CD10, CD30, and bcl6 were negative. These results revealed that the tumor was DLBCL non-germinal center B-cell type. Epstein–Barr (EB) virus-encoded small RNA in situ hybridization was negative (Fig. 3). The tumorous lesion in the anterior chest revealed a tendency to enlarge during the postoperative course. No results indicated metastasis to other organs. The clinical stage was deemed to involve local infiltration when consulted with a hematologist, equivalent to stage IV. The patient’s declining performance status during hospitalization, decreased cardiac function, chronic kidney disease, and other organ impairments increased the risk of complications from chemotherapy while indicating curative chemotherapy. Full-dose treatment was difficult, thereby decreasing the likelihood of disease cure. The best supportive care approach was adopted after discussions with the patient and family. The patient passed away 3 months post-drainage surgery.
Fig. 3 Pathological findings. (A) HE stain (×4), (B) HE stain (×50), (C) CD20 (×20), and (D) EB virus-encoded small RNA (×20). Immunohistochemistry showed positive staining for CD20, and EB virus encoded small RNA in situ hybridization was negative. HE: hematoxylin and eosin; EB: Epstein–Barr; RNA: ribonucleic acid
Discussion
Primary malignant lymphoma originating from the chest wall accounts for approximately 0.3%–1.0% of extranodal lymphoma. This lymphoma is mostly associated with underlying diseases, such as tuberculous pleurisy or pyothorax after artificial pneumothorax, and is caused by pleural chronic inflammation.^1)^ However, the present case demonstrated none of these predominant features. In this case, the lymphoma had progressed along the artificial graft, and chronic inflammation caused by the artificial graft cannot be completely ruled out as contributing to malignant lymphoma development. Breast implant-associated anaplastic large cell lymphoma is reported as a lymphoma related to artificial materials. The biofilm surrounding the textured implants may stimulate lymphocyte production, which triggers an inflammation cycle that ultimately causes breast implant-associated anaplastic large cell lymphoma.^2)^ However, the pathological results in this case do not match this lymphoma subtype. The cause remains unclear because no reports describe malignant lymphoma occurring around artificial grafts, such as in this case.
If a biopsy via puncture had been considered as a preoperative diagnostic method, the diagnosis could have been made more quickly. Unfortunately, we were unable to perform a postmortem autopsy, and therefore, we could not confirm any pathological findings of malignant lymphoma infiltration into the graft.
Previous reports have described favorable outcomes with aggressive treatment for malignant lymphomas originating from the aorta or heart.^3,4)^ However, chemotherapy was invariably administered in these cases, whereas the patient in our case was unable to undergo chemotherapy and subsequently passed away. This case experienced multiple comorbidities, but the prognosis may have been prolonged if chemotherapy had been administered.
Conclusion
We present a novel case of DLBCL with the appearance of an infected graft after thoracic aortic surgery. DLBCL originating around artificial graft is extremely rare but crucial for differential diagnosis. Aggressive chemotherapy is considered necessary when diagnosing DLBCL if a favorable prognosis is expected.
Declarations
Consent for publication
We have obtained the patient’s consent for publication.
Ethics approval
This study was approved by the Institutional Review Board with approval number 2024-22.
Funding
No funding was received for this study.
Disclosure statement
The authors have nothing to disclose.
Author contributions
Manuscript preparation: KY
Critical review and revision: all authors
Final approval of the article: all authors
Accountability for all aspects of the work: all authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iwasa Y, Okada A, Takenaka H, et al. Primary malignant lymphoma originating from the chest wall without preceding pleural disease. Intern Med 2017; 56: 681–6.28321070 10.2169/internalmedicine.56.7053 PMC 5410480 · doi ↗ · pubmed ↗
- 2Elameen AM, Al Marakby MA, Atta TI, et al. The risk of breast implant-associated anaplastic large cell lymphoma; a systematic review and meta-analysis. Aesthetic Plast Surg 2024; 48: 5315–28.38724638 10.1007/s 00266-024-03956-9PMC 11750888 · doi ↗ · pubmed ↗
- 3Jean-Marie E, Gillombardo CB, Baeza C, et al. Diffuse large B-cell lymphoma mimicking intramural hematoma of the thoracic aorta. JACC Case Rep 2023; 15: 101858.37283827 10.1016/j.jaccas.2023.101858 PMC 10240261 · doi ↗ · pubmed ↗
- 4Ellen S, Emma H. Primary cardiac lymphoma: a case report. Eur Heart J Case Rep 2023; 7: ytad 175.37090756 10.1093/ehjcr/ytad 175PMC 10118624 · doi ↗ · pubmed ↗