Continuous Non-Invasive Hemodynamic Monitoring in Cirrhotic Patients—Friend or Foe?
Mirela Crihan, Alexandru Leonard Alexa, Dan Valean, Daniela Ionescu

TL;DR
This study compares non-invasive and minimally invasive methods for monitoring blood flow in cirrhotic patients, finding mixed accuracy and potential for non-invasive tools in specific cases.
Contribution
The study evaluates non-invasive hemodynamic monitoring accuracy in decompensated cirrhosis patients, highlighting its limitations and potential for fluid responsiveness assessment.
Findings
ClearSight showed significant discrepancies compared to FloTrac for CO, CI, and MAP measurements.
SVV measurements were consistent between the two methods, indicating similar fluid responsiveness assessment.
ClearSight is less accurate than FloTrac but may still be useful for specific monitoring needs in high-risk patients.
Abstract
Background and Objectives: Liver cirrhosis leads to significant hemodynamic changes, particularly portal hypertension and a hyperdynamic circulatory state. Traditional invasive methods for hemodynamic monitoring, while accurate, carry risks such as infection and hemorrhage in a patient predisposed to these conditions. This study evaluates the accuracy of non-invasive continuous hemodynamic monitoring compared to a minimally invasive method in patients with decompensated liver cirrhosis. Materials and Materials and Methods: The study enrolled 51 patients with decompensated liver cirrhosis requiring continuous hemodynamic monitoring in the ICU. Patients underwent simultaneous monitoring via the minimally invasive FloTrac system and continuous non-invasive ClearSight sensor over 24 h, with measurements registered at 6 h intervals. Hemodynamic parameters measured included cardiac output…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
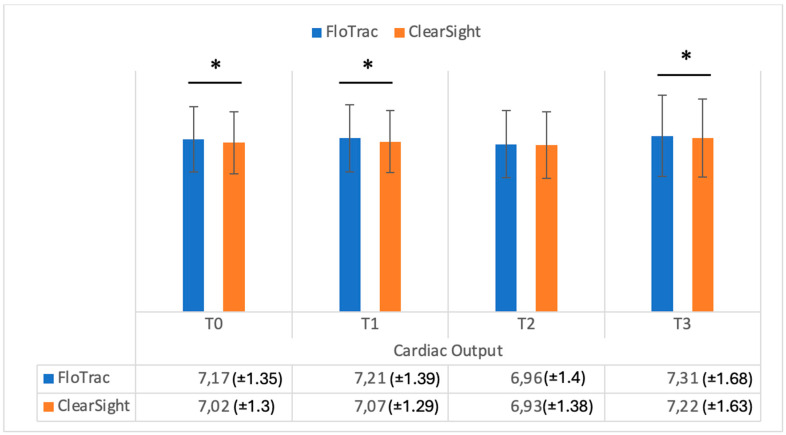 Figure 1
Figure 1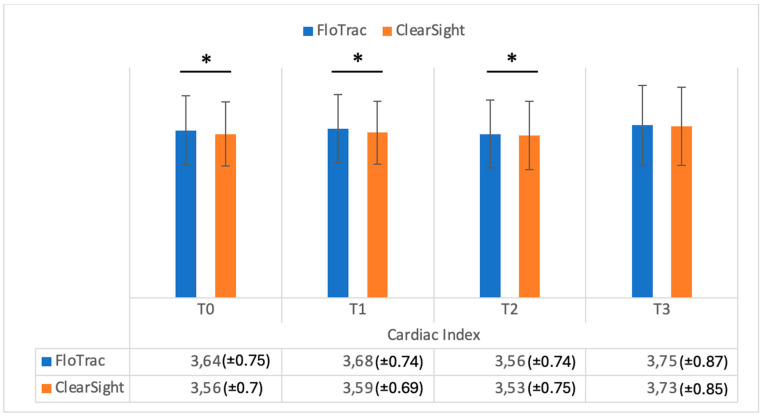 Figure 2
Figure 2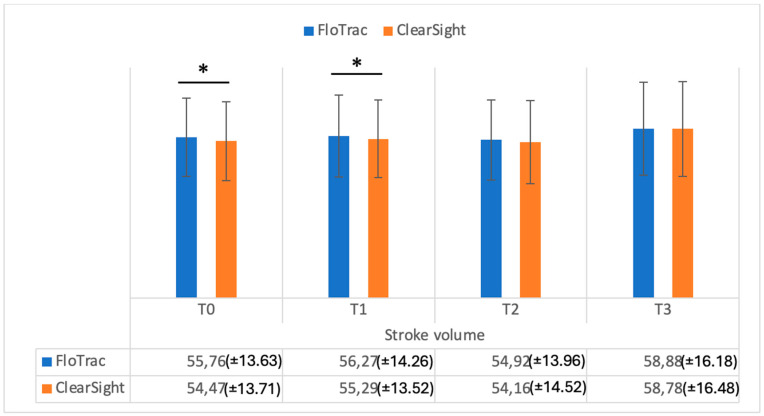 Figure 3
Figure 3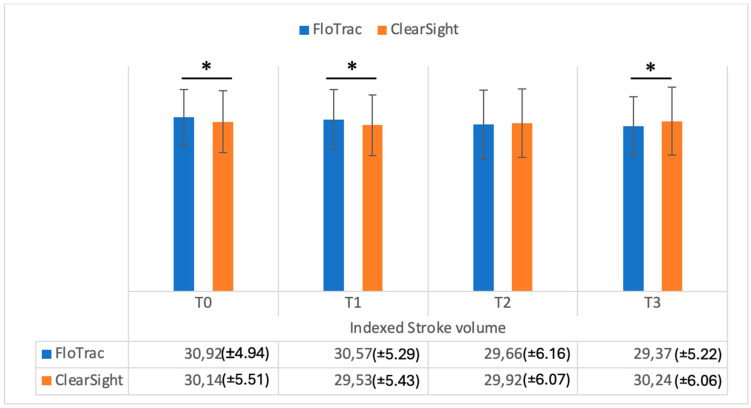 Figure 4
Figure 4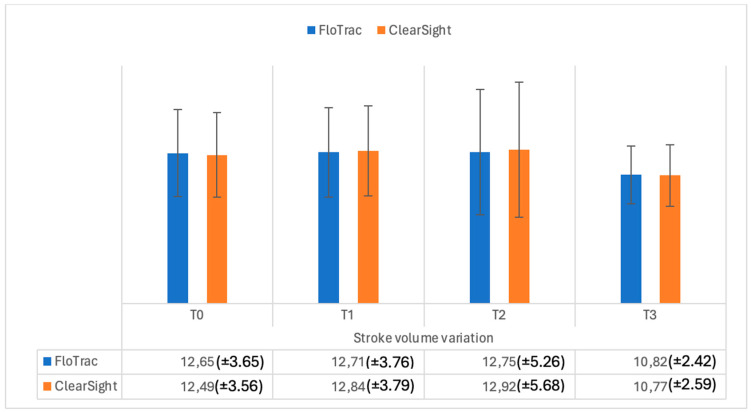 Figure 5
Figure 5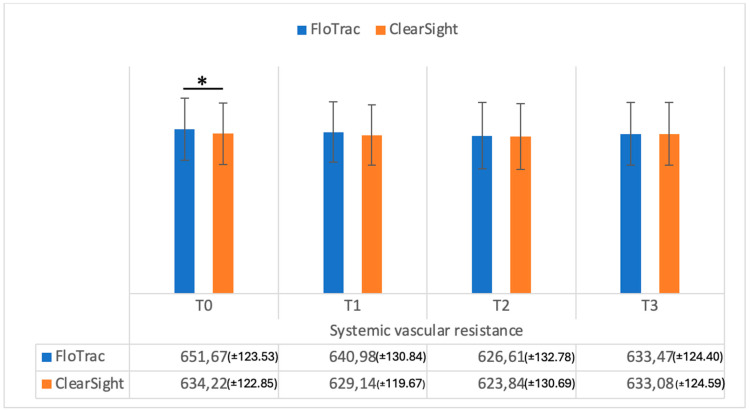 Figure 6
Figure 6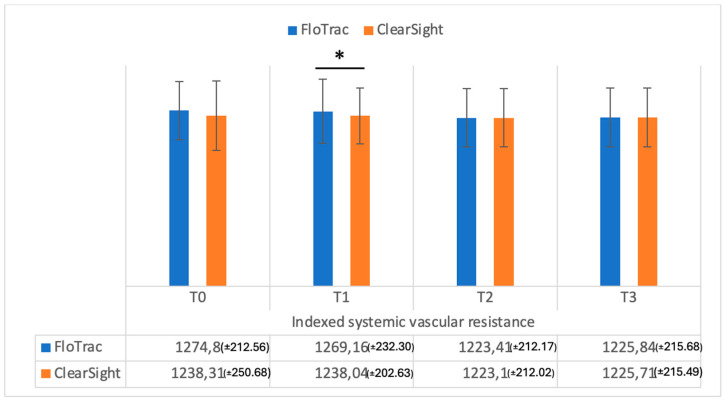 Figure 7
