Ki-67 as a Prognostic Marker in Squamous Cell Carcinomas of the Vulva: A Systematic Review
Gilbert Georg Klamminger, Elke Eltze, Annick Bitterlich, Yaman Degirmenci, Annette Hasenburg, Mathias Wagner, Meletios P. Nigdelis

TL;DR
This paper reviews studies on whether Ki-67 staining can predict outcomes in vulvar squamous cell carcinoma, finding mixed results for survival and no clear link to lymph node spread.
Contribