Oligodendroglioma of the Hippocampus: A Case Report and Systematic Review on Therapeutic Approaches of Oligodendroglioma After WHO 2021 Classification
Panagiotis Skouras, Georgios Giakoumettis, Charalampos Argyros, George Vavoulis, Emmanouil K. Verigos, Dimitrios Giakoumettis

TL;DR
This paper discusses how molecular diagnostics, like IDH mutations and 1p/19q co-deletion, are changing treatment for oligodendrogliomas, a type of brain tumor, by guiding personalized therapies.
Contribution
The study provides a systematic review of therapeutic approaches for oligodendrogliomas post-WHO 2021 classification and includes a case report illustrating molecular-guided treatment.
Findings
Maximal safe surgical resection combined with PCV chemotherapy and radiotherapy improves progression-free and overall survival.
Molecular profiling is critical for personalizing treatment strategies in oligodendroglioma patients.
A multidisciplinary approach incorporating molecular insights leads to favorable clinical outcomes.
Abstract
Background: Oligodendrogliomas are a molecularly distinct subtype of glioma according to the WHO 2021 tumor classification, defined as isocitrate dehydrogenase (IDH) mutations and 1p/19q co-deletion. This updated classification has changed the approach to glioma management by emphasizing the critical role of molecular diagnostics. This study explores current therapeutic strategies for adult oligodendrogliomas and contextualizes findings with a patient with a Grade 3 oligodendroglioma of the hippocampus. Methods: A systematic review was conducted, synthesizing evidence from 36 studies published between 2021 and 2024. The review focuses on surgical resection, PCV chemotherapy (procarbazine, lomustine, vincristine), and radiotherapy, with progression-free survival (PFS) and overall survival (OS) as primary outcomes. Moreover, a 45-year-old woman diagnosed with an IDH-mutant,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1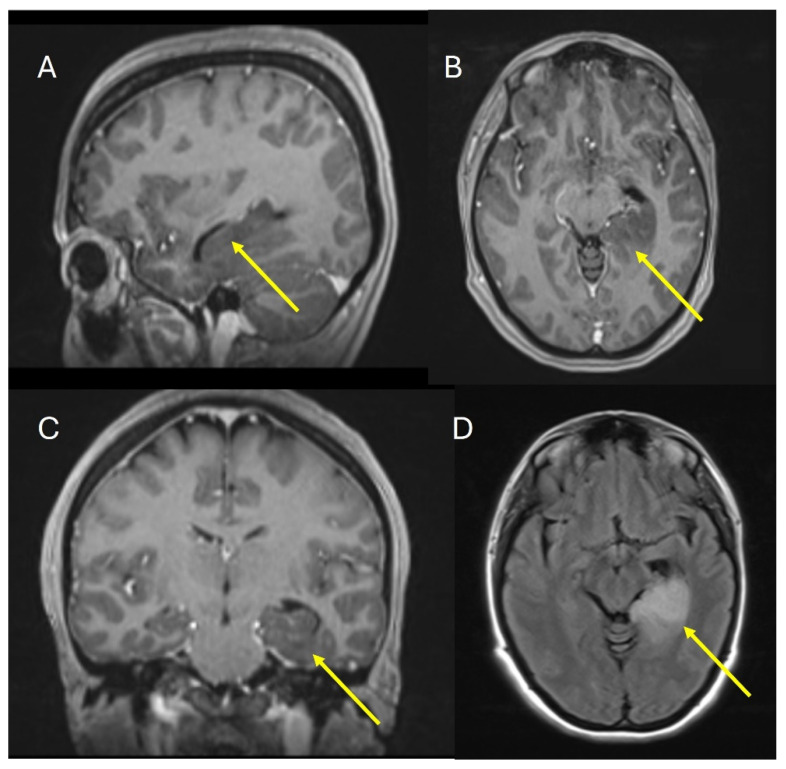 Figure 2
Figure 2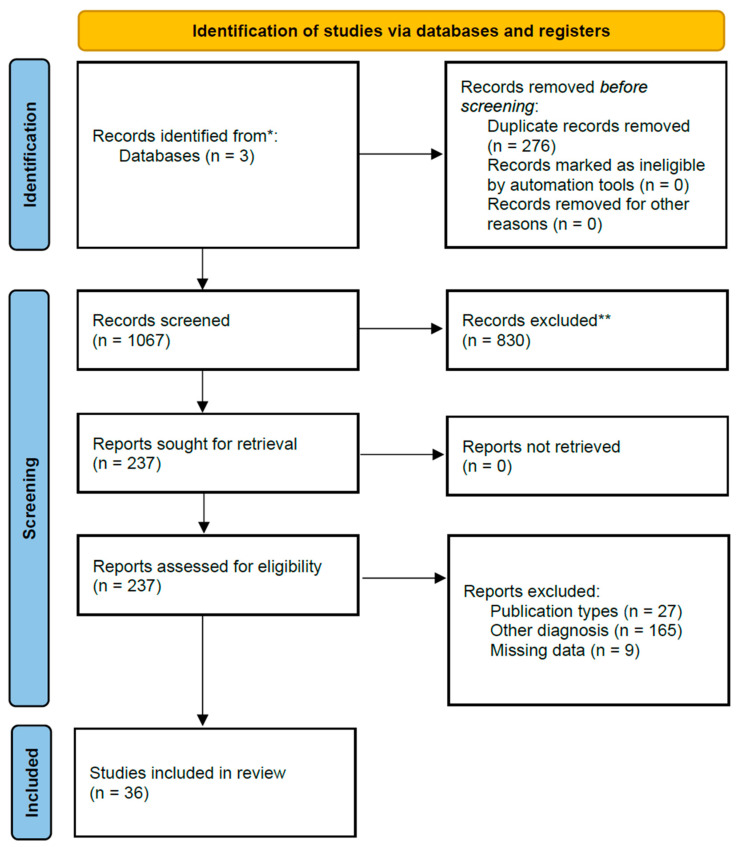 Figure 3
Figure 3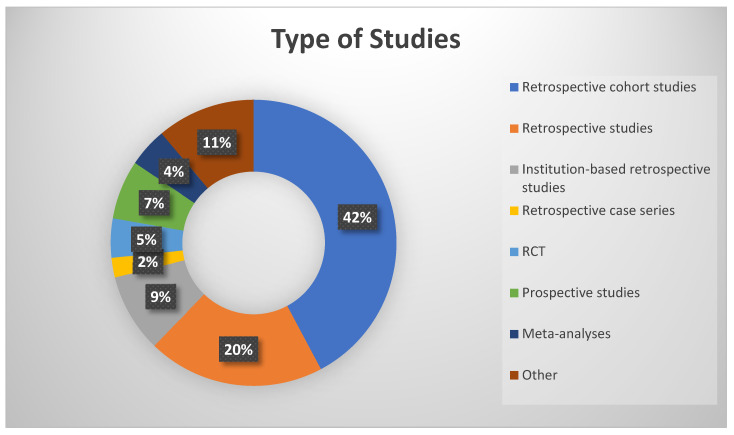 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Brain Metastases and Treatment · MicroRNA in disease regulation
1. Introduction
Gliomas, originating from neuroglial cells in the brain and spinal cord, account for over 80% of malignant central nervous system (CNS) tumors. The 2021 World Health Organization (WHO) classification incorporates advancements in molecular biology, categorizing gliomas into adult-type diffuse gliomas, pediatric-type diffuse low-grade and high-grade gliomas, circumscribed astrocytic gliomas, and ependymal tumors [1,2,3]. In the updated classification, oligodendrogliomas are defined by the presence of isocitrate dehydrogenase IDH1 or IDH2 mutations and 1p/19q co-deletion. Despite this molecular specificity, predicting outcomes remains challenging, as survival data from older histology-based studies and registries are confounded by the inclusion of 20–70% of patients lacking these molecular markers. Based on the latest report of the Central Brain Tumor Registry of the United States (CBTRUS) 2016–2020, the average annual age-adjusted incidence rate of IDH-mutant and 1p/19q-co-deleted oligodendroglioma is 0.29 (95% CI 0.28–0.30). The 5-year survival rate for all ages for patients with oligodendroglioma and anaplastic oligodendroglioma is 84.6% (95% CI 83.7–85.4) and 66.8 (95% CI 65.2–68.4), respectively [4]. Improved survival has been linked to extensive yet safe surgical resection and the use of procarbazine, CCNU (lomustine), and vincristine (PCV) chemotherapy in combination with partial brain radiotherapy [5]. The current study focuses on optimizing treatment strategies, including therapies targeting IDH mutations and refining cytotoxic regimens. In addition, we review current therapeutic approaches in adults based on the WHO 2021 classification of gliomas. Moreover, we report the case of a 45-year-old woman with an oligodendroglioma located in the left hippocampus.
2. Materials and Methods
2.1. Case Presentation
A 45-year-old female patient presented in the ED due to dysarthria, drooping of the mouth corner, and an epileptic episode that had occurred 4 h ago. She was a right-handed teacher with no significant medical history. She was evaluated by a neurologist who initially considered the possibility of an ischemic stroke in the differential diagnosis. A CT scan of the brain (Figure 1) was performed, which revealed a hypodense area in the left hippocampus. Subsequently, the patient was referred to the neurosurgical team. During the examination, the patient showed improvement in her dysarthria and did not present any other neurological deficits. There were no memory impairments and no focal neurological deficits. The patient was admitted for further investigation with an MRI of the brain. Signed informed consent was received from the patient and, since this is a retrospective reflection of the case, an Institutional Review Board Statement was not deemed necessary.
2.2. Systematic Review
The search strategy included three databases, Pubmed, Scopus and ClinicalTrials, where an advanced search was undertaken including the keywords “oligodendrogliomas” AND “therapy” for the period from June 2021 to July 2024. This period was chosen due to the publication of The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary on 29 June 2021. The 2021 WHO grading, introduced in the fifth edition published in August 2021, brought significant changes, advancing the role of molecular diagnostics in CNS tumor classification, particularly for oligodendrogliomas. As this is a systematic review of the literature, an Institutional Review Board Statement was not deemed necessary. PRISMA guidelines and the PICO framework were followed.
2.3. Review Structure and PICO Framework
The review is structured using the following PICO framework:
- Population (P): Adults (≥18 years) diagnosed with oligodendroglioma, as defined by the WHO 2021 classification (IDH-mutant, 1p/19q-co-deleted, Grade 2 or 3).
- Intervention (I): Treatments including surgery, chemotherapy, radiotherapy, or other therapeutic interventions.
- Comparison (C): No specific comparator.
- Outcome (O): Progression-free survival (PFS) and/or overall survival (OS).
This update will include studies that meet predefined inclusion and exclusion criteria.
2.4. Inclusion Criteria
Eligible studies must focus on adult patients (≥18 years) diagnosed with oligodendroglioma, as defined by the 2021 World Health Organization (WHO) classification, specifically IDH-mutant and 1p/19q-co-deleted Grade 2 or 3 gliomas. We will include original studies such as randomized clinical trials (RCTs), non-RCTs, observational studies, retrospective studies, meta-analyses, and case series involving more than three patients. Studies must be published in English, evaluate treatment modalities (e.g., surgery, chemotherapy, radiotherapy, or other therapies), and report outcomes related to progression-free survival (PFS) or overall survival (OS). Only studies published within the last three years, after the adoption of the WHO 2021 classification, will be considered.
2.5. Exclusion Criteria
We will exclude studies that do not meet the inclusion criteria, including reviews, systematic reviews, case reports, letters to the editor, animal studies, and gray literature. Studies focused on pediatric patients (<18 years), written in languages other than English, or addressing diagnoses other than oligodendroglioma based on the 2021 WHO molecular classification will also be excluded. Furthermore, studies that do not address treatment approaches for oligodendrogliomas will not be considered.
2.6. Data Extraction
Following the search and removal of duplicates, the research team will independently screen the titles and abstracts of the identified studies to determine their potential inclusion. The full texts of all potentially relevant studies will then be assessed against our inclusion criteria. Any disagreements between reviewers regarding a study’s eligibility will be resolved by consulting a sixth reviewer. Data will be extracted from the included studies using a standardized, piloted form. The extracted data will include study design, population details, the number of participants, comprehensive descriptions of the analytical techniques used, and study results.
3. Results
3.1. Case Results
The patient underwent an MRI of the brain with contrast, which revealed a lesion occupying the left hippocampal formation and the parahippocampal gyrus. The lesion was not contrast enhanced; it was hypo-intensive in T1WI and high-intensive in FLAIR and T2WI (Figure 2). The patient was offered and underwent a biopsy of the lesion.
The pathology report revealed an IDH-mutated (IDH1^R132H^) and 1p/19q co-deleted oligodendroglioma, Grade 3 (WHO grading 2021). The tumor was characterized by a moderate-to-sufficient number of cells with relative morphological uniformity. There was no evidence of vascular hyperplasia or necrosis. No H3.3 K27M mutation was found. Additionally, the neoplastic cells expressed the transcription factors Olig2, FOXG1, and GFAP. There was no expression of the mutated p53 protein, and the nuclear expression of ATRX was preserved. There was no expression of the FUBP1 protein and no overexpression of the EGFR protein. After the diagnosis and treatment options were discussed with the patient and her family, she decided to continue with oncological therapy, including chemotherapy and radiotherapy, receiving the typical Stupp protocol. At her 3-month follow-up, there were no clinical signs or symptoms from her tumor, and she had only mild chemotherapy-related side effects. This aligns with the review’s findings, indicating a favorable prognosis for IDH-mutant, 1p/19q co-deleted oligodendrogliomas when treated with multimodal therapy.
3.2. Systematic Review Results
We conducted a comprehensive search using three databases. The search in PubMed identified 409 studies, and in Scopus, 927 studies were found, all from the period between 2021 and 2024. Additionally, a focused search was performed on ClinicalTrials.gov, restricted to completed trials, and only studies with available results were considered within the timeframe for study completion 1 January 2021 to 20 July 2024. This approach ensured that only the most relevant and up-to-date clinical trials, focusing on treatment strategies for oligodendroglioma in adult populations, were included. The search in ClinicalTrials.gov yielded seven studies. The total number of articles identified across all databases was 1343. These articles were analyzed using Rayyan accessed on 20 July 2024 (https://new.rayyan.ai/), and 276 duplicates were removed. The remaining 1067 articles were screened based on their titles and abstracts. After applying the inclusion and exclusion criteria, 830 articles were excluded. The remaining 237 articles underwent full-text screening and, ultimately, 36 studies were included in the final analysis (Appendix A, Table A1) (Figure 3, PRISMA flow chart). The types of study included are shown in Figure 4. The total number of patients was 7134 with an IDH mutated and 1p/19q co-deleted oligodendroglioma. The majority of patients were between 35 and 65 years old, with a mean age of approximately 45.7 years and range from 19 to 83 years. The pooled mean overall survival (OS) and progression-free survival (PFS) were not possible to extract or extrapolate safely due to the fact that there was no uniform report on them. Several studies within the cohort highlighted that median OS values exceeded 100 months for certain patient subgroups and others reported on 1-, 3- and 5-year overall survival. Survival outcomes, particularly PFS and OS, were found to vary significantly based on molecular characteristics, such as IDH mutation status and 1p/19q co-deletion. However, a trend seems to exist on age, which, above 35 years, was associated with decreased OS in some studies, and treatment factors, including the extent of surgery, chemotherapy, and radiotherapy, which played a crucial role in influencing survival outcomes.
4. Discussion
Oligodendroglioma of the hippocampus is rare, and the literature is scarce in this region. Our patient was diagnosed with an IDH-mutant, 1p/19q-co-deleted Grade 3 oligodendroglioma, according to the WHO 2021 classification. This molecular signature is a key diagnostic and prognostic marker, commonly observed in reviewed cases. The tumor was located in the hippocampus, an uncommon site for oligodendrogliomas, which can complicate surgical resection and impact treatment strategies. However, the survival is still based on the molecular characteristics of the tumor, in addition to the extent of resection (EOR), and oncological therapies. This systematic review provides an analysis for oligodendrogliomas defined by the WHO 2021 CNS tumor classification. All of the 36 studies included in the analysis highlighted the important role of the molecular markers, IDH mutations and 1p/19q co-deletion, in predicting therapeutic response and survival outcomes. The therapeutic strategies presented included surgical resection with adjuvant chemotherapy, and radiotherapy as the cornerstone of treatment. Nevertheless, chemotherapy and radiotherapy without surgical excision may also be a therapeutic choice, with temozolomide and PCV regimens as standard chemotherapy options. In our case, a biopsy was performed, followed by chemotherapy and radiotherapy. While PCV (procarbazine, lomustine, vincristine) is a standard regimen, the patient received temozolomide (TMZ), a well-tolerated alternative commonly used in recent studies. Moreover, adjuvant therapies, particularly the combination of radiotherapy and chemotherapy, have also demonstrated significant survival benefits, with better outcomes in high-grade tumors. Even though all studies agree on the importance of molecular markers, there are significant variations in treatment protocols as well as patient outcomes. This stresses the need for a standardized approach and report. There is no doubt that molecular markers play and will continue to play a pivotal role in the diagnosis, prognosis, and treatment of oligodendrogliomas [7,8,9], as depicted in all studies. In addition, elevated FXYD2 mRNA expression and MGMT (O6-Methylguanine-DNA Methyltransferase) promoter methylation were highlighted in several studies as improving survival outcomes [10,11]. In general, median OS has been shown to be better for patients with IDH-mutant and 1p/19q co-deleted tumors, exceeding 14 years in some cohorts [12]. Nevertheless, several factors such as age, tumor size, incomplete resection, or certain genetic mutations have been blamed for negatively influencing survival [5,13], e.g., a mutation on PIK3CA along with intratumoral calcifications was linked to worse prognosis [14,15]. The emerging use of DNA methylation profiling and gene signatures demonstrated their potential to stratify patients and predict treatment responses [8,16]. In terms of surgical operation, the extent of resection and, more specifically, gross total resection or subtotal resection, has been strongly associated with overall survival and progression-free survival [8,9,12,17]. In a retrospective study by Hervey-Jumper et al., 190 patients (48.5%) had an IDH-mutant and 1p/19q-co-deleted oligodendroglioma. The median age of this group was 42.6 years, with a range between 34.4 and 49.5 years. Tumor locations included the frontal lobe in 116 patients (61%), the temporal lobe in 21 patients (11.1%), the parietal lobe in 25 patients (13.2%), the insular lobe in 27 patients (14.2%), and other locations in 1 patient (0.5%). In terms of treatment, all patients received a surgical operation, 88 patients (47.1%) received chemotherapy (out of which, 76 patients received TMZ), and 72 patients (37.9%) received radiotherapy. Achieving an EOR of at least 75% for OS and 80% for PFS is particularly beneficial. Outcomes showed a median progression-free survival (PFS) of 11.69 years, with a range between 9.29 and 17.70 