Figure 7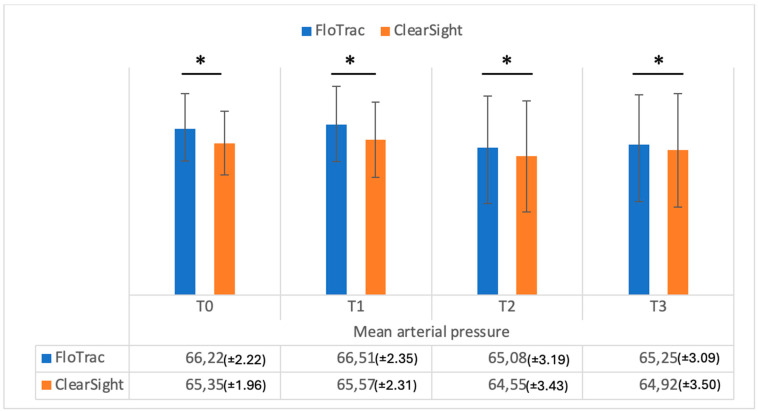 Figure 8
Figure 8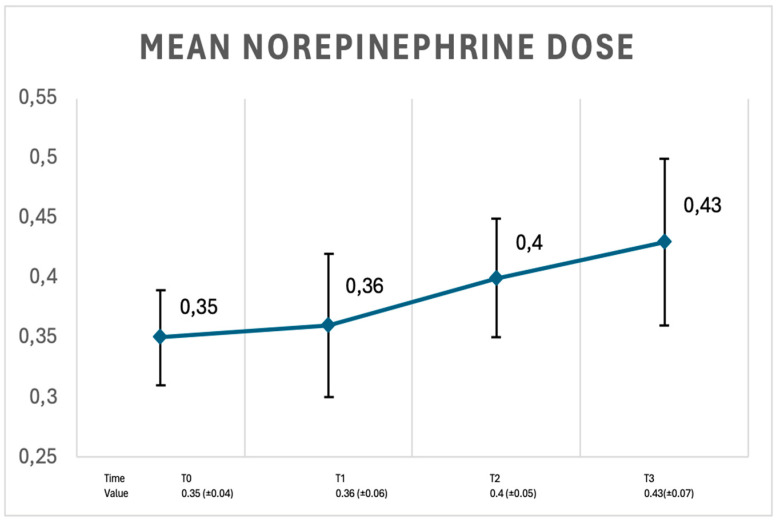 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemodynamic Monitoring and Therapy · Non-Invasive Vital Sign Monitoring · Liver Disease and Transplantation
1. Introduction
Liver cirrhosis induces profound hemodynamic alterations, primarily manifested by increased portal venous pressure (portal hypertension) due to fibrotic changes within the liver [1]. This results in a hyperdynamic circulatory state characterized by elevated cardiac output and decreased systemic vascular resistance and the portal level contributes to complications such as variceal hemorrhage and ascites [1,2,3]. These hemodynamic changes become more pronounced as cirrhosis and portal hypertension progress, and the severity of the hyperdynamic state is directly associated with the risk of developing complications such as variceal bleeding and ascites. Furthermore, the degree of hyperdynamic circulation is a significant predictor of patient outcomes, including overall survival in those with advanced liver disease [3,4].
