Incidence and Factors Associated with Self-Reported Skin Symptoms of Allergic Reactions to COVID-19 Vaccines
Karnsinee Thanborisutkul, Prapasri Kulalert, Kanthida Methaset, Sira Nanthapisal, Tibet Chunthatikul, Nathamon Phangpanya, Phenpraphatson Charoenying, Worakamon Atsawutmangkru, Suphatsara Srijaroen, Patcharaporn Punyashthira, Orapan Poachanukoon

TL;DR
This study found that allergic skin reactions to COVID-19 vaccines are rare in Thailand, with higher risk among younger people, women, and those with a history of allergies.
Contribution
The study provides new insights into the incidence and risk factors for allergic reactions to inactivated and viral vector COVID-19 vaccines in a Thai population.
Findings
The incidence of self-reported allergic reactions was 0.85% among 215,079 vaccine doses.
Female sex and a history of allergic rhinitis were the strongest risk factors for allergic reactions.
Younger individuals and those with a family history of allergies were also at higher risk.
Abstract
Background: Few reports exist regarding the incidence and factors associated with allergic reactions to COVID-19 vaccines during post-marketing surveillance, especially for inactivated whole virus or viral vector vaccines. We aimed to determine the incidence and factors associated with self-reported allergic reactions to COVID-19 vaccines in the Thai population. Methods: A cross-sectional case-control study was conducted via telephone-based interviews. Cases were defined as physician-confirmed, self-reported vaccine recipients diagnosed with non-severe immediate allergic reactions, anaphylaxis, or delayed allergic reactions. Controls were randomly sampled from vaccinated individuals who reported no adverse events and were matched by the type of vaccine (1 case:2 controls). Demographic information and the history of atopic diseases were collected in both groups. Conditional logistic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
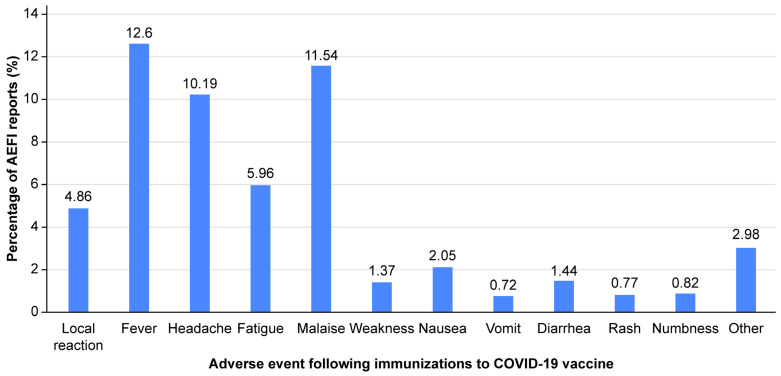 Figure 1
Figure 1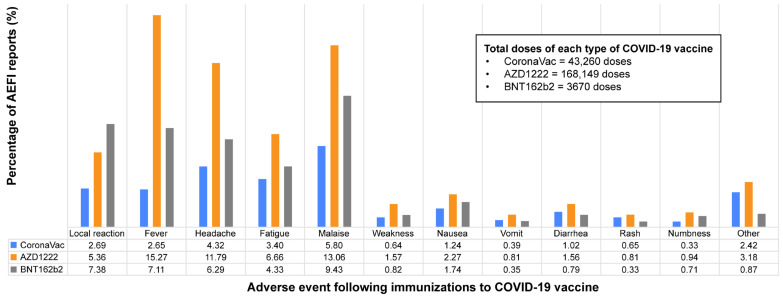 Figure 2
Figure 2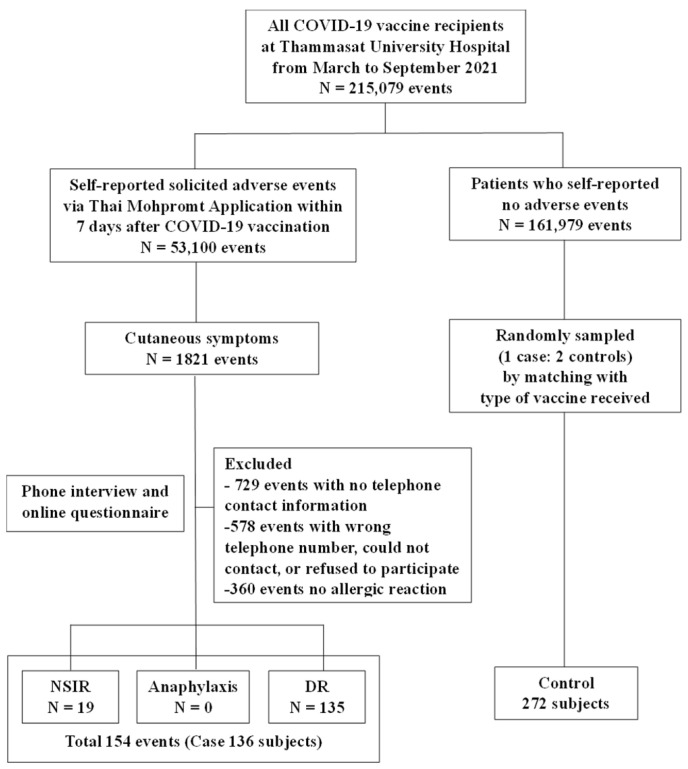 Figure 3
Figure 3- —Faculty of medicine, Thammasat University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Drug-Induced Adverse Reactions · Allergic Rhinitis and Sensitization
1. Introduction
The outbreak of coronavirus disease 2019 (COVID-19) that emerged in Wuhan, China, was first identified in December 2019 [1]. It rapidly spread worldwide and became a global pandemic that has impacted health and global economies resulting in morbidity and mortality [2,3,4]. Currently, several types of COVID-19 vaccines are available that include inactivated vaccines (e.g., CoronaVac), mRNA vaccines, such as BNT162b2 (Pfizer BioNTech, London, UK) and mRNA-1273 (Moderna, Cambridge, MA, USA), and vector vaccines, such as ChAdOX1 nCOV-19 (Oxford-AstraZeneca, Cambridge, UK) [5]. They have shown efficacy in preventing COVID-19 infections [6,7,8,9].
In addition to efficacy, adverse events following immunization (AEFI) to the COVID-19 vaccines are an important issue associated with COVID-19 vaccine hesitancy related to patient preference and physician advice. From the clinical trials, the COVID-19 vaccines showed a safety profile with a low incidence of AEFI. Polack et al. [6] conducted a multinational, placebo-controlled, observer-blinded, efficacy and safety trial of the BNT162b2 vaccine and reported that local reactions were often reported in the BNT162b2 group. Mild-to-moderate pain at the injection site was the most common local reaction. Likewise, Baden et al. [7] conducted a randomized, observer-blinded, placebo-controlled trial for the efficacy and safety of the mRNA-1273 vaccine and showed that solicited local and systemic adverse events occurred more frequently in the mRNA-1273 group than in the placebo group. Serious adverse events were rare, and the incidence was similar in the two groups. Similarly, Falsey et al. [8] reported that AZD1222 was safe, with low incidences of serious and medically attended adverse events. The most common adverse events were general pain, headache, injection-site pain, and fatigue. Durusu et al. [9] reported that CoronaVac has a good safety and tolerability profile, fatigue was the most common systemic adverse event, and injection-site pain was the most frequent local adverse event, respectively.
Post-marketing surveillance is the practice of monitoring the safety of a pharmaceutical drug after its release on the market. During post-marketing surveillance from December 2020 through January 2021, the Centers for Disease Control and Prevention reported that the anaphylaxis cases following BNT162b2 and mRNA-1273 vaccinations had incidence rates of 4.7 and 2.5 cases per million doses, respectively [10]. From February to March 2021 in Japan, the Committee on Drug Safety of the Pharmaceutical Affairs and Food Sanitation Council and the Vaccine Adverse Reaction Review Committee evaluated cases of suspected event reports of anaphylaxis after the BNT162b2 vaccination. They reported an incidence rate of 8.1 cases per 100,000 doses of suspected vaccine event reports [11]. Several studies have reported that the factors associated with allergic reactions to the mRNA COVID-19 vaccines included a younger age, female, and personal history of allergic disease [12,13,14,15].
However, to the best of our knowledge, studies have not reported the incidences and factors associated with allergic reactions due to inactivated vaccines (e.g., CoronaVac) and vector vaccines, such as ChAdOX1 nCOV-19 (Oxford-AstraZeneca), during the post-marketing phase. Filling this gap in knowledge will help develop the surveillance and monitoring of COVID-19 recipients with risk factors.
The AZD1222 and CoronaVac vaccines were available in Thailand and administrated as the mainstay vaccines in the early period of the pandemic. Thammasat University Hospital is one of the mass vaccination centers in Thailand where more than 200,000 recipients received vaccines including CoronaVac, AZD1222, and BNT162b2 between 1 March and 30 September 2020. Therefore, we aimed to determine the incidence of self-reported AEFI and self-reported allergic reactions. We also explored the factors associated with self-reported allergic reactions to COVID-19 vaccines.
2. Materials and Methods
2.1. Study Design and Populations
A cross-sectional study was conducted to collect data on self-reported AEFI to COVID-19 vaccines from the Thai application database, which was developed by The Ministry of Public Health of Thailand. All COVID-19 recipients aged ≥ 12 years old who received the CoronaVac, AZD1222, or BNT162b2 COVID-19 vaccines at Thammasat University Hospital between 1 March and 30 September 2021, were enrolled.
All recipients who reported cutaneous symptoms were contacted via telephone by physicians to confirm the allergic reactions. The relevant clinical findings that included symptoms, onset of symptoms after vaccination, and data on medications received were also collected. Self-reported allergic reactions were classified as non-severe, immediate allergic reaction (NSIR) (e.g., urticaria and/or angioedema < 4 h), anaphylaxis, or delayed allergic reaction (DR) (e.g., urticaria ≥ 4 h or maculopapular rash) [16,17].
Then, we conducted a case-control study to explore the factors associated with self-reported allergic reactions to COVID-19 vaccines. Cases were defined as physician-confirmed self-reported vaccine recipients diagnosed as NSIR, anaphylaxis, or DR [16,17]. If a recipient showed the same type of allergic reaction at the first and second dose of vaccination, data for only the first dose were collected. If the recipients reported different types of allergic reactions at the first and second doses, the data of each dose were recorded. Controls were randomly sampled from those who reported no AEFI and matched with the case by the type of vaccine received (1 case:2 controls).
2.2. Data Collection
Both case and control groups were interviewed via telephone and online questionnaires for baseline characteristic collection that included age, gender, body weight, height, personal history of atopic disease (i.e., asthma, allergic rhinitis, atopic dermatitis, food allergy, and drug allergy), or family history of allergic disease.
Adverse events to COVID-19 vaccines were defined based on safety assessments for the clinical development of COVID-19 vaccines licensed by in the US FDA. COVID-19 vaccine adverse events were classified as the following: (1) solicited adverse events that were predictable following immunization and the reactogenicity of the vaccine reported by the vaccine recipient within 7 days after vaccination, and the reactions were divided into local and systemic reactions; (2) unsolicited adverse events that were unpredictable and reported by the vaccine recipients or healthcare workers within 28 days after vaccination; (3) medically attended adverse events; (4) serious adverse events that were life-threatening adverse events that required hospitalization and caused disability or a substantial disruption of the ability to conduct normal life function or death [18].
Allergic reactions were classified into three types based on the characteristics of cutaneous symptoms and the timing of onset after vaccination as follows: (1) non-severe, immediate allergic reactions (NSIRs) included acute onset urticaria or angioedema occurring within 4 h of vaccination [16]. Urticaria was characterized by the sudden appearance of wheals with circumscribed erythema and edema of the superficial dermis in variable numbers and sizes, with or without angioedema. Angioedema involved edema in the deeper dermis and subcutis, often affecting the face, as well as the buccal mucosa, tongue, larynx, and pharynx [17]. (2) Anaphylaxis was defined as the acute onset of urticaria or angioedema accompanied by systemic involvement, such as cardiovascular, respiratory, or gastrointestinal symptoms following vaccination. Confirmatory anaphylaxis was diagnosed based on the Brighton Collaboration definition [19]. (3) Delayed allergic reactions (DRs) included the delayed onset of urticaria or angioedema occurring more than 4 h after vaccination [16], or maculopapular eruptions occurring within 7 days following vaccination. Maculopapular exanthem was characterized by macular or papular rashes, or both, accompanied by pruritus without other systemic involvement [17].
2.3. Study Variables
Candidate factors associated with self-reported allergic reactions to COVID-19 vaccines were identified from the literature review. Previous studies reported a younger age [12,20], female [12,13], and personal history of atopic disease [12,13,14,15] as potential risk factors for allergic reactions to COVID-19 vaccines. Also included were a personal history of drug or vaccine allergy [21], family history of allergic disease in first-degree relatives [22], increased risk of drug allergy. Therefore, we selected these risk factors as interesting variables.
2.4. Statistical Analysis
The incidence of self-reported allergic reactions to vaccines used the number of COVID-19 vaccine recipients who reported allergic reactions between 1 March and 30 September 2021, at our center as the numerator and the total number of vaccine recipients within the same period as the denominator. The frequency and percentage described the categorical variables, and the mean and standard deviation or median and interquartile range (IQR) were used to describe continuous variables as appropriate. Categorical data were analyzed based on Fisher’s exact test. An independent t-test was used for continuous data with a normal distribution, and the Wilcoxon rank sum test was used for skewed data. A two-sided p-value < 0.05 was considered statistically significant. Conditional logistic regression was used to explore the factors associated with allergic reactions. Variables that were potential risk factors associated with allergic reactions to COVID-19 vaccines, as observed via univariable analysis (p < 0.05), were further processed through multivariable analysis and are presented as the adjusted odds ratio (aOR) with the 95% confidence interval (CI). All statistical analyses were performed using Stata version 17 (StataCorp, Lakeway, TX, USA).
3. Results
3.1. Incidence of Self-Reported AEFI
A total of 215,079 doses of COVID-19 vaccines were administered to Thai people at Thammasat University Hospital between 1 March and 30 September 2021. Fifty-three thousand and one hundred self-reported SAEs were reported via the application within 7 days after vaccination. The overall incidence rate of self-reported SAEs to COVID-19 vaccines was 24.69%. All self-reported SAEs following all types of vaccine are shown (Figure 1). The three most common AEFIs were fever, malaise, and headache in descending order. Of the 43,260 doses of CoronaVac, the three most common AEFIs were malaise, headache, and fatigue in descending order. In the AZD1222 group with 168,149 vaccine doses, the three most common AEFIs were fever, malaise, and headache. Of the 3670 doses of the BNT162b2 vaccine, the three most common AEFIs were malaise, local reaction, and fever (Figure 2).
3.2. Incidence of Self-Reported Allergic Reactions
During the study period, a total of 1821 events of self-reported cutaneous symptoms were reported via the application. The incidence rate of self-reported skin symptoms of allergic reactions to COVID-19 vaccines was 846.67 (0.85%) per 100,000 injections. A total of 1821 events of self-reported cutaneous symptoms were reported via the application, and of the 1307 events, 729 events were excluded due to no telephone contact information, and 578 events were excluded due to wrong telephone numbers, could not contact, or the recipients refused to participate. Five hundred and fourteen events were interviewed and confirmed as allergic reactions by physicians. However, 360 events were not enrolled due to no allergic reaction after confirmation by a physician. Finally, we confirmed 154 events from 136 cases as allergic reactions that included 19 (12.33%) NSIRs and 135 (87.66%) DRs. Anaphylaxis was not reported in this study (Figure 3).
3.3. Baseline Characteristics of the Participants
A total of 408 participants, including cases and controls (1 case:2 controls), were enrolled (136 cases and 272 controls). Among both groups, the most common type of administered vaccine was AZD1222. The median (IQR) ages in the case and control groups were 36 (28, 49) and 45 (31, 56) years, respectively, which were significantly different (p < 0.001), and females predominated in the case group (p < 0.001). Furthermore, a family history of allergic disease in first-degree relatives and a personal history of all allergic diseases, except asthma, were also statistically significantly different (p < 0.001) (Table 1).
3.4. Risk Factors for Self-Reported Skin Symptoms of Allergic Reactions to COVID-19 Vaccines
In the univariable analysis, recipients with allergic reactions to COVID-19 vaccines were significantly younger than 60 years (p < 0.001), female (p < 0.001) and had histories of allergic rhinitis (p < 0.001), atopic dermatitis (p < 0.001), and food allergy (p < 0.001). Furthermore, the vaccine recipients with allergic reactions had a previous vaccine or drug allergy (p = 0.021) and had a family history of allergic disease in first-degree relatives (p < 0.001). All observed variables were potentially associated with allergic reactions to COVID-19 vaccines (Table 2).
In the multivariable conditional logistic regression analysis, the significant variables associated with allergic reactions included age < 60 years (aOR 3.53; 95% CI: 1.43–8.70; p = 0.006), female (aOR 8.33; 95% CI: 4.35–15.94; p < 0.001), allergic rhinitis (aOR 4.32; 95% CI: 2.43–7.69; p < 0.001), atopic dermatitis (aOR 4.27; 95% CI: 1.74–10.47; p = 0.002), food allergy (aOR 6.53; 95% CI: 2.42–17.61; p < 0.001), and had a family history of allergic disease (aOR 2.14; 95% CI: 1.12–4.08; p = 0.021) (Table 3).
4. Discussion
This is the first population-based study conducted during the post-marketing surveillance of COVID-19 vaccines in the Thai population and included three types of vaccines (BNT162b2, AZD1222, and CoronaVac). Our study revealed a low incidence rate of self-reported allergic reactions to COVID-19 vaccines, and anaphylactic reactions were not reported, which was similar to the estimated incidence rate reported previously. Imai et al. [13] recruited 614,151 mRNA-1723 vaccine recipients from a mass vaccination center in Japan and reported low incidence rates of immediate hypersensitivity reaction (IHSR) and anaphylaxis. The incidence rate of IHSR per million doses was 266 cases, and anaphylaxis was 2 cases, respectively. Macy et al. also conducted a retrospective review of electronic health records, and there were only 2 of 606,273 (0.00033%) vaccinations, and they reported that the population-based incidence of confirming anaphylaxis was 3.29 per million vaccine doses [23].
In contrast, Blumenthal et al. [24] conducted a questionnaire-based study, including 64,900 healthcare employees at Mass General Brigham. They reported that the incidence of allergic symptoms after the first dose of mRNA COVID-19 vaccination was 2.1%, and anaphylactic reactions occurred at a rate of 2.47 per 10,000 injections. Shavit et al. [14] prospectively performed a study in Israel and documented rates of allergic reactions of 1.4% and anaphylaxis of 0.7% in 429 highly allergic patients who received BNT162b2 vaccines. The incidence rates of allergic reactions in our study were significantly lower than those reported in those studies, which was possibly due to different methods among the studies. In addition to the self-reported allergic reactions of our participants, we confirmed the reactions through telephone follow-up by physicians to increase the reliability of the allergic reaction evaluation.
Currently, the known factors associated with an increased risk of allergic reactions to COVID-19 vaccines include a younger age [12,20,23], female [12,13,23,25], and a personal history of allergic disease [21,23,25]. However, these findings explored associating factors with allergic reactions to mRNA COVID-19 vaccines. We explored the factors associated with self-reported allergic reactions to COVID-19 vaccines, including viral vector and inactivated vaccines. By comparing clinical characteristics in this study between recipients with and without reported allergic reactions, we identified four factors associated with self-reported allergic reactions to COVID-19 vaccines: (1) younger age (<60 years); (2) female; (3) personal history of allergic disease (i.e., allergic rhinitis, atopic dermatitis, food allergy); and (4) family history of allergic disease in first-degree relatives.
Of the four factors, being female was the most potent predictor of the development of allergic reactions following COVID-19 vaccination (OR 8.33; 95% CI: 4.35–15.94; p < 0.001). This was in concordance with previous studies. Iguchi et al. [11] and Bian et al. [12] reported that anaphylaxis following mRNA vaccination was more commonly observed in females than males. Likewise, Imai et al. [13] documented that female recipients were associated with IHSR after mRNA-1723 administration (OR 3.69; 95% CI: 2.56–5.31; p < 0.001). Being female is also a factor that can predict drug hypersensitivity. Although many reports showed that being female was a significant risk factor for allergic reactions to the COVID-19 vaccine and other drugs, to date, no known pathophysiological evidence has been reported.
Many studies also reported that a younger age was a predictor of allergic reactions to COVID-19 vaccines; however, differences existed in the cut-off ages in these studies. Bian et al. [12] documented that those recipients who reported allergic reactions had a mean age of 45.11 ± 5.6 years vs. 47.01 ± 6.3 years (p < 0.001). Similarly, Paoletti et al. reported that immediate allergic reactions were more frequent in the younger age group [25]. In this current study, we used a cut-off age of 60 years, which is the same for the elderly in Thailand, defined as a high-risk group for COVID-19 infections and receiving priority for vaccination. Our results showed that a younger age was one factor associated with allergic reactions to COVID-19 vaccines (aOR 3.53; 95% CI: 1.43–8.70; p = 0.006).
A personal history of allergic disease was also an important factor that several reports and international guidelines for COVID-19 vaccine allergy management focused on. In this study, we found that allergic rhinitis, atopic dermatitis, and food allergy were related to allergic reactions to COVID-19 vaccines. Similarly, Iguchi et al. [11] and Bian et al. [12] reported that anaphylaxis following mRNA vaccination was more frequently observed in recipients with a prior history of allergy. Desai et al. [15] documented that a pre-existing history of allergy and anaphylaxis had a 2- and 7-times higher incidence rate of anaphylaxis after an mRNA vaccination compared with those without any history of allergy. Likewise, Imai et al. [13] reported that mRNA-1723 recipients who had a history of asthma, atopic dermatitis, and food allergy had a statistically significantly increased risk of developing IHSR. These factors were in concordance with most previous studies that mentioned mRNA COVID-19 vaccine recipients. Interestingly, for our study, most data were collected from the viral-vector-based vaccine and inactivated vaccine. We hypothesize that the predicting factors identified in this current study may be important factors for the prediction of all types of COVID-19 vaccine hypersensitivity reactions. Further studies are needed to provide more data.
A family history of allergy was described as a predictor of drug hypersensitivity. Previously, no data were available on COVID-19 vaccines. This current study is the first to show that a family history of allergic disease in first-degree relatives was also significantly associated with allergic reactions following vaccination (aOR 2.14; 95% CI: 1.12–4.08; p = 0.021).
Some clinically relevant factors have been reported to be associated with allergic reactions to COVID-19 vaccines but did not show statistical significance in our study. For example, it was reported that people with a history of drug allergy had a higher risk of developing allergic reactions following vaccination [21,23]. Similarly, Imai et al. [13] reported that allergic reactions to the mRNA-1723 vaccine were significantly reported by recipients with a prior history of drug allergy (OR 13.32; 95% CI: 7.57–23.44; p < 0.001). Even though a history of drug allergy was not statistically significant in our study, clinical practice should be aware of allergic reactions to COVID-19 vaccines in people with this risk.
Our findings provide the incidence rates of allergic reactions to COVID-19 vaccines that mostly reflect a viral vector-based vaccine and an inactivated vaccine, which differ from previously published studies. Moreover, we identified factors associated with allergic reactions after vaccination to increase the awareness of COVID-19 vaccination in people who have these risk factors.
This study has some strengths. First, it included a large population of more than 200,000 participants. Second, even though several studies on the incidence and factor-related COVID-19 vaccines allergic reactions are available, most of them focused on mRNA vaccines. This study differs from previous studies because it focused on the viral vector-based and inactivated COVID-19 vaccines. Third, this study was one of the few studies that collected data in an Asian country. However, this study also has some limitations. First, some parts of the study involved retrospective data collection, which may be subject to recall bias. Although we made efforts to minimize this bias by providing a questionnaire that included images of all types of cutaneous reactions to aid the participants’ memory, we acknowledge that it is impossible to completely eliminate the risk of recall bias and recognize that some degree of recall bias may still persist. Second, since our outcome was based on self-reported allergic reactions from vaccine recipients, there is a possibility that the incidence rate may have been overestimated. To increase the reliability of these self-reports, we confirmed the allergic reactions via telephone interviews conducted by physicians, using the clinical history, onset of reaction, and type of reaction. However, we acknowledge that despite this confirmation, self-reporting still remains a potential source of bias, and some mild reactions may not have been recorded.
5. Conclusions
COVID-19 vaccines showed a very low incidence rate of self-reported allergic reactions. Allergic reactions were more likely to occur in vaccine recipients who were <60 years old, female, and had a history of atopic disease. Our study suggests that people with these risk factors should be closely monitored after COVID-19 vaccination.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu Y.C. Chen C.S. Chan Y.J. The outbreak of COVID-19: An overview J. Chin. Med. Assoc.20208321722010.1097/JCMA.000000000000027032134861 PMC 7153464 · doi ↗ · pubmed ↗
- 2Huang C. Wang Y. Li X. Ren L. Zhao J. Hu Y. Zhang L. Fan G. Xu J. Gu X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China Lancet 202039549750610.1016/S 0140-6736(20)30183-531986264 PMC 7159299 · doi ↗ · pubmed ↗
- 3Tyrrell C.S.B. Mytton O.T. Gentry S.V. Thomas-Meyer M. Allen J.L.Y. Narula A.A. Mc Grath B. Lupton M. Broadbent J. Ahmed A. Managing intensive care admissions when there are not enough beds during the COVID-19 pandemic: A systematic review Thorax 20217630231210.1136/thoraxjnl-2020-21551833334908 PMC 7892390 · doi ↗ · pubmed ↗
- 4Kontis V. Bennett J.E. Rashid T. Parks R.M. Pearson-Stuttard J. Guillot M. Asaria P. Zhou B. Battaglini M. Corsetti G. Magnitude, demographics and dynamics of the effect of the first wave of the COVID-19 pandemic on all-cause mortality in 21 industrialized countries Nat. Med.2020261919192810.1038/s 41591-020-1112-033057181 PMC 7615092 · doi ↗ · pubmed ↗
- 5Li M. Wang H. Tian L. Pang Z. Yang Q. Huang T. Fan J. Song L. Tong Y. Fan H. COVID-19 vaccine development: Milestones, lessons and prospects Signal Transduct. Target. Ther.202271463550491710.1038/s 41392-022-00996-y PMC 9062866 · doi ↗ · pubmed ↗
- 6Polack F.P. Thomas S.J. Kitchin N. Absalon J. Gurtman A. Lockhart S. Perez J.L. Pérez Marc G. Moreira E.D. Zerbini C. Safety and Efficacy of the BNT 162b 2 m RNA COVID-19 Vaccine N. Engl. J. Med.20203832603261510.1056/NEJ Moa 203457733301246 PMC 7745181 · doi ↗ · pubmed ↗
- 7Baden L.R. El Sahly H.M. Essink B. Kotloff K. Frey S. Novak R. Diemert D. Spector S.A. Rouphael N. Creech C.B. Efficacy and Safety of the m RNA-1273 SARS-Co V-2 Vaccine N. Engl. J. Med.202038440341610.1056/NEJ Moa 203538933378609 PMC 7787219 · doi ↗ · pubmed ↗
- 8Falsey A.R. Sobieszczyk M.E. Hirsch I. Sproule S. Robb M.L. Corey L. Neuzil K.M. Hahn W. Hunt J. Mulligan M.J. Phase 3 Safety and Efficacy of AZD 1222 (Ch Ad Ox 1 n Co V-19) COVID-19 Vaccine N. Engl. J. Med.20213852348236010.1056/NEJ Moa 210529034587382 PMC 8522798 · doi ↗ · pubmed ↗