years [7]. Chemotherapy and radiotherapy are another therapeutic choice for patients. The combination of them, particularly using PCV (procarbazine, lomustine, vincristine) or temozolomide (TMZ), has shown better results in PFS and OS in comparison to monotherapy, as shown in the clinical trial CODEL and the randomized controlled trial by Bush et al. [18,19]. The choice between these modalities may, however, depend on tumor grade, e.g., Grade 2 tumors with favorable features could be tackled with chemotherapy alone to reduce long-term toxicities [19,20]. Adjuvant radiotherapy has been shown in the meta-analysis by Koh to improve OS and PFS in Grade 3 tumors, whereas proton radiotherapy, though effective, has been associated with several risks such as radiation-induced contrast enhancements (RICE), particularly in lower-grade tumors [21]. Radiotherapy alone has not been proven to improve OS and PFS in comparison to its combination with other treatment modalities [18]. Finally, emerging therapies have offered hope for better therapies. Mutant IDH inhibitors induce differentiation into astrocytic-like states, while NOTCH1 mutations may serve as biomarkers for response stratification. Recent studies suggest that mutant IDH inhibitors promote differentiation of oligodendroglioma cells into astrocytic-like states, reducing tumor proliferation [22]. Unlike conventional chemotherapy, which induces direct cytotoxicity, IDH inhibitors work by modifying tumor metabolism. Early clinical trials have shown disease stabilization in IDH-mutant gliomas, but long-term survival benefits remain uncertain, as most trials are still in Phase I/II. Meanwhile, other studies have offered insight into the use of advanced imaging techniques, such as FET-PET (Fluoroethyltyrosine Positron Emission Tomography), for assessing treatment response and guiding clinical decisions [23]. Targeted therapy has also been shown to be a promising future option. The retrospective study by Jun et al. on recurrent high-grade gliomas treated with anlotinib included 29 patients with a median age of 50 years, ranging from 15 to 71 years. Of these, 93.1% had undergone surgery prior to the study. Tumor characteristics revealed that 48.3% of cases were multifocal or disseminated, while 51.7% were focal. The molecular characteristics of the patients included in the study indicated that 79.3% were IDH wild type, while only 20.7% had an IDH mutation. A methylated MGMT promoter status was reported in 41.4% and unmethylated in 58.6% of patients. Anlotinib is a multi-targeted tyrosine kinase inhibitor (TKI) that was administered as monotherapy or in combination with other therapies, including temozolomide, semustine, irinotecan, and vemurafenib. All patients had received radiotherapy with concurrent chemotherapy during their initial treatment after diagnosis of high-grade glioma, and previous therapies included bevacizumab and nimotuzumab in some patients. The outcomes showed a median progression-free survival (PFS) of 9.4 months (95% CI: 6.5–12.3), with a 6-month PFS rate of 62.1%. Median overall survival (OS) was 12.7 months (95% CI: 9.7–15.7), with a 6-month OS rate of 79.3% and a 1-year OS rate of 48.3%. The key findings of this study suggest that anlotinib, a multi-target anti-angiogenic agent, demonstrated potential efficacy as both monotherapy and in combination therapy for the treatment of recurrent high-grade gliomas [24]. Moreover, other studies investigate the use of neoadjuvant and adjuvant immunotherapy in patients with a second or third recurrence of histologically confirmed IDH1R132H-positive, 1p/19q-co-deleted oligodendrogliomas (CNS WHO Grade 2 or 3). This immunotherapy approach aims to harness IDH1 mutation-specific vaccination combined with checkpoint inhibition to improve patient outcomes. Checkpoint inhibitors targeting PD-1/PD-L1 and IDH1-specific vaccines have shown potential in preclinical models of IDH-mutant gliomas (Table 1) [25].
However, unlike in other cancers, immunotherapy has shown mixed results in gliomas due to their highly immunosuppressive microenvironment. Combining checkpoint inhibitors with radiotherapy or chemotherapy may enhance response rates, but more clinical data is needed before replacing conventional therapies. Two large meta-analyses with many patients have also been included in our study. Xuan et al. present a systematic review and meta-analysis that examines the outcomes of treatments in IDH-mutated and 1p/19q co-deleted oligodendrogliomas. The review included data from 17 studies with a total of 11,949 participants, out of which 1646 patients had IDH-mutated and 1p/19q co-deleted oligodendrogliomas. The tumor samples were mostly obtained after gross total resection (GTR) and subtotal resection (STR), and from biopsies in some cases. The treatments and interventions analyzed in the review primarily involved chemotherapy, with PCV (procarbazine, lomustine, vincristine) or temozolomide (TMZ) being the most commonly used agents. The latter was favored in more recent studies due to its better tolerability. Standard protocols were followed for both regimens. Where RT was combined with chemotherapy either concurrently or sequentially, better outcomes were seen compared to monotherapy. Additional RT or chemotherapy were used for patients who experienced disease progression, as salvage therapy. The outcomes of the review showed that adjuvant RT improved PFS by 50% (hazard ratio [HR] 0.52; confidence interval [CI]: 0.40–0.66), where both Grade 2 and Grade 3 oligodendroglioma patients benefited from this improvement. Adjuvant RT also improved OS by 28% (HR 0.72; CI: 0.56–0.93), with a more pronounced benefit in Grade 3 oligodendroglioma patients compared to Grade 2 [26]. The second meta-analysis by Zhang et al., involved 1944 patients with newly diagnosed gliomas, including 169 patients with oligodendrogliomas. The median age range of the cohort was between 54.2 and 59 years, although some studies included younger patients, with age ranges starting as low as 20.5 years. The study did not provide specific details on the extent of surgical resection or tumor locations. Chemoradiotherapy included temozolomide (TMZ) and conventional External Beam Radiotherapy (EBRT) following the established Stupp protocol [27]. Hypofractionation was used in some cases. The study also highlighted the frequent use of glucocorticoids to manage edema, though doses exceeding 2 mg/day were associated with worsened lymphopenia. Outcomes showed that severe lymphopenia significantly worsened overall survival (OS), with a hazard ratio of 1.99 (95% CI: 1.74–2.27). OS was also influenced by radiation dose and chemotherapy regimens. However, molecular characteristics such as 1p/19q co-deletion and MGMT promoter methylation were not consistently reported across studies. This meta-analysis underscored the importance of lymphopenia in predicting OS outcomes in glioma patients, though more molecular data would be valuable for a clearer understanding of prognostic factors [28].
5. Limitations
This review is subject to certain limitations. First, the predominance of retrospective studies limits the ability to draw definitive causal inferences. Second, the heterogeneity in treatment protocols and patient populations across studies complicates direct comparisons. In addition, there is no uniform way of presenting the outcomes; where several studies report either median or year OS and PFS, others do not. Moreover, only a few studies included long-term follow-up, particularly in emerging therapies, leaving uncertainties about their sustained efficacy and safety. Even though it was not in the scope of this systematic review, a pooled analysis was not possible to carry out safely due to the diversity of the reported outcomes.
6. Conclusions
Advancements in molecular diagnostics have profoundly shaped the management of oligodendrogliomas, reinforcing the necessity of a personalized, multidisciplinary approach. Maximal safe surgical resection should be the primary goal, as it significantly improves progression-free survival (PFS) and overall survival (OS). In cases where complete resection is not achievable, subtotal resection followed by adjuvant therapy remains a viable option. Patients with IDH-mutant, 1p/19q-co-deleted oligodendrogliomas should be considered for adjuvant chemotherapy and/or radiotherapy based on tumor grade and patient-specific factors. Given the prognostic and predictive significance of IDH mutations and 1p/19q co-deletion, molecular profiling should be integrated into routine clinical practice. Additional markers, such as MGMT promoter methylation and PIK3CA mutations, may further refine treatment strategies. Regular MRI monitoring is essential for the early detection of recurrence or progression. Personalized follow-up intervals should be based on initial treatment response and molecular risk stratification. IDH inhibitors and immunotherapy hold promise as adjuncts or alternatives in refractory or recurrent cases. Clinicians should consider enrolling eligible patients in clinical trials evaluating these novel therapies to expand treatment options. By integrating molecular insights into clinical decision-making, adopting a patient-centered approach, and considering novel therapies when appropriate, clinicians can optimize outcomes and quality of life for patients with oligodendrogliomas. Future prospective or retrospective studies about oligodendroglioma patients focusing on standardizing treatment protocols and reporting results in a uniform way—including percentage of resection, overall survival rate, and progression-free survival rate—would be the next logical thing to do.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu H. Zhang L. Tan Y. Jiang Y. Lu H. Observation of the delineation of the target volume of radiotherapy in adult-type diffuse gliomas after temozolomide-based chemoradiotherapy: Analysis of recurrence patterns and predictive factors Radiat. Oncol.2023181610.1186/s 13014-023-02203-w 36691100 PMC 9872393 · doi ↗ · pubmed ↗
- 2Louis D.N. Perry A. Wesseling P. Brat D.J. Cree I.A. Figarella-Branger D. Hawkins C. Ng H.K. Pfister S.M. Reifenberger G. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary Neuro Oncol.2021231231125110.1093/neuonc/noab 10634185076 PMC 8328013 · doi ↗ · pubmed ↗
- 3Torp S.H. Solheim O. Skjulsvik A.J. The WHO 2021 Classification of Central Nervous System tumours: A practical update on what neurosurgeons need to know-a minireview Acta Neurochir.20221642453246410.1007/s 00701-022-05301-y 35879477 PMC 9427889 · doi ↗ · pubmed ↗
- 4Ostrom Q.T. Price M. Neff C. Cioffi G. Waite K.A. Kruchko C. Barnholtz-Sloan J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2016–2020 Neuro Oncol.202325 iv 1iv 9910.1093/neuonc/noad 14937793125 PMC 10550277 · doi ↗ · pubmed ↗
- 5Wick A. Sander A. Koch M. Bendszus M. Combs S. Haut T. Dormann A. Walter S. Pertz M. Merkle-Lock J. Improvement of functional outcome for patients with newly diagnosed grade 2 or 3 gliomas with co-deletion of 1p/19q—IMPROVE CODEL: The NOA-18 trial BMC Cancer 20222264510.1186/s 12885-022-09720-z 35692047 PMC 9190129 · doi ↗ · pubmed ↗
- 6Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ 2021372 n 7110.1136/bmj.n 7133782057 PMC 8005924 · doi ↗ · pubmed ↗
- 7Hervey-Jumper S.L. Zhang Y. Phillips J.J. Morshed R.A. Young J.S. Mc Coy L. Lafontaine M. Luks T. Ammanuel S. Kakaizada S. Interactive Effects of Molecular, Therapeutic, and Patient Factors on Outcome of Diffuse Low-Grade Glioma J. Clin. Oncol.2023412029204210.1200/JCO.21.0292936599113 PMC 10082290 · doi ↗ · pubmed ↗
- 8Mair M.J. Leibetseder A. Heller G. Puhr R. Tomasich E. Goldberger S. Hatziioannou T. Wohrer A. Widhalm G. Dieckmann K. Early Postoperative Treatment versus Initial Observation in CNS WHO Grade 2 and 3 Oligodendroglioma: Clinical Outcomes and DNA Methylation Patterns Clin. Cancer Res.2022284565457310.1158/1078-0432.CCR-22-113335998208 · doi ↗ · pubmed ↗