Observational, causal relationship and shared genetic basis between cholelithiasis and gastroesophageal reflux disease: evidence from a cohort study and comprehensive genetic analysis
Yanlin Lyu, Shuangshuang Tong, Wentao Huang, Yuying Ma, Ruijie Zeng, Rui Jiang, Ruibang Luo, Felix W Leung, Qizhou Lian, Weihong Sha, Hao Chen

TL;DR
This study finds a strong observational and genetic link between gallstones and GERD, suggesting shared causes and potential for new treatments.
Contribution
The study identifies five shared genetic loci and three novel risk genes linking cholelithiasis and GERD.
Findings
Individuals with cholelithiasis have nearly double the risk of developing GERD.
Genetic liability to cholelithiasis causally increases the risk of GERD.
Five novel shared genetic loci and three risk genes (SUN2, CBY1, JOSD1) were identified.
Abstract
Cholelithiasis and gastroesophageal reflux disease (GERD) contribute to significant health concerns. We aimed to investigate the potential observational, causal, and genetic relationships between cholelithiasis and GERD. The observational correlations were assessed based on the prospective cohort study from UK Biobank. Then, by leveraging the genome-wide summary statistics of cholelithiasis (N = 334,277) and GERD (N = 332,601), the bidirectional causal associations were evaluated using Mendelian randomization (MR) analysis. Subsequently, a series of genetic analyses was used to assess the genetic correlation, shared loci, and genes between cholelithiasis and GERD. The prospective cohort analyses revealed a significantly increased risk of GERD in individuals with cholelithiasis (hazard ratio [HR] = 1.99; 95% confidence interval [CI], 1.89–2.10) and a higher risk of cholelithiasis among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
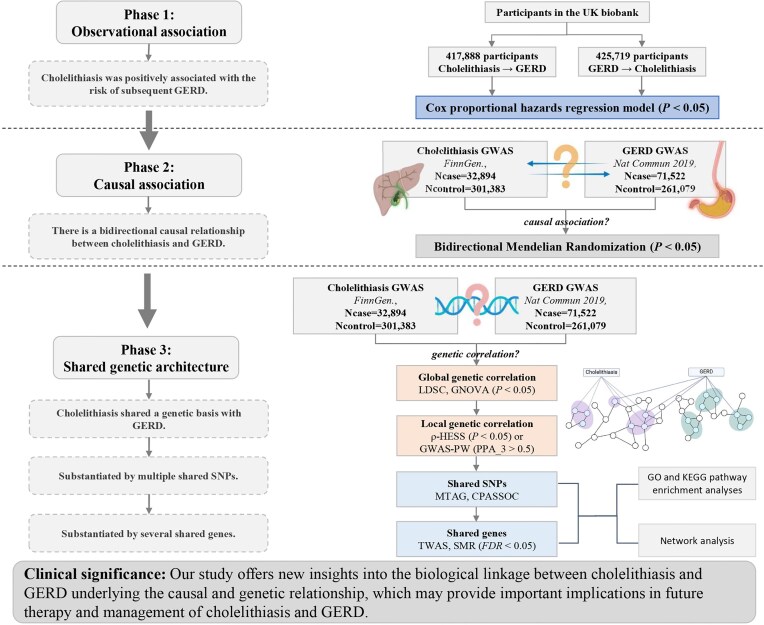 Figure 1
Figure 1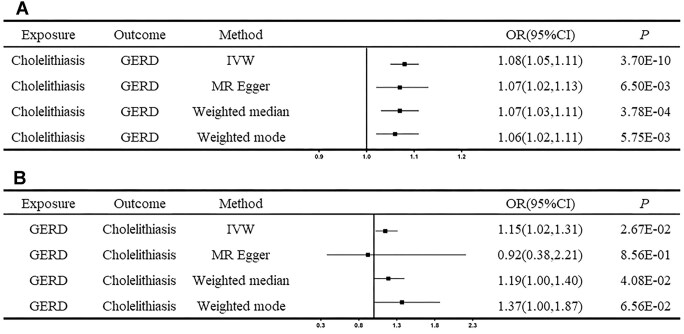 Figure 2
Figure 2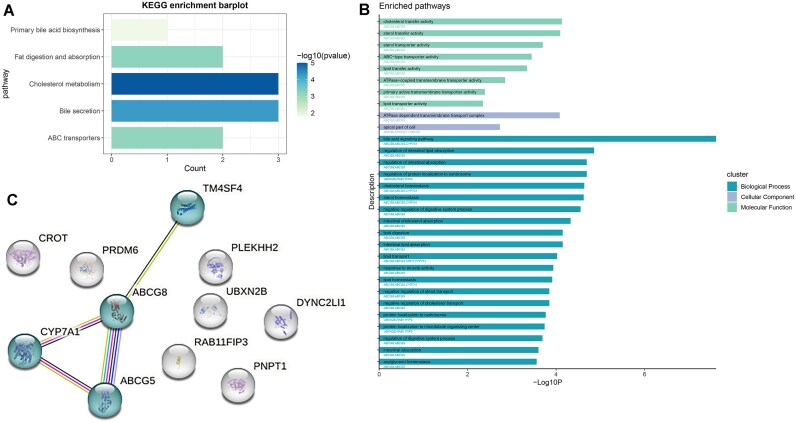 Figure 3
Figure 3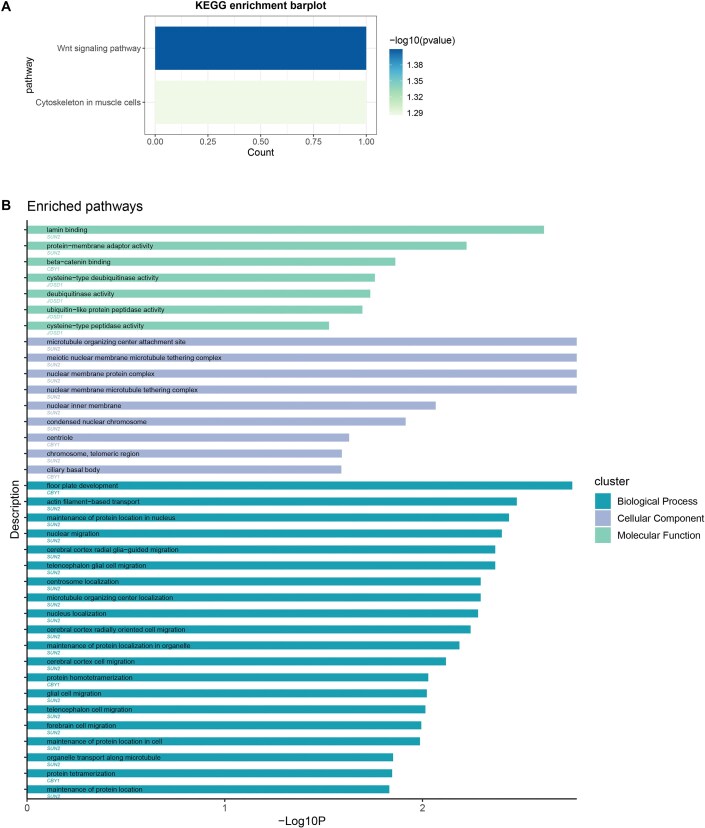 Figure 4
Figure 4| Case/person-years | Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) |
| HR (95% CI) |
| HR (95% CI) |
| ||
|
| 20,780/2,649,797 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| Cholelithiasis | 1,628/86,654 | 2.40 (2.30–2.52) | <0.001 | 2.28 (2.17–2.40) | <0.001 | 1.99 (1.89–2.10) | <0.001 |
|
| |||||||
| Non-GERD | 5,883/2,372,960 | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| GERD | 1,066/220,497 | 2.86 (2.70–3.02) | <0.001 | 2.69 (2.54–2.84) | <0.001 | 2.30 (2.18–2.44) | <0.001 |
| Cholelithiasis | GERD | ||
|---|---|---|---|
| Total liability scale heritability | LDSC without constraining the intercept | 0.1695 | 0.1251 |
| Total liability scale heritability | LDSC with constraining the intercept | 0.2665 | 0.1401 |
| Observed heritability | GNOVA | 0.0659 | 0.0768 |
| Genetic correlation (rg), | LDSC without constraining the intercept | 0.3053, 2.77 × 10–27 | |
| Genetic correlation (rg), | LDSC with constraining the intercept | 0.2499, 3.90 × 10–56 | |
| Genetic correlation (rg), | GNOVA | 0.2625, 2.50 × 10–32 | |
| SNP | Chromosome | Base pairs | A1 | A2 | Odds ratio | Cross-trait meta-analyses |
|
| Gene | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cholelithiasis | GERD | MTAG | CPASSOC | Cholelithiasis | GERD | |||||||
|
| 2 | 56,004,781 | T | C | 1.055259069 | 1.041435448 |
|
| 9.28E-06 | 7.90E-07 |
|
|
|
| 2 | 53,201,324 | T | C | 1.033076972 | 1.02716235 |
|
| 3.38E-06 | 1.10E-06 |
|
|
|
| 5 | 122,503,245 | G | A | 1.033058996 | 0.973653294 |
|
| 2.58E-06 | 5.66E-07 |
|
|
|
| 8 | 62,948,007 | G | A | 1.157742514 | 0.927187007 |
|
| 5.03E-06 | 3.49E-06 |
|
|
|
| 16 | 570,557 | C | T | 1.037051717 | 0.975700114 |
|
| 8.29E-07 | 2.31E-06 |
|
|
| rs146812426 | 2 | 43,909,666 | A | G | 1.733518226 | 1.057174729 |
|
| 1.26E-93 | 2.48E-08 | 3.68E-121 |
|
| rs4299376 | 2 | 44,072,576 | T | G | 1.3178505 | 1.017247042 |
|
| 5.88E-124 | 2.12E-12 | 2.10E-158 |
|
| rs6733452 | 2 | 44,094,845 | A | G | 1.775888747 | 1.085672923 |
|
| 1.63E-120 | 9.66E-14 | 1.04E-151 |
|
| rs7596134 | 2 | 44,052,833 | A | C | 1.324747665 | 1.018366629 |
|
| 8.81E-175 | 3.78E-15 | 8.31E-227 |
|
| rs4681515 | 3 | 149,212,076 | G | A | 0.879264075 | 1.024597651 |
|
| 1.35E-48 | 5.58E-11 | 3.67E-55 |
|
| rs9297994 | 8 | 59,392,324 | A | G | 0.888037773 | 0.974529976 |
|
| 2.25E-40 | 2.40E-10 | 1.06E-44 |
|
| rs10935762 | 3 | 149,216,298 | T | C | 0.850727852 | 0.960117122 |
|
| 5.12E-42 | 1.33E-09 | 1.55E-47 |
|
| rs3922717 | 6 | 27,030,924 | G | A | 0.959186164 | 1.043833506 |
|
| 2.16E-08 | 1.99E-11 | 1.07E-13 |
|
| rs12633863 | 3 | 149,211,512 | A | G | 0.878788522 | 0.977457956 |
|
| 2.03E-48 | 2.63E-10 | 1.56E-55 |
|
| rs802036 | 7 | 86,977,894 | C | T | 0.865221271 | 1.050850672 |
|
| 5.58E-21 | 5.84E-09 | 1.52E-22 |
|
- —National Natural Science Foundation of China10.13039/501100001809
- —Natural Science Foundation
- —Minister of Science and Technology of China
- —Natural Science Foundation of Guangdong Province10.13039/501100003453
- —Guangdong Science and Technology Department10.13039/501100007162
- —High-level Hospital Construction Project of Guangdong Provincial People’s Hospital10.13039/501100018609
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Esophageal and GI Pathology · Gastrointestinal disorders and treatments
Introduction
Cholelithiasis, a condition characterized by lithic deposits of either cholesterol or bilirubin in the gallbladder or the bile ducts, is one of the most prevalent digestive disorders, imposing a significant socioeconomic burden [1]. Cholelithiasis affects nearly 20% of the adult population worldwide, with a continuously rising incidence rate [1, 2]. The development of cholelithiasis involves intricate mechanisms, encompassing genetic and environmental factors and their interactions. [1, 3] Gastrointestinal defects in patients with cholelithiasis have raised widespread concerns and require further exploration [1, 4].
Gastroesophageal reflux disease (GERD) is a common gastrointestinal disorder typically characterized by recurrent heartburn and regurgitation [5, 6]. This condition could pose a substantial public health challenge, owing to its association with a spectrum of subsequent severe complications, including Barrett’s esophagus, esophageal stenosis, and esophageal adenocarcinoma [7]. Therefore, early identification and vigilant monitoring of individuals at high risk for GERD can facilitate timely intervention, potentially mitigating the severity of the disease and decreasing the risk of GERD and GERD-related complications.
Several studies have investigated the correlation between cholelithiasis and the risk of GERD [8–11]. Nonetheless, the existing findings have been inconsistent and insufficient, lacking support from prospective studies. For instance, a retrospective, observational study involving 1,381,004 individuals with gallstone disease found that 40% of the patients had concurrent GERD [11]. On the contrary, a case-control study, comprising 790 cases and 407 controls demonstrated no associations between the presence of cholelithiasis and GERD [9]. Most of the previous studies are outdated and statistically underpowered due to small sample sizes. In addition, these observational studies are prone to some inevitable defects such as potential reverse causality and confounding [12]. The causal association between cholelithiasis and GERD remains obscure. Therefore, large datasets and updated methodologies are warranted to disentangle the conflicting relationship between them and to further reveal the underlying genetic underpinnings.
The evolution of genetic statistical methods has facilitated the understanding of the interconnected genetic basis of complex diseases, providing novel perspectives on the potential biological mechanisms behind the epidemiologic correlations. In our study, we initiated a comprehensive evaluation of the correlations and the shared genetic basis between cholelithiasis and GERD via a prospective cohort study, Mendelian randomization (MR) analyses, and a range of genetic analyses (Fig. 1).
Flowchart of the overall study design. First, we assessed the phenotypic correlations between cholelithiasis and GERD based on the prospective cohort data from the UK Biobank. Second, we conducted a bidirectional 2-sample Mendelian randomization analysis to investigate the causality by using large-scale GWAS data. Third, we utilized a variety of approaches to dissect the genetic correlations and shared genetic architecture. LDSC and GNOVA methods were applied to detect the global genetic correlation. ρ-HESS and GWAS-PW methods were used to further explore the local genetic correlation. Then, MTAG and CPASSOC methods were employed to find the shared-risk SNPs. Finally, TWAS and SMR methods were utilized to study the shared genes between cholelithiasis and GERD. CPASSOC: cross-phenotype association test; FDR: false discovery rate; GERD: gastroesophageal reflux disease; GNOVA: genetic covariance analyzer; GO, Gene Ontology Biological Process; GWAS: genome-wide association study; GWAS-PW: pairwise genome-wide association study; KEGG, Kyoto Encyclopedia of Genes and Genomes; LDSC: linkage disequilibrium score regression; MTAG: multitrait analysis of genome-wide association study; SMR: summary data-based Mendelian randomization; SNP: single nucleotide polymorphism; TWAS: transcriptome-wide association studies; ρ-HESS: heritability estimator from summary statistics.
Methods
Data summary
Prospective data from the UK Biobank
The UK Biobank (UKB) is a large-scale prospective cohort study with 502,368 participants aged 37–73 years who were recruited between 2006 and 2010 [13]. Participants visited 1 of 22 assessment centers across England, Scotland, and Wales to complete touch-screen questionnaires, verbal interviews, and physical measurements at recruitment.
Data on hospital admissions were collected regularly through linkages to the Scottish Morbidity Records, the Patient Episode Database, and Health Episode Statistics. Information on death was obtained from the National Health Service Central Register and National Health Service Digital. This study was conducted under the UK Biobank project 83339. The UK Biobank received ethical approval from the North West Multi-Centre Research Ethics Committee (21/NW/0157, 16/NW/0274, and 11/NW/0382).
Diagnostic information was sourced from primary care data, hospital admission data, and death registry records. We defined diagnoses according to the International Classification of Diseases, 10th revision (ICD-10) code K80 for cholelithiasis and K21 for GERD, respectively.
As shown in the flowchart (Supplementary Fig. S1), participants with self-reported cholelithiasis or GERD (N = 13,320) or without follow-up data (N = 1,298) were excluded, leaving 487,750 individuals. To ensure a similar distribution of follow-up time between groups, the index date of participants in the control group was manually assigned based on the distribution of the first diagnosis date of those patients with diseases of interest when conducting corresponding analyses. After excluding 69,862 participants with a history of GERD before the index date, 417,888 participants were finally included to analyze the association between cholelithiasis and GERD. After excluding 62,031 participants with a history of cholelithiasis before the index date, 425,719 participants were finally included to analyze the association between GERD and cholelithiasis.
Follow-up time was calculated from the index date to the time to diagnosis of outcome of interest or the censoring date (30 October 2022) or death, whichever occurred first.
Genome-wide association study datasets
Genome-wide association study (GWAS) summary data for cholelithiasis were obtained from the FinnGen databases comprising 32,894 cholelithiasis cases and 301,383 controls of European ancestry [14]. The cholelithiasis dataset was defined with the ICD-10 code K80, ICD-9 code 574, and ICD-8 code 574.
GWAS summary data for GERD were obtained from a meta-analysis of 332,601 individuals including 71,522 cases and 261,079 controls of European ancestry combining the 2 largest existing genetic studies of GERD (UKB and the QSkin study) [15]. The phenotypes ranged from self-reported GERD, ICD-10, and use of GERD medication. For the replication dataset of GERD, we utilized the summary data with 129,080 European ancestry cases and 473,524 European ancestry controls from the UK and Australian population [16]. Detailed information of sample collection, quality control, and imputation process for these datasets has been explained in the original articles [14–16]. There is no population overlap between the datasets for cholelithiasis and GERD. The GWAS summary datasets utilized in this research are publicly available, and the ethical statements can be found in the original publications corresponding to the data. Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Statistical analysis
Observational analysis
To handle the missing data of the covariates, we applied multiple imputation by chained equations (MICE packages in R) [17] with a predictive mean matching method that combining regression models and nearest-neighbor matching. Five imputations and 50 iterations were performed, and 1 of the 5 imputations was selected randomly as the final imputed data set.
We constructed a Cox proportional hazards regression model with exposure to cholelithiasis to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs). The proportional hazards assumption was tested by Schoenfeld residuals tests, and no evidence of violation was found. Three sets of adjustments were established to minimize the role of confounding. Model 1 was without any adjustments. Model 2 was adjusted only for age and sex. Model 3 was further adjusted for ethnicity, average total annual household income, deprivation index, body mass index (BMI), alcohol consumption, smoking status, physical activity, education, fresh fruit consumption, raw vegetable consumption, tea consumption, coffee consumption, hypertension, diabetes, renal failure, myocardial infarction, stroke, chronic obstructive pulmonary disease, asthma, anxiety, depression, and peptic ulcer. All analyses were performed using RStudio (RRID:SCR_000432) and R 4.2.1 software. Statistical significance was set at a 2-tailed P value of less than 0.05.
Mendelian randomization analysis
We performed the bidirectional MR analysis to explore the potential causal relationship between cholelithiasis and GERD, using R packages “TwoSampleMR” [18], and “MR-PRESSO” [19] in R software (version 4.2.1). MR analysis utilizes genetic variants as instruments, and the validity of its causal inference relies on 3 critical assumptions of independence, relevance, and exclusion restriction [20]. These assumptions are indispensable for mitigating bias and establishing causality. Only significant single nucleotide polymorphisms (SNPs) independently associated with the exposure at a P threshold of 5 × 10^–8^ and satisfying the linkage disequilibrium (LD) criteria of r^2^ < 0.001 and kb > 10,000 were identified as instruments in MR studies. Additionally, we searched the instrumental variables in the GWAS catalog [21] to identify potential confounders like BMI, smoking, and certain dietary habits and excluded the confounding variants from further analyses.
We employed inverse variance weighting (IVW) [22] as the main MR approach, complemented by 3 additional sensitivity analysis methods, including MR-Egger [23], weighted median [24], and weighted mode [25], to detect the causal relationships between cholelithiasis and GERD. Different methods were based on different assumptions concerning the influence of horizontal pleiotropy. The IVW MR model, assuming balanced pleiotropy, applies multiplicative random effects to meta-analyze the Wald estimates of each SNP [22]. The MR-Egger model allows the uncorrelated directional pleiotropy by adding a nonzero intercept that relaxes the assumption of relevance of selected genetic variants [23]. The weighted median and weighted mode models remain robust when up to 50% or more of genetic variants are valid, which exhibit greater resilience to pleiotropy [24, 25].
We conducted the MR-Egger intercept test, Cochran’s Q statistic, MR-PRESSO, and leave-one-out analysis to evaluate the heterogeneity, pleiotropy, and potential outliers of the MR results. If heterogeneity is detected in the MR analysis (P < 0.05), we would recalculate the MR estimates after the removal of outliers identified with a P value of less than 1 in the MR-PRESSO outlier test to ensure the robustness of the MR results. The MR analysis in this research has been documented in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline specific for MR study.
Global genetic correlation analysis
To quantify the heritability of each trait and the global genetic correlation between cholelithiasis and GERD, we applied linkage disequilibrium score regression (LDSC) method with Python 2.7 [26]. Based on precomputed LD scores derived from 1000 Genomes reference data of European population, we selected SNPs that matched the reference panel (minor allele frequency [MAF] > 0.01 and INFO score > 0.9) in the GWAS datasets [27]. We used univariate LDSC to estimate SNP heritability for each trait and bivariate LDSC to calculate the genetic correlations between cholelithiasis and GERD with and without constraining the intercept. Based on the prevalence rates of 20% [1] for cholelithiasis and 17.1% [6] for GERD, we calculated the liability scale of the reported heritability for both traits. The genetic correlation with a P value less than 0.05 was considered significant [28, 29].
Additionally, we employed the genetic covariance analyzer (GNOVA) as a supplementary method to validate the genetic correlations. The steps of quality control on GWAS datasets are similar to the LDSC method [30]. More detailed descriptions are in the original study [31]. Based on the framework of the annotation-stratified genetic covariance estimation, GNOVA provides a more powerful statistical inference of the shared genetic basis between complex traits and shows higher estimation accuracy. Threshold of P < 0.05 was regarded as strong evidence for MAF-stratified genetic correlation [31].
Local genetic correlation analysis
To identify whether cholelithiasis and GERD have genetic correlation in local genomic region, we further applied the heritability estimator from summary statistics (ρ-HESS) with Python 2.7 [32]. We first calculated the LD block and eigenvalues by referring to the 1000 Genomes Project of Europeans. Then, we explored the local SNP heritability for each trait and estimated the local genetic correlation in 1,613 approximately LD-independent regions [33]. Suggestive genetic associations with a P value less than 0.05 were noted.
Similarly, pairwise-GWAS (GWAS-PW) was supplemented to explore the significant shared local regions [34]. Based on the Bayesian statistical framework, GWAS-PW calculated the posterior probabilities of association (PPAs) for each genomic region across 4 models. Genomic regions with a PPA of model 3 larger than 0.5 were considered significantly associated with both traits, in accordance with a previous article [35, 36].
Cross–trait meta–analysis
To detect the shared genetic variants in cholelithiasis and GERD, we performed multitrait analysis of GWAS (MTAG) [37]. MTAG is based on a fundamental assumption that all SNPs exhibit the same variance–covariance matrix of effect sizes and heritability across traits. To meet the assumption, we rigorously filtered the MTAG SNP with MAF ≥1% and sample size ≥75% of the 90th percentile and dropped the outliers [37]. By joint analysis of multiple traits, MTAG substantially enhances the statistical power to detect the genetic associations for each trait and generate trait-specific estimates for each SNP. To identify the significant and independent loci, we utilized the threshold PMTAG < 5 × 10^–8^ and the “clumping” function of PLINK (settings: clump_p1 = 5e^−8^, clump_p2 = 1e^−5^, clump_r^2^ = 0.2, clump_kb = 500) [38].
Cross-phenotype association test (CPASSOC) is a complementary method to deduce the shared risk SNPs between complex traits [39]. Compared with the single-trait analysis, CPASSOC improves statistical power and reasonably controlled type I error rate. Considering the heterogeneity effects for different phenotypes, we primarily used the heterogeneous version of cross-phenotype statistic (Shet) method to integrate association evidence of different but correlated traits [40]. Given the inherent variability induced by the random sampling analysis embedded in this method, we set a random seed to 123 to ensure a reproducible result. After getting the estimates, we identified the independent loci using the “clumping” function of PLINK (settings as before). The variant in each locus with the smallest P value was regarded as the index SNP. Index SNPs that met the criteria of PCPASSOC < 5 × 10^–8^ and Peach trait < 1 × 10^–3^ were deemed significant pleiotropic SNPs. Newly discovered pleiotropic SNPs were defined as those significant pleiotropic SNPs that were not genome-wide significant (5 × 10^–8^ < Peach trait < 1 × 10^–3^) and independent (r^2^ < 0.20) of earlier identified trait-related genome-wide significant SNPs, and all their adjacent SNPs (±500 kb) did not reach P < 5 × 10^–8^ in each GWAS dataset.
We used dbSNP [41] and 3DSNP [42] for detailed functional annotation of the identified pleiotropic SNPs.
Transcriptome–wide association analysis
Numerous genetic variants impact intricate traits through the regulation of gene expression. To identify significant gene–trait associations, we implemented a transcriptome-wide association scan (TWAS) leveraging FUSION software [43]. Based on the LD reference data of European 1000 Genomes, we converted the GWASs of cholelithiasis and GERD into an LD-score format. We prioritized the trait-related tissues; thus, we prepared the expression quantitative trait loci (eQTL) data of whole blood, liver, stomach, and esophagus-related tissues from GTEx v8 (Genotype-Tissue Expression, version 8) [43]. By integrating the precomputed phenotypic summary data and corresponding eQTL data, we identified significant tissue-specific genes with a false discovery rate (FDR) <0.05 for each trait and selected genes that overlapped between cholelithiasis and GERD in the same tissue.
Summary data-based Mendelian randomization (SMR) analysis is a complementary method to deduce the causative genes underlying cholelithiasis and GERD [44]. We used the eQTL data of whole blood, liver, stomach, and esophagus-related tissues from GTEx v8 [45] and cis-eQTL data of whole blood from the eQTLGen consortium [46]. The heterogeneity in dependent instruments (HEIDI) test was conducted to distinguish pleiotropy or causality from linkage. We primarily focused on the genes with FDR < 0.05 and passed the P value thresholds for the HEIDI test (PHEIDI > 0.05) [44].
The pathway enrichment analyses and biomolecular network analyses
To gain shared biological insights into cholelithiasis and GERD, we conducted functional annotation of the pleiotropic SNPs and shared genes using multiple methods. We utilized the knowledge-based Kyoto Encyclopedia of Genes and Genomes (KEGG) and Gene Ontology (GO) databases to perform pathway enrichment analyses for identifying pathways associated with these genes, using the ClusterProfiler R package (RRID:SCR_016884) [47, 48]. P values from the pathway enrichment analyses were adjusted for multiple comparisons through the FDR approach. In addition, we utilized the STRING database [49] to find the interactions mapped to the pleiotropic SNPs and shared functional genes.
Results
Observational association between cholelithiasis and GERD
Baseline characteristics of the study cohort by cholelithiasis are presented in Supplementary Table S1. In total, participants were followed for 2,736,451 person-years, during which 1,628 cholelithiasis patients and 20,780 non-cholelithiasis individuals developed GERD (Table 1A). In the age/sex-adjusted model, the risk of GERD was 2.28 times higher in cholelithiasis patients compared to those without cholelithiasis. In the fully adjusted model, the risk of GERD remained statistically significant in cholelithiasis patients (HR = 1.99; 95% CI, 1.89–2.10; P < 0.001).
Moreover, we also observed the association between baseline GERD and incident cholelithiasis, as shown in Table 1B. In the age/sex-adjusted model, the HR for cholelithiasis was 2.69 (95% CI, 2.54–2.84; P < 0.001) for GERD patients. In the fully adjusted model, the GERD group also displayed a significantly increased risk of developing cholelithiasis (HR = 2.30; 95% CI, 2.18–2.44, P < 0.001).
Causal association between cholelithiasis and GERD
After excluding the confounding instrumental variables, we used 46 cholelithiasis-associated and 20 GERD-associated genetic instruments (Supplementary Table S2), respectively, in the analyses and provided evidence for the causal association between cholelithiasis and GERD. Genetically determined cholelithiasis has the possibility to increase the risk of GERD by 8% (IVW OR = 1.08; 95% CI, 1.05–1.11; P = 3.70 × 10^–10^; Fig. 2A, Supplementary Table S3), which was further validated by the other 3 MR methods and the analyses with a supplementary dataset (Supplementary Table S4). Besides, we also conducted a reverse MR analysis and found that genetically predicted GERD could increase the risk of cholelithiasis by 15% (OR = 1.15; 95% CI, 1.02–1.31; P = 0.027) according to IVW method (Fig. 2B, Supplementary Table S3). This association was further validated through analyses employing the weighted median method and an additional dataset (Supplementary Tables S3–S4), although it could not be confirmed using the MR-Egger and the weighted mode methods.
The causal associations between cholelithiasis and GERD. (A) The causal effect of cholelithiasis on GERD. (B) The causal effect of GERD on cholelithiasis. Error bars represent the 95% CIs for the estimates. CI: confidence interval; GERD: gastroesophageal reflux disease; IVW: inverse variance weighted.
The F statistic of each SNP related to cholelithiasis and GERD was larger than the empirical threshold of 10, suggesting little possibility of weak instrument bias (Supplementary Table S2). We also performed several sensitive analyses to validate the causal association between cholelithiasis and GERD. Cochran’s Q test in the IVW model and the MR-Egger model suggested a lack of evidence for the existence of heterogeneity in effects across the instrumental variables. The P value of the MR-Egger intercept test was larger than 0.05, which indicated that there was a lower possibility of horizontal pleiotropy in the causal estimates (Supplementary Tables S3–S4). The leave-one-out analysis suggested that the observed causal relationship was not influenced by any outliers (Supplementary Figs. S2–S3). The scatterplots, forest plots, and funnel plots of the MR results are displayed in Supplementary Figs. S2–S3.
Global and local genetic correlations between cholelithiasis and GERD
SNP-based liability-scale heritability h² for cholelithiasis and GERD was 26.65% and 14.01% when utilizing the univariate LDSC with constraining the intercept. The observed heritability of cholelithiasis and GERD was 6.60% and 7.68% utilizing GNOVA. The cross-trait LDSC suggested that cholelithiasis had a relatively strong positive genetic correlation with GERD, exhibiting a genetic correlation (r_g_) of 0.31 and a P value of 2.77 × 10^–27^. After constraining the intercept, the genetic correlation was decreased but remained significant (r_g_ = 0.25, P = 3.90 × 10^–56^). This finding was consistent with the GNOVA analysis, reflecting a genetic correlation (r_g_) of 0.26 and a P value of 2.50 × 10^–32^ (Table 2).
We also tested the local genetic correlation by ρ-HESS and GWAS-PW (Supplementary Table S5). Seven suggestively significant regions were identified by ρ-HESS, and 8 significant regions were identified by GWAS-PW. Four regions were overlapped according to ρ-HESS and GWAS-PW. These findings suggested a potential shared genetic foundation, necessitating further exploration to elucidate the underlying biological mechanisms.
Identification of shared risk loci for cholelithiasis and GERD
MTAG identified 8 independent pleiotropic loci (rs146812426, rs4299376, rs6733452, rs7596134, rs4681515, rs9297994, rs10935762, rs3922717), which were also significant in CPASSOC (Table 3, Supplementary Table S6). CPASSOC found 23 pleiotropic loci, 5 of which were significant in MTAG, including rs9297994, rs10935762, rs3922717, rs12633863, and rs802036 (Table 3, Supplementary Table S7). Overall, 10 independently significant loci have been identified as shared between cholelithiasis and GERD by both MTAG and CPASSOC, namely, rs146812426, rs4299376, rs6733452, rs7596134, rs10935762, rs12633863, rs4681515, rs3922717, rs802036, and rs9297994, which mapped to 9 genes, including PLEKHH2, ABCG8, DYNC2LI1, ABCG5, TM4SF4, LOC100270746, CROT, UBXN2B, and CYP7A1 (Table 3). It is worth noting that 5 novel pleiotropic loci were identified in the CPASSOC analysis, including rs10167227, rs6742945, rs335208, rs72664027, and rs11537754, which mapped to genes PNPT1, LOC105369165, PRDM6, LINC02842, and RAB11FIP3, respectively (Table 3, Supplementary Table S7). Other SNP-associated genes are listed in Supplementary Tables S6–S7.
After multiple corrections, the pathway enrichment analysis using the KEGG database identified 5 pathways according to the above genes, including cholesterol metabolism, bile secretion, fat digestion and absorption, ABC transporters, and primary bile acid biosynthesis (Fig. 3A, Supplementary Table S8). The pathway enrichment analysis using the GO database identified 65 biological processes, 2 cellular components, and 8 molecular functions; most of these pathways are related to lipid and bile acid metabolism (Fig. 3B, Supplementary Table S9). In the network analysis, we observed a close association among TM4SF4, CYP7A1, ABCG5, and ABCG8 (Fig. 3C).
Enriched pathways identified using KEGG and GO databases and network of genes associated with pleiotropic variants. (A) Enriched pathways identified using the KEGG database. (B) Enriched pathways identified using the GO database. (C) The network of genes associated with pleiotropic variants.
Identification of shared genes for cholelithiasis and GERD
Results from tissue-specific TWAS and SMR revealed gene-level genetic overlap. After FDR corrections, a total of 15 genes were shared by cholelithiasis and GERD and enriched in 6 tissues, including blood, liver, esophagus mucosa, esophagus muscularis, esophagus gastroesophageal junction, and stomach in the TWAS analysis (Supplementary Table S10). Among them, 7 genes significantly overlapped in 2 or more tissues. Five of 7 genes (SUN2, CBY1, JOSD1, DDX17, FAM227A) were located in 22q13.1. The TWAS analysis showed that overexpression of SUN2, JOSD1, and CBY1 was negatively associated with the risk of cholelithiasis and GERD in the blood and esophagus-related tissues, while overexpression of JOSD1 and CBY1 was positively associated with these 2 diseases in the liver tissue. SUN2, JOSD1, and CBY1 also displayed a significant SMR association signal with FDR < 0.05 and passed the HEIDI-outlier test in blood, esophagus mucosa, and esophagus muscularis (Supplementary Table S11). No significant shared causal gene was found in other tissues, namely liver, esophagus gastroesophageal junction, and stomach, according to SMR results.
Using the KEGG database, we found 2 significantly enriched pathways, Wnt signaling pathway (CBY1) and cytoskeleton in muscle cells (SUN2) (Fig. 4A, Supplementary Table S12). Wnt signaling pathway (CBY1) also enriched significantly in the GO pathway enrichment analysis, which is shown in Fig. 4B and Supplementary Table S13. In the network analysis, we did not identify the association between these 3 shared genes.
Enriched pathways of shared genes identified using KEGG and GO databases. (A) Enriched pathways identified using the KEGG database. (B) Enriched pathways identified using the GO database.
Discussion
To our knowledge, this is the first study to comprehensively explore the observational, causal, and genetic relationships between cholelithiasis and GERD. By leveraging UK Biobank data and GWAS data, we found the bidirectional causal relationship between cholelithiasis and GERD. The subsequent genetic analyses provided new insights into their shared genetic basis and related biological mechanism, which may contribute to the prediction, diagnosis, and treatment of these diseases.
Previous research has reported that cholelithiasis and GERD shared numerous common etiological risk factors such as obesity [50], type 2 diabetes mellitus [51], depression [52], and smoking [53]. We conducted a Cox proportional hazards regression model analysis using the UKB cohort, with adjustments for a wide range of established and potential confounders associated with these 2 conditions. Although the HRs were slightly attenuated after controlling the covariates, the bidirectional association between cholelithiasis and GERD remained statistically significant. This is consistent with the findings by Unalp-Arida et al. [11] and Portincasa et al. [8], which reported a statistically significant association between cholelithiasis and GERD. Subsequently, using the MR approach, we identified bidirectional causality between cholelithiasis and GERD, while the pathophysiologic mechanisms underlying the causal relationship remain unclear. Previous studies suggested that patients with gallstones showed impaired gastric motility [4, 8], which might be related to the pathogenesis of GERD. Meanwhile, patients with GERD presented a higher incidence of gallbladder dyskinesia [54, 55], which may be attributed to the routine use of proton pump inhibitors (PPIs) in GERD treatment. It has been reported that PPIs could reduce the release of cholecystokinin, which might diminish gallbladder motility, thereby causing the formation of gallstones [56]. The current evidence indicated the potential shared pathogenesis or genetic basis between cholelithiasis and GERD, warranting further exploration.
In the analysis of heritability and genetic correlation, the heritability of cholelithiasis and GERD was estimated to be 17% and 13%, respectively, indicating a significant genetic contribution to the etiology of both diseases, consistent with previous studies [15, 57]. The genetic correlation between cholelithiasis and GERD was 0.31, suggesting a moderate to strong genetic association between these conditions. The finding supports the hypothesis that genetic factors, such as local genetic correlations, shared loci, and common functional genes, play an important role in the co-occurrence of cholelithiasis and GERD. We identified 4 regions that exhibited a suggestively significant local genetic association, as evidenced by ρ-HESS < 0.05 and GWAS-PW > 0.5. Most loci identified by MTAG and CPASSOC were situated within these regions. Moreover, we found that 22q13.1 might be a shared region between gallstone disease and GERD by combining analyses of local genetic correlation, shared loci, and shared genes: First, this region showed suggestively significant local genetic association between cholelithiasis and GERD using GWAS-PW. Second, the shared loci rs1056661, identified by CPASSOC, were located within this region. Third, 5 and 3 overlapped genes, identified from TWAS analysis and SMR, respectively, were situated within this region. Previous studies have reported that several significant loci related to gallstone disease, including rs12004, rs41281265, and rs1946990, were in this region [58, 59]. However, currently, there is no research linking this region to GERD. Future research is warranted to delve deeper into this specific region to elucidate the genetic correlation between gallstone disease and GERD.
Given the significant genetic correlation observed, we conducted cross-trait GWAS meta-analyses to detect risk SNPs underlying the joint phenotypes of cholelithiasis–GERD. We identified 10 shared independently significant loci through MTAG and CPASSOC. According to the results of pathway enrichment analyses, the genes associated with these loci were enriched in pathways related to lipid and bile acid metabolism, including cholesterol metabolism, bile secretion, ABC transporters, and primary bile acid biosynthesis. Several studies have reported that aberrant lipid and bile acid metabolism contributes to the development of both cholelithiasis and GERD [1, 60–62]. ABCG5 (index SNP: rs7596134), ABCG8 (index SNP: rs4299376 and rs6733452), and CYP7A1 (index SNP: rs9297994) are associated with lipid metabolism. Numerous investigations have suggested the involvement of these genes in the development of gallstone disease [63–65]. Although several studies have reported that obesity [50] and dyslipidemia [60] are risk factors for GERD, no research has investigated the involvement of these genes in GERD. Therefore, the relationship between these genes and GERD warrants further investigation. Additionally, 5 new loci associated with cholelithiasis and GERD were identified via CPASSOC analysis. PNPT1 (index SNP: rs10167227) is associated with the mitochondrial respiratory chain, and mutations in PNPT1 can lead to mitochondrial dysfunction, subsequently causing neuromuscular dysfunction, which affects the peristaltic function of the gastrointestinal tract [66, 67]. The functions of long noncoding RNA (lncRNA) gene LINC02842 (index SNP: rs72664027) and noncoding RNA (ncRNA) gene LOC105369165 (index SNP: rs6742945) remain unclear, but research has suggested that lncRNAs might have a crucial role in the dysfunction of the lower esophageal sphincter (LES) [68], potentially shedding light on the onset of GERD. Additional research is required to offer more detailed functional annotation of these shared loci.
In addition to detecting shared loci, we also explored whether the cholelithiasis–GERD association can be mediated by shared risk genes through TWAS and SMR analysis. In general, we identified 3 putatively functional genes shared between cholelithiasis and GERD, including SUN2, CBY1, and JOSD1, overexpression of which was negatively associated with the risk of cholelithiasis and GERD in the esophagus-related tissues. Prior research has reported the negative effect of CBY1 and SUN2 genes on tumorigenesis [69–71], which implied a potential role of them in the pathogenesis of gallstone disease and GERD, given that these 2 diseases are risk factors for gallbladder and esophageal cancer, respectively [72, 73]. Furthermore, existing studies suggested the involvement of bile acids in GERD progression through the activation of the Wnt/β-catenin pathway [74]. CBY1 might be involved in the linkage between gallstone disease and GERD, as it can inhibit the Wnt/β-catenin pathway [75], which was enriched according to the results of the pathway enrichment analyses. JOSD1 is a deubiquitinating enzyme, playing a pivotal role in many cellular biological processes [76]. Our findings imply that JOSD1 may play a significant role in the associative mechanisms between cholelithiasis and GERD via the deubiquitination processes. In general, our study offers novel insights into the underlying shared genetic basis of cholelithiasis and GERD, and additional research is required for a more profound elucidation.
Strengths and Limitations
In our study, we conducted the largest prospective study assessing the phenotypic association between cholelithiasis and incident GERD. Besides, we performed a series of sensitive analyses and further applied validation datasets in MR estimates to enhance the robustness of our results. Furthermore, genetic correlation, pleiotropic loci, and gene detection were fully analyzed by 2 different approaches. The convergent evidence acquired through these dual approaches reinforces the reliability of our findings. However, several limitations need to be acknowledged. First, the causal relationship from GERD to cholelithiasis was not significant in all sensitivity analyses, which may be attributed to the limitations of GWAS statistics. Therefore, larger and more powerful GWAS data for cholelithiasis and GERD will be needed to establish the causal relationships from GERD to cholelithiasis. Second, all the data used in this study came from European ancestry populations, which limited the extension of our findings to other ethnic populations; thus, future studies involving a broader range of ancestries are warranted. Third, due to limited GWAS data availability at the time of conducting the analysis, we were unable to perform a deeper subgroup analysis based on the stratification information, such as age, gender, and severity of the disease.
Conclusion
In summary, we found a bidirectional association between cholelithiasis and GERD, which may be attributed to a bidirectional causal relationship and a shared genetic basis, including the significant genetic correlation, novel shared loci, and genes. Our findings provided new insights into the biological mechanisms for cholelithiasis and GERD and suggested promising therapeutic targets, which might provide an innovative research direction for future therapeutic strategy and risk prediction.
Supplementary Material
giaf023_Supplemental_Files
giaf023_GIGA-D-24-00123_Original_Submission
giaf023_GIGA-D-24-00123_Revision_1
giaf023_Response_to_Reviewer_Comments_Original_Submission
giaf023_Reviewer_1_Report_Original_SubmissionJian Zeng -- 7/9/2024
giaf023_Reviewer_1_Report_Revision_1Jian Zeng -- 12/15/2024
giaf023_Reviewer_2_Report_Original_SubmissionMangala Hegde -- 8/12/2024
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lammert F, Gurusamy K, Ko CW, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024. 10.1038/nrdp.2016.24.27121416 · doi ↗ · pubmed ↗
- 2Wang F, Wang J, Li Y, et al. Gallstone disease and type 2 diabetes risk: a Mendelian randomization study. Hepatology. 2019;70(2):610–20. 10.1002/hep.30403.30515881 · doi ↗ · pubmed ↗
- 3Katsika D, Grjibovski A, Einarsson C, et al. Genetic and environmental influences on symptomatic gallstone disease: a Swedish study of 43,141 twin pairs. Hepatology. 2005;41(5):1138–43. 10.1002/hep.20654.15747383 · doi ↗ · pubmed ↗
- 4Di Ciaula A, Molina-Molina E, Bonfrate L, et al. Gastrointestinal defects in gallstone and cholecystectomized patients. Eur J Clin Invest. 2019;49(3):e 13066. 10.1111/eci.13066.30592298 PMC 8118136 · doi ↗ · pubmed ↗
- 5Richter JE, Rubenstein JH. Presentation and epidemiology of gastroesophageal reflux disease. Gastroenterology. 2018;154(2):267–76. 10.1053/j.gastro.2017.07.045.28780072 PMC 5797499 · doi ↗ · pubmed ↗
- 6Maret-Ouda J, Markar SR, Lagergren J. Gastroesophageal reflux disease. JAMA. 2020;324(24):2565. 10.1001/jama.2020.21573.33351044 · doi ↗ · pubmed ↗
- 7Katzka DA, Kahrilas PJ. Advances in the diagnosis and management of gastroesophageal reflux disease. BMJ. 2020;371:m 3786. 10.1136/bmj.m 3786.33229333 · doi ↗ · pubmed ↗
- 8Portincasa P, Di Ciaula A, Palmieri V, et al. Impaired gallbladder and gastric motility and pathological gastro-oesophageal reflux in gallstone patients. Eur J Clin Invest. 1997;27(8):653–61. 10.1046/j.1365-2362.1997.1600709.x.9279528 · doi ↗ · pubmed ↗