Post-Transplant Cyclophosphamide-Based GVHD Prophylaxis After Peripheral Blood Stem Cell HLA Identical Transplantation in Patients with Lymphoma: A Prospective Observational Study
Stefania Bramanti, Daniela Taurino, Filippo Magri, Chiara De Philippis, Barbara Sarina, Luca Castagna, Laura Giordano, Jacopo Mariotti, Daniele Mannina, Armando Santoro

TL;DR
This study shows that using post-transplant cyclophosphamide to prevent graft-versus-host disease in lymphoma patients after stem cell transplants is effective and safe.
Contribution
The study provides prospective evidence that post-transplant cyclophosphamide is a viable GVHD prophylaxis in HLA-identical donor transplants for lymphoma.
Findings
3-year GVHD-relapse-free survival was 70.4%.
Only 7.4% of patients experienced non-relapse mortality within one year.
Low rates of acute and chronic GVHD were observed with no grade IV events.
Abstract
Allogeneic stem cell transplantation (allo-SCT) from HLA-identical donors (HLAid) could be an effective salvage treatment for relapsed/refractory lymphoma. In this setting, standard graft-versus-host disease (GVHD) prophylaxis is based on cyclosporine and methotrexate, with the addition of anti-thymocyte globulin, at least for matched, unrelated donors. Promising data using post-transplant cyclophosphamide (PT-Cy) have been reported from retrospective studies in patients receiving allo-SCT from HLAid donors. Here, we report the results of a single-center, prospective observational study exploring the main outcomes of GVHD prophylaxis based on PT-Cy in 27 patients receiving HLAid donor transplantation for relapsed/refractory lymphoma. With a median follow-up of 38 months, 3-year GVHD-relapse-free survival and PFS and OS were 70.4%, 81.5%, and 88.9%, respectively. The 1-year cumulative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