In the management of decompensated cirrhosis, hemodynamic monitoring is an essential element. In recent years, there has been rapid development in continuous non-invasive hemodynamic monitoring technologies [5]. Patients with advanced cirrhosis often present with hyperdynamic circulation characterized by a decrease in systolic and diastolic blood pressure, and an increase in heart rate and cardiac output (CO) [5,6,7]. Even though they are often described as the gold standard, the invasive methods are relatively complex procedures (depending on the type of catheter) and have certain periprocedural risks like infection, local hemorrhage (in patients with coagulation disturbances), or thrombosis [6,7].
The ClearSight (Edwards Lifesciences— Irvine, CA, USA) system allows for continuous monitoring of hemodynamic parameters through a non-invasive finger cuff. Continuous data offered by the ClearSight system enables proactive optimization of perfusion through hemodynamic management [8]. This system uses a cuff applied on a finger of the patient and is a method of measuring arterial pressure and hemodynamic parameters (CO, SV, SVV, etc.) using a disposable pneumatic cuff [8] called the “volume clamping” method described by Jan Penaz [9]. After 8 h of continuous monitoring on the same finger, the cuff should be switched to another finger. The total measurement time shall not exceed 72 h of continuous monitoring [9,10].
In our study, we aimed to investigate if this monitoring is comparable to minimally invasive monitoring in decompensated cirrhotic patients, taking into consideration coagulation disturbances due to liver dysfunction with consecutive hemorrhage and the risk of catheter infection [8,9].
The main objective was to assess the accuracy and reliability of this continuous non-invasive method for measuring key hemodynamic parameters, such as CO, SV, SVV, SVR, CI, SVI, SVRI, and mean arterial pressure, in comparison to the minimally invasive method.
2. Materials and Methods
This study was approved by the Ethics Committee of the “Iuliu Haţieganu” University of Medicine and Pharmacy Cluj-Napoca (approval no. 94/20 June 2023) and by the Ethics Committee of the Regional Institute of Gastroenterology and Hepatology “Prof. Dr. Octavian Fodor” Cluj-Napoca (approval no. 1652/2 February 2024).
After written informed consent was obtained from each patient (or relatives in case of severe hepatic encephalopathy), the study enrolled 51 patients between January 2023 and September 2024 with decompensated liver cirrhosis admitted to the ICU who required continuous hemodynamic monitoring, vasoactive support, and mechanical ventilation. Data collection was handled in compliance with the Declaration of Helsinki.
Inclusion criteria for patients were a diagnosis of decompensated liver cirrhosis (bacterial or viral sepsis, hemorrhage) requiring continuous hemodynamic monitoring; aged 18–80 years; ASA risk II–III.
Exclusion criteria for this study included: refusal to participate; age < 18 years or > 80 years, patients with documented cardiac arrhythmias; patients with severe coagulopathies contraindicating arterial catheter placement during the study timeframe; and patients with severe peripheral vasoconstriction (determined via doppler ultrasound screening). Repeated compared measurements of hemodynamic parameters registered comparatively were taken at 6 h intervals during continuous patient monitoring for 24 h with minimally invasive techniques (FloTrac with HemoSphere monitor—Irvine, CA 92614, USA) and continuous monitoring of hemodynamic parameters via non-invasive techniques.
2.1. Minimally Invasive Monitoring
Eligible patients underwent insertion of an arterial catheter into the radial artery using the Seldinger technique. Catheterization was performed under local anesthesia, and the correct catheter position was confirmed by ultrasonography. The hemodynamic parameters (cardiac output [CO], cardiac index [CI], stroke volume [SV], stroke volume indexed [SVI], stroke volume indexed [SVI], stroke volume variable [SVV], systemic vascular resistance [SVR], systemic vascular resistance indexed [SVRI], and mean arterial pressure [MAP]) were measured continuously for 24 h and registered at 6 h intervals. The first measurement (T0) was done at 6 h after admission. This time interval was necessary for patient admission, catheter insertion, fluid administration, as well as noradrenaline infusion set-up.
2.2. Continuous Non-Invasive Monitoring
Continuous non-invasive hemodynamic monitoring was performed using a ClearSight sensor. This non-invasive technique preserves tissue integrity, offering advantages such as operational simplicity and reduced risk of catheter bleeding or infection. A disposable pneumatic cuff was applied to a finger (the middle finger) of each patient, continuously inflating and deflating in accordance with the volume clamping method previously discussed. The ClearSight system utilizes a self-calibration algorithm that periodically recalibrates the measurements using a cardiac reference system to account for the vertical displacement between the finger cuff and the heart [11,12]. Hemodynamic parameters were registered comparatively at 6 h time intervals for 24 h. Each study patient had a total of 4 comparative measurements of hemodynamic monitoring (T0, T1, T2, T4).
2.3. Statistics
Data collection was handled in compliance with EU General Data Protection Regulation legislation 2016/679 on the protection of individuals with regard to the processing of personal data.
The data were checked for normal distribution and comparisons of the mean values using t-tests for independent variables were performed. Based on the comparative cardiac output measurements of the first 5 patients, we calculated that a sample size of 44 patients would be necessary to attain a study power of 90%. We enrolled 51 patients to cover eventual dropouts.
The statistical analysis of the data was performed using IBM SPSS v26.0. Comparisons of the mean values between two variables were performed using a t-test. Comparisons of the mean between three or more variables were performed using ANOVA. A p < 0.05 was considered statistically significant.
3. Results
A final roster of 51 patients were enrolled in and completed the study. The demographic and clinical data of the study group are shown in Table 1.
The biochemical laboratory parameters and clinical score data are shown in Table 2.
The comparative time interval measurements (T0, T1, T2, T3) and hemodynamic values of the study group population (n = 51) are shown in Table 3.
Figure 1 shows the data registered on cardiac output in the study groups, while Figure 2 shows the cardiac index in the study groups. As can be seen in Figure 1, cardiac output values were significantly different when measured comparatively (FloTrac vs. ClearSight — Irvine, CA, USA) at T0, T1, and T3 (p = 0.001, p = 0.002, p = 0.002). Cardiac index (CI) values were also significantly different between methods at T0, T1, and T2 (p = 0.001, p = 0.001, p = 0.03) (Figure 2). Regarding stroke volume (SV), as can be seen in Figure 3, significantly different values were registered at T0 and T1 (p = 0.001, p = 0.002), while indexed stroke volume (SVI) had significant differences at T0, T1, and T3, as seen in Figure 4 (p = 0.001, p = 0.001, p = 0.02).
Stroke volume variation (SVV) did not differ at any time interval (Figure 5) between FloTrac and ClearSight — Irvine, CA, USA (p = 0.29; p = 0.41; p = 0.36; p = 0.69, respectively).
Systemic vascular resistance (SVR) values were significantly different (p = 0.001) between the methods at T0 (Figure 6), while indexed systemic vascular resistance (SVRI) was significantly different only at T1 (p = 0.01), as shown in Figure 7, and did not differ at the other time intervals.
Mean arterial pressure (MAP) values (FloTrac vs. ClearSight — Irvine, CA, USA) were significantly different at all intervals, as can be seen in Figure 8 (T0—p = 0.001; T1—p = 0.001; T2—p = 0.001; T3—p = 0.01, respectively). It can also be seen that MAP as measured by FloTrac had higher values as compared with ClearSight at any time interval.
The noradrenaline (norepinephrine) dose in the study group was recorded at every 6 h interval and varied, as shown in Figure 9.
4. Discussion
In our study, the hemodynamic parameters CO, CI, SV, SVV, SVI, SVR, SVRI, and MAP, were measured comparatively by two methods, minimally invasive and continuous non-invasive monitoring (FloTrac and ClearSight sensor), in decompensated cirrhotic patients. The ClearSight sensor measurements were statistically significantly different for most parameters, except for stroke volume variation (SVV), where there were no significant differences at any time interval. Most of discrepancies were registered at T0, T1, and T3.
Patients with decompensated liver cirrhosis have characteristic hemodynamic changes, such as systemic vasodilation and hyperdynamic circulation, initially increased cardiac output (CO) and cardiac index (CI), as well as decreased peripheral vascular resistance [13].
These hemodynamic characteristics may complicate hemodynamic measurements, as the FloTrac and ClearSight algorithms may be influenced by decreased blood volume and vascular tone [14]. For example, marked vasodilatation and decreased peripheral vascular resistance may lead to discrepancies in the comparative measurement of parameters such as SVR and MAP, especially in times of severe decompensation or after vasoactive drug administration [15].
There are relatively few studies on comparative measurements of hemodynamic parameters between minimally invasive and continuous non-invasive methods. Most of the studies were done perioperatively. Thus, Cho et al. found that ClearSight did not provide clinically acceptable interchangeability for cardiac output (CO) and systemic vascular resistance (SVR) compared to traditional invasive methods like pulmonary artery catheterization (PAC) during liver transplantation [7]. This was likely due to the hyperdynamic circulation and low SVR characteristic of cirrhotic patients, which made ClearSight less reliable, particularly during rapid hemodynamic changes caused by bleeding or drug administration [7]. However, in contrast with our results, for parameters like mean arterial pressure (MAP), ClearSight showed acceptable accuracy, making it potentially useful for certain non-invasive monitoring situations [7,16].
Hemodynamic assessment in patients with cirrhosis is essential for appropriate fluid and vasopressor management [17]. Measures such as cardiac output (CO), stroke volume (SV), and systemic vascular resistance (SVR) play a critical role in monitoring these patients, but non-invasive ClearSight technologies may have limitations in patients with marked vasodilation [18]. Sumiyoshi et al. highlighted the limitations of the ClearSight system in accurately measuring hemodynamic parameters, particularly in patients undergoing abdominal aortic aneurysm (AAA) surgery [19]. The primary objective of their study was to demonstrate the system’s inability to provide reliable cardiac index (CI) and systemic vascular resistance index (SVRI) measurements during significant hemodynamic changes induced by the surgical process, such as aortic clamping and declamping [19,20].
The ClearSight sensor is a widely used technology for hemodynamic monitoring, but its accuracy can be compromised under extreme conditions, such as hypotension with vasoactive medication or severe vasodilation, commonly seen in decompensated cirrhosis [21,22].
On the other hand, Lee’s study demonstrated that the non-invasive ClearSight method showed a statistically significant correlation with the traditional invasive monitoring method during single-lung thoracic surgery. Although systolic and diastolic blood pressures showed some discrepancies, they were close to acceptable levels compared to the invasive method [23].
There are several potential explanations for our findings compared to the studies mentioned above. Ascites and fluid retention are important characteristics in decompensated cirrhosis and may affect stroke volume (SV) and stroke volume index (SVI) measurements [24,25]. These factors may lead to overestimation or underestimation of the patient’s real hemodynamic status [24,25].
In our study, due to the fact that there were no significant differences in SVV measurements between FloTrac and ClearSight respectively, may indicate that the ClearSight sensor could be used to measure fluid responsiveness or fluid status with results comparable to the gold standard of invasive monitoring.
This may be attributed to several factors, including the patient’s volemic status and the characteristics of the calculation methods used by both technologies [26]. Patients with decompensated cirrhosis share similar pathophysiological characteristics with chronic heart failure [26]. Factors such as chronic vasodilation and mechanically controlled ventilation may also reduce normal SVV, making the measurements similar between devices [26,27]. In comparison to these results, Wang et al.’s study compared non-invasive ClearSight measurements with invasive Swan–Ganz catheter measurements in cardiac surgery patients and found that ClearSight provides accurate and reliable hemodynamic data, including stroke volume variation (SVV), comparable to traditional invasive methods [26].
The results of our study regarding fluid responsiveness monitoring are consistent with the established standards of good medical practice. The European Society of Intensive Care Medicine recommends the non-invasive option for hemodynamic monitoring and the initial assessment of the patient’s response to fluid therapy (fluid responsiveness) [27]. However, it may not be sufficient for the continuous evaluation of a critically ill patient [27]. For continuous, reliable monitoring and precise hemodynamic management, especially in cases where patients do not respond to fluid therapy and their hemodynamic instability deepens, minimally invasive techniques are recommended [28,29].
Recent data reinforces that the ClearSight sensor is an alternative, particularly in scenarios where invasive monitoring is not ideal or feasible [30,31]. In patients with decompensated cirrhosis, in which hemodynamic parameters are severely impaired, non-invasive monitoring can help to rapidly adjust vasopressors. However, in conditions where vasoconstriction induced by vasopressors affects the measurements, physicians should be cautious and supplement monitoring with additional invasive hemodynamic monitoring methods if the results are uncertain [21,26,30,31].
To our knowledge, this is the first study to evaluate two hemodynamic monitoring approaches: continuous non-invasive and invasive techniques. In cirrhotic patients, our main objective was to assess the accuracy and reliability of non-invasive methods in measuring key hemodynamic parameters, such as CO, SV, SVV, SVR, CI, SVI, SVRI, and mean arterial pressure, in comparison to invasive methods.
However, our study has some limitations. First is the small size of the study group, thus comparable with other similar studies published in the literature. We also did not corelate the magnitude of discrepancies in measurements with noradrenaline dose or the amount of fluids administered to study group patients.
5. Conclusions
Our study showed no significant difference in measuring SVV between continuous non-invasive and minimally invasive methods, while significant discrepancies were observed when comparing minimally invasive with non-invasive monitoring for cardiac output (CO), cardiac index (CI), and mean arterial pressure (MAP), in patients with decompensated cirrhosis. Further studies on large groups of patients are needed to quantify the role of continuous non-invasive methods.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giuseppetti G.M. Argalia G. Abbattista T. Liver cirrhosis: Evaluation of haemodynamic changes using an ultrasound contrast agent Eur. J. Radiol.200451273310.1016/S 0720-048X(03)00212-215186881 · doi ↗ · pubmed ↗
- 2Brittain J.M. Busk T.M. Møller S. Validation of non-invasive haemodynamic methods in patients with liver disease: The Finometer and the Task Force Monitor Clin. Physiol. Funct. Imaging 20183838438910.1111/cpf.1242528402021 · doi ↗ · pubmed ↗
- 3Han S. Park J. Hong S.H. Park C.S. Choi J. Chae M.S. Cardiovascular manifestation of end-stage liver disease and perioperative echocardiography for liver transplantation: Anesthesiologist’s view Anesth. Pain. Med.20221713214410.17085/apm.2213235538654 PMC 9091670 · doi ↗ · pubmed ↗
- 4Ma Z. Lee S.S. Cirrhotic cardiomyopathy: Getting to the heart of the matter Hepatology 19962445145910.1002/hep.5102402268690419 · doi ↗ · pubmed ↗
- 5Iwakiri Y. Groszmann R.J. The hyperdynamic circulation of chronic liver diseases: From the patient to the molecule Hepatology 200643 S 121S 13110.1002/hep.2099316447289 · doi ↗ · pubmed ↗
- 6Frank P. Logemann F. Gras C. Palmaers T. Noninvasive continuous arterial pressure monitoring during anesthesia induction in patients undergoing cardiac surgery Ann. Card. Anaesth.20212428128710.4103/aca.ACA_120_2034269255 PMC 8404578 · doi ↗ · pubmed ↗
- 7Cho H.Y. Lee H.J. Hwang I.E. Lee H.C. Kim W.H. Yang S.M. Comparison of invasive and non-invasive measurements of cardiac index and systemic vascular resistance in living-donor liver transplantation: A prospective, observational study BMC Anesthesiol.20232335910.1186/s 12871-023-02302-x 37924013 PMC 10625262 · doi ↗ · pubmed ↗
- 8Truijen J. van Lieshout J.J. Wesselink W.A. Westerhof B.E. Noninvasive continuous hemodynamic monitoring J. Clin. Monit. Comput.20122626727810.1007/s 10877-012-9375-822695821 PMC 3391359 · doi ↗ · pubmed ↗