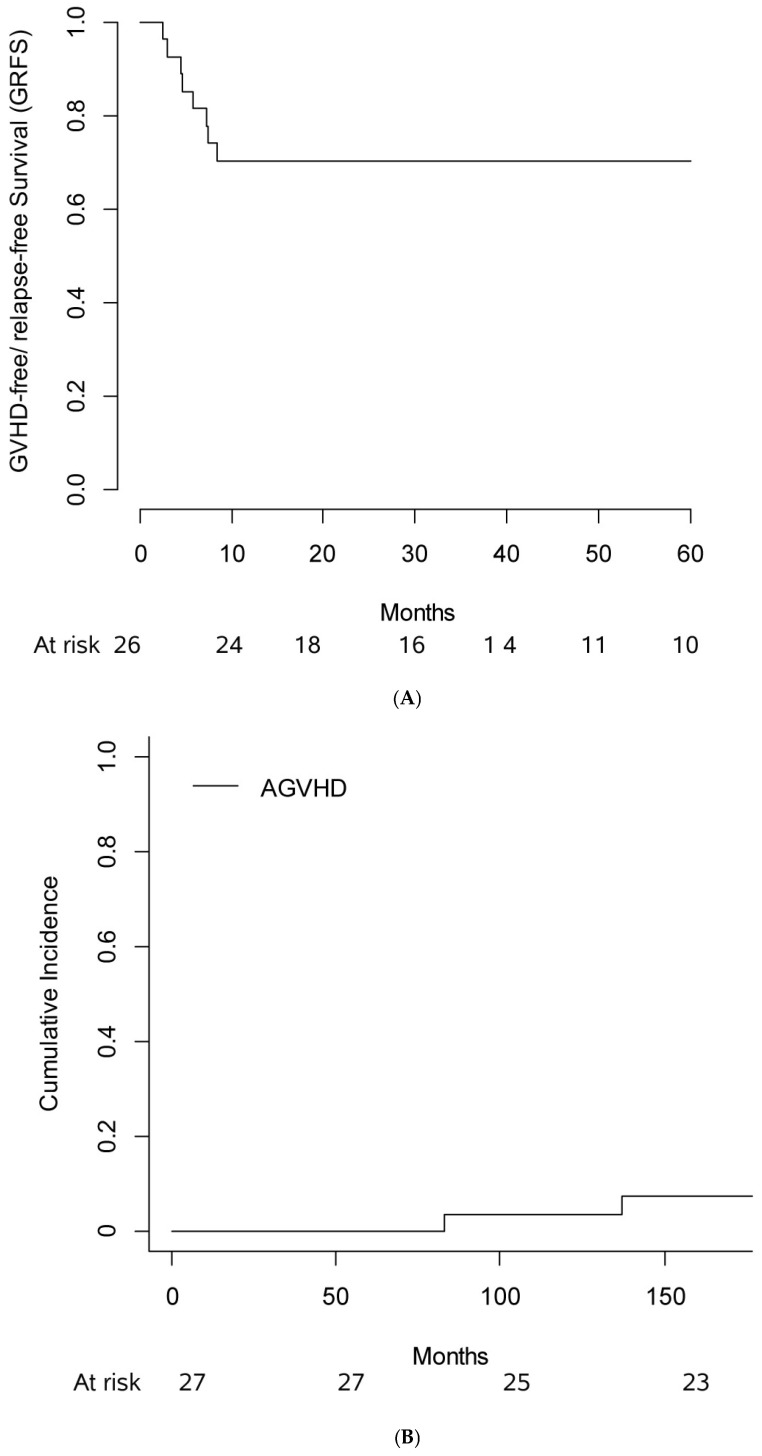 Figure 1
Figure 1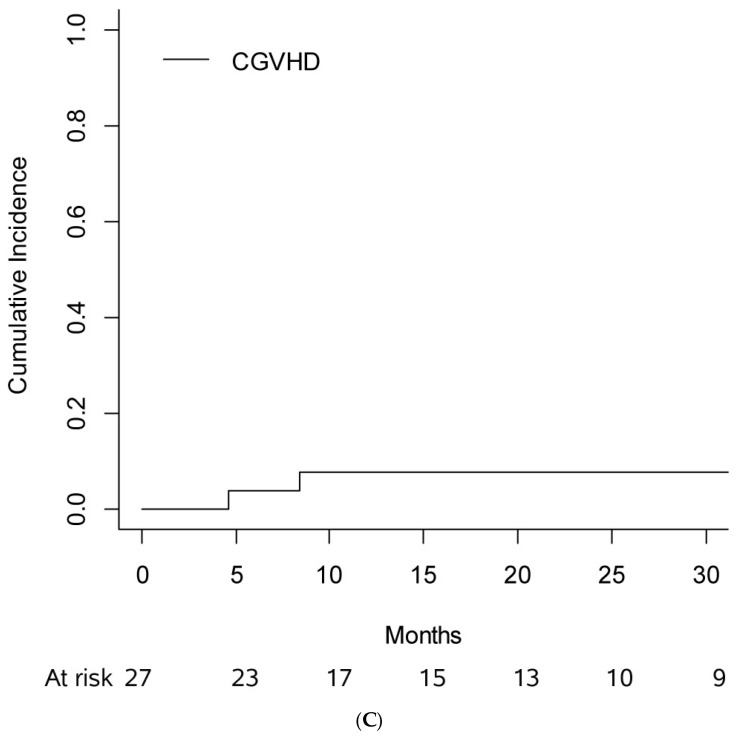 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Polyomavirus and related diseases · Viral-associated cancers and disorders
1. Introduction
Before the introduction of CAR-T therapy, allogeneic stem cell transplantation (allo-SCT) was the only strategy capable of achieving long-term survival in patients with relapsed or refractory lymphoma after more than two lines of chemotherapy and/or autologous transplantation and poor prognosis. HLA identical donor (HLAid), sibling or unrelated (UD) peripheral blood stem cells (PBSCs), is considered the most suitable donor source [1]. With the introduction of CAR-T-cell therapy for treating relapsed/refractory lymphoma, the clinical course of these patients has undergone further changes. The role of allo-SCT in patients relapsed or refractory to CAR-T-cell therapy remains controversial. However, it may represent these patients’ only potential curative option, offering a promising therapeutic avenue in the context of otherwise limited treatment options [2,3]. The only recently published prospective trial on allo-HCT for relapsed/refractory aggressive non-Hodgkin lymphoma is DSHNHL 2004-R3 (NCT00785330) [4], which enrolled 84 patients. With 55% of the patients being chemorefractory at allo-HCT, PFS and OS were 45% and 52% at 1 year and 39% and 42% at 3 years post-transplant. One-year relapse/progression incidence was 29%, with no relapse event occurring thereafter.
In this setting, prophylaxis for graft-versus-host disease (GVHD) was historically based on cyclosporine (CSA) and methotrexate (MTX), with anti-thymocyte globulin (ATG) in UD donors. With this approach, the expected cumulative incidence (CI) of acute GVHD (aGVHD) grade II-IV was 35%, and extensive chronic GVHD (cGVHD) was 25% [5]. In the haploidentical donor transplant setting, T-cell replete grafts with post-transplant cyclophosphamide (PT-Cy) have become the standard GVHD prophylaxis for patients with hematological malignancies [6,7,8]. Several studies have evaluated the use of PT-Cy as GVHD prophylaxis in patients who underwent HLA-matched transplantation in leukemia patients [9,10,11,12,13,14,15,16,17,18,19]. Collectively, these studies showed a lower incidence of acute and chronic GVHD compared with standard calcineurin inhibitors (CNI)-based GVHD prophylaxis with or without ATG in the HLA-matched–related or –unrelated allo-SCT [13,14]. However, information on the application of this approach in patients with lymphoid disease is scant, and more data are needed to assess the role of PT-Cy as GVHD prophylaxis in this patient population.
Here, we present a single-center prospective observational study to evaluate GVHD-relapse-free survival (GRFS) using a GVHD prophylaxis based on the combination of PT-Cy, CSA, and mycophenolic acid (MPA) according to the Baltimora-modified platform [8] in patients diagnosed with relapsed/refractory (R/R) lymphoma who underwent allo-SCT from HLAid donors, both familiar and unrelated, after a reduced-intensity (RIC)/non-myeloablative (NMA) conditioning regimen.
2. Materials and Methods
2.1. Setting and Design
This single-arm, double-stage, open-label, prospective observational study was conducted from March 2018 to November 2021 and evaluated the patients diagnosed with R/R lymphoma receiving PBSC HLAid transplantation conditioning with RIC/NMA regimen and GVHD prophylaxis with PT-Cy, CSA, and MPA.
The institutional review board of the IRCCS Humanitas Research Hospital approved the study. Patients provided informed consent for the collection of their clinical data. All procedures were performed by the Ethical Standards of the Responsible Committee on Human Experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
2.2. Patients
All patients had a histologically confirmed lymphoma diagnosis in complete remission (CR) or partial remission (PR) after the last chemotherapy line. Therefore, the indications for allo-SCT were primary refractory lymphomas, relapse after autologous transplantation, or PBSC mobilization failure.
Other inclusion criteria were as follows: 18–70 years of age; heart ventricular ejection fraction > 40%; DLCO and FEV1 > 50% predicted; total bilirubin ≤ 2.5 mg/dL; ALT, AST, and alkaline phosphatase < 5 × upper limit of normal (ULN); creatinine clearance or GFR by Cockroft–Gault formula > 50 mL/min/1.73 m^2^; Karnofsky performance score ≤ 60%.
Exclusion criteria were haploidentical or mismatched unrelated donor (MMUD) transplantations and any medical condition contraindicating allo-SCT.
2.3. Endpoints
The study’s primary endpoint was the proportion of patients without GRFS at one year. The secondary endpoints were incidence of engraftment, chimerism, aGVHD grade II-IV and III-IV, cGVHD, NRM, relapse, progression-free survival (PFS: defined as the time from enrollment to progression of disease, death, or loss to follow-up; whatever occurred first), overall survival (OS: defined as the time from enrollment to death or loss to follow-up; whatever occurred first), and incidence of infection.
2.4. Conditioning Regimen and GVHD Prophylaxis
The choice of conditioning regimens followed local guidelines and took into consideration the patient’s age, the hematopoietic cell transplantation-comorbidity index [20], disease risk index (DRI) [21], and disease status at transplant. Three main conditioning regimens were used: (a) NMA regimen (Cy 14.5 mg/kg on days −6 and −5, fludarabine 30 mg/m^2^ from day −6 to day −2, and low-dose total body irradiation (TBI) (2 Gy) on day −1); (b) RIC regimen (either thiotepa 5 mg/kg on day −7, busulfan 65 mg/m^2^ on day −6 and day −3, and fludarabine 40 mg/mq from day −6 to day −3; since 2019 the patients received busulfan target AUC = 16.000 μmolar × minutes [22,23,24]); and (c) RIC regimen (thiotepa 6 mg/kg BID on day −5, cyclophosphamide 30 mg/kg from day −4 to day −3, and fludarabine 30 mg/m^2^ from day −4 to day −3).
The GVHD prophylaxis regimen consisted of PT-Cy 50 mg/kg intravenous (IV) administered on days +3 and +4, CSA 3 mg/kg from day +5 to day +100, and MPA 45 mg/kg divided into three doses administered orally from day +5 to day +35. CSA dose was progressively reduced from day +100 to day +180.
Subcutaneous granulocyte colony-stimulating factor (G-CSF) was used from day +5 at 5 μg/kg/day. Prophylaxis against bacterial, viral, and fungal agents was administered according to local guidelines [25]. In addition, monitoring for CMV and EBV reactivation by PCR was performed twice a week during the early period (+15 to day +100) and then weekly until day +180. Letermovir was approved in Italy in 2018. However, according to the AIFA restrictions, only 26% of the patients in the study performed prophylaxis with letermovir based on donor/recipient CMV status.
2.5. Stem Cell Source and Donors
Family members who were potential donors were HLA typed at the HLA-A, HLA-B, HLA-DRB1, and HLA-DQB1 loci at a high-resolution level. In addition, selected donors were typed at the HLA-C locus at a high-resolution level. The selection of donors in case of multiple-choice availability was based on weight, age, blood group, and CMV serology matches.
Donors underwent BM harvest under general anesthesia or were mobilized by subcutaneous G-CSF at 10 mg/kg/day for 5–6 days. In addition, unmanipulated bone marrow (BM) and PBSC were infused on day 0.
2.6. Engraftment Definition, GVHD, and Treatment Response Evaluation
White blood count recovery was defined as the first three consecutive days with an absolute neutrophil count of 0.5 × 10^9^/L since G-CSF was interrupted. Platelet recovery was defined as a count of 20 × 10^9^/L, with no transfusions required during the preceding seven days. Graft failure is defined as the lack of hematopoietic cell engraftment following allo-SCT. The MAGIC criteria [26] were used to grade aGVHD, and the NIH criteria [27] were used to grade cGVHD. Disease assessment was performed with a PET scan before the transplant for all patients [28,29]. In addition, pre-transplant CR patients were evaluated with a CT scan at 100 days’ post-transplant and subsequently every three months up to 1 year. Those in PR with PET scan at 100 days’ post-transplant and then with CT scan at the same time points. Chimerism was evaluated on peripheral blood 30 days after transplantation. In cases of male/female gender mismatch, the chimerism is evaluated by karyotype analysis and, in the absence of mismatch, by studying short tandem repeats by multiplex-PCR [30].
2.7. Statistical Analysis
The data were collected within a prospective clinical trial in which the sample size was not reached. Here, we present analyses of the primary outcome for exploratory purposes. Data were summarized as frequencies and proportions for categorical variables and median and range for continuous variables. Kaplan–Meier method was used to estimate survival and to depict corresponding curves. CI was used to estimate aGVHD, cGVHD, and NRM. In the data analysis, given the small sample size and number of events, the restricted mean survival time (RMST) was calculated for GRFS, with bootstrap resampling performed for estimation. All analyses have been performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
3. Results
3.1. Patients, Transplant, and Donor Characteristics
From March 2018 to 27 November 2021 patients were enrolled; the main patients, donors, and transplant characteristics are shown in Table 1.
One-third of patients (n = 9; 33%) were affected by Hodgkin lymphoma (HL), and two-thirds (18; 67%) by non-Hodgkin lymphoma (NHL).
Most patients were candidates for allo-SCT because they were primary refractory (n = 12, 45%) or relapsed after autologous transplantation (n = 10, 37%). Patients underwent a median of four lines of prior chemotherapy, and only one patient underwent an allogeneic transplant as consolidation following first-line therapy for T-prolymphocytic leukemia, achieving complete remission after alemtuzumab treatment. All patients with HL were previously exposed to checkpoint inhibitors and brentuximab vedotin. Among patients with DLBCL, only one underwent transplantation in relapse post-CAR T-cell therapy, while three did so after treatment with glofitamab. The majority of patients with mantle cell lymphoma were chemotherapy-refractory and achieved complete response after ibrutinib.
Most patients were in CR (n = 22, 81%). PBSC was the transplantation source for all but one patient, and the conditioning regimen was TBF for 78% of the patients (n = 21); 67% (n = 18) of HLA-matched donors were siblings.
3.2. GVHD-Relapse-Free Survival, PFS, OS
With a median follow-up of 37 months (IQ range: 25; 52), the 3-year PFS was 81.5% (CI 95%: 61.1; 91.8%), the 3-year GRFS was 70.4% (CI 95%: 49.4; 84%, Figure 1A), and the 3-year OS was 88.9% (CI 95%: 69.4; 96.2%). GRFS, RMST at 2 years was 18.5 months (CI 95%: 14.9; 21.4%).
3.3. Hematopoietic Recovery
No graft failures were observed. At 100 days, all but one patient had complete chimerism. The patient with mixed chimerism achieved complete chimerism at subsequent follow-up after cyclosporine discontinuation.
The median time for neutrophil and platelet recovery was 21 days (IQ range: 19; 21) and 23 days (IQ range: 17; 28), respectively.
3.4. GVHD
The 6-month CI of aGVHD grade II-IV was 7.4% (CI 95%: 0; 17.5%) (Figure 1B). In particular, one patient had grade II aGVHD (skin stage III, upper gastrointestinal stage I) and one grade III aGVHD (liver stage III); no grade IV aGVHD was observed. The 1-year CI of severe cGVHD was 7.7% (CI 95%: 0, 18.1%) (Figure 1C), with two patients experiencing moderate cGVHD. No patient died of GVHD.
3.5. NRM, RELAPSE
The 1-year CI of NRM was 7.4% (CI 95%: 0; 17.5%); two patients died of encephalitis, one from Escherichia coli and the other from an unknown cause. Only two patients experienced disease relapse at 77- and 220 days post-transplant, respectively. Overall, the 1-year cumulative incidence of relapse was 11.1% (CI 95%: 0; 23.2%), with two patients dying of progressive disease and the other presently in CR following CAR-T-cell therapy.
3.6. Infections
About 89% (CI 95%: 71; 97.6%, n = 24) of patients experienced an infectious event during the follow-up period. The most frequent symptoms were febrile neutropenia, pneumonia, CMV reactivations, BK cystitis, and sepsis. In more detail, ten patients (37%, CI 95%: 19; 58%) reported a bacterial infection, seven (26%, CI 95%: 11; 46%) had a viral infection, and four (15%, CI 95%: 0; 34%) showed a fungal infection.
Only one patient died of an infective complication (E. coli encephalitis at 160 days’ post-transplantation).
CMV reactivation was documented in seven patients (26%, CI 95%: 11; 46%) at a median time of 32 days’ post-transplantation. Only two patients developed a CMV infection, specifically gastritis and pneumonia, 36 and 35 days after the transplant, respectively. Furthermore, three patients (11%, CI 95%: 0; 29%) developed HHV-6 gastritis at a median time of 58 days’ post-transplant. BK virus cystitis was documented in three patients (11%, CI 95%: 0; 29%) at a median time of 41 days’ post-transplantation, with no grade ≥ III.
4. Discussion
Severe GVHD is a major cause of NRM and significantly impairs quality of life (QoL) after allo-SCT; therefore, improving GVHD prophylaxis strategies is crucial to reducing mortality and morbidity in these patients. The mechanisms of action of PT-Cy in preventing GVHD after haploidentical T-replete stem cell transplantation remain to be fully defined. However, alloreactive T-cell [31] elimination and regulatory T-cell preservation [32] could partially explain the GVHD prevention after PT-Cy. Different studies have explored PT-Cy-based GVHD prophylaxis regimens in patients receiving allo-SCT from HLAid donors, but mainly in patients with leukemia [9,10,11,12,13,14,15,16,17,18,19] (Table 2). Information on PT-Cy-based GVHD in patients with lymphoma is scant.
This monocentric prospective study focused on the use of PT-Cy-, MPA-, and CSA-based regimens as a GVHD-preventing strategy for patients with lymphoma who underwent an HLAid (both familiar and unrelated) PBSC transplantation with a previous RIC or NMA conditioning. The primary endpoint was achieved, showing a remarkable GRFS rate of 70.4% at three years. Considering the dismal prognosis of a heavily pretreated lymphoma population, the PT-Cy-based prophylaxis regimen after HLAid stem cell transplantation effectively reduced GVHD without losing disease control. With this strategy, few GVHD cases required treatment: only two cases (7.4%) of aGVHD, one grade II and one grade III, and all were responsive to first-line steroids without any further complication. Similarly, only two patients (7.7%) experienced moderate cGVHD and required treatment. These findings translate into a satisfying rate of NRM (7.4%). Despite the very high-risk lymphoma population, the incidence of relapse was low. Among the two patients who relapsed, only one died of progressive disease, and the second is still alive thanks to CAR T-cell therapy rescue. As expected, a longer median time (21 days) to engraftment of neutrophils was observed, probably due to MPA, comparable with a haploidentical transplant, but this did not translate into an increase in infectious events and toxic deaths. It should be noted that only 26% of patients enrolled in our study had undergone letermovir prophylaxis. Therefore, increased use of letermovir [33] over the years will likely further reduce CMV reactivations and infections.
Compared to the study by Broers et al. [34], with all the limits of cross-study comparisons, the main difference in acute and chronic GVHD seems to be using a three-drug prophylaxis regimen in our cohort, superimposable to the haploidentical one used by the Baltimore group [35]. Furthermore, the results of this study are comparable to those recently published in a retrospective series of the European Society for Blood and Marrow Transplantation (EBMT) and the Center for International Blood and Marrow Transplant Research (CIBMTR) [36]. In this retrospective study, matched unrelated donors with PT-Cy were associated with prolonged OS compared with the haploidentical donor, thanks to lower NRM and GVHD incidences. Currently, the patient population with lymphoma has changed, as the majority of patients with lymphoma undergoing allo-SCT are those who have relapsed or are refractory to CAR-T-cell therapy. Therefore, this transplant approach could be applied to this category of patients, given the excellent results achieved in terms of disease relapse and toxicity.
This study has several limitations that must be considered when interpreting the results. Firstly, the relatively small sample size. Second, the short follow-up period limits our ability to assess long-term outcomes and the duration of observed effects. Finally, the absence of a control arm in a single-center study design introduces a potential bias so that more studies would be needed for a more complete evaluation of the efficacy and safety of our approach.
Overall, this study shows that the use of the original Baltimore approach based on three drugs (PT-Cy, CSA, and MPA) could be as effective and safe as the standard approach in the prevention of acute and chronic GVHD also in patients with lymphoma who underwent HLAid PBSC transplantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Snowden J.A. Sánchez-Ortega I. Corbacioglu S. Basak G.W. Chabannon C. De La Camara R. Dolstra H. Duarte R.F. Glass B. Greco R. Indications for hematopoietic cell transplantation for hematological diseases, solid tumors, and immune disorders: Current practice in Europe, 2022 Bone Marrow Transpl.2022571217123910.1038/s 41409-022-01691-w 35589997 PMC 9119216 · doi ↗ · pubmed ↗
- 2Zurko J. Ramdial J. Shadman M. Ahmed S. Szabo A. Iovino L. Tomas A.A. Sauter C. Perales M.-A. Shah N.N. Allogeneic transplant following CAR T-cell therapy for large B-cell lymphoma Haematologica 20221089810910.3324/haematol.2022.28124235833303 PMC 9827150 · doi ↗ · pubmed ↗
- 3RochéP. Brisou G. Furst S. Noel R. Montes De Oca C. Collignon A. Inchiappa L. Schiano De Colella J.M. Brenot Rossi I. Reichert T. Allogeneic Transplant as a Curative Option for Relapsed/Refractory Large B-Cell Lymphoma in the Era of CAR T-Cell Therapy: A Monocentric Retrospective Study Blood 20221407740774110.1182/blood-2022-157915 · doi ↗
- 4Glass B. Hasenkamp J. Wulf G. Dreger P. Pfreundschuh M. Gramatzki M. Silling G. Wilhelm C. Zeis M. Gorlitz A. Rituximab after lymphoma-directed conditioning and allogeneic stem-cell transplantation for relapsed and refractory aggressive non-Hodgkin lymphoma (DSHNHL R 3): An open-label, randomised, phase 2 trial Lancet Oncol.20141575776610.1016/S 1470-2045(14)70161-524827808 · doi ↗ · pubmed ↗
- 5Corradini P. Dodero A. Farina L. Fanin R. Patriarca F. Miceli R. Matteucci P. Bregni M. ScimèR. Narni F. Allogeneic stem cell transplantation following reduced-intensity conditioning can induce durable clinical and molecular remissions in relapsed lymphomas: Pre-transplant disease status and histotype heavily influence outcome Leukemia 2007212316232310.1038/sj.leu.240482217597807 · doi ↗ · pubmed ↗
- 6Solomon S.R. Sizemore C.A. Sanacore M. Zhang X. Brown S. Holland H.K. Morris L.E. Bashey A. Haploidentical Transplantation Using T Cell Replete Peripheral Blood Stem Cells and Myeloablative Conditioning in Patients with High-Risk Hematologic Malignancies Who Lack Conventional Donors is Well Tolerated and Produces Excellent Relapse-Free Survival: Results of a Prospective Phase II Trial Biol. Blood Marrow Transplant.2012181859186610.1016/j.bbmt.2012.06.01922863841 · doi ↗ · pubmed ↗
- 7Ciurea S.O. Shah M.V. Saliba R.M. Gaballa S. Kongtim P. Rondon G. Chen J. Wallis W. Cao K. Konopleva M. Haploidentical Transplantation for Older Patients with Acute Myeloid Leukemia and Myelodysplastic Syndrome Biol. Blood Marrow Transplant.2018241232123610.1016/j.bbmt.2017.09.00528918304 PMC 7172017 · doi ↗ · pubmed ↗
- 8Castagna L. Bramanti S. Devillier R. Sarina B. Crocchiolo R. Furst S. Granata A. Faucher C. Harbi S. Morabito L. Haploidentical transplantation with post-infusion cyclophosphamide in advanced Hodgkin lymphoma Bone Marrow Transpl.20175268368810.1038/bmt.2016.34828092347 · doi ↗ · pubmed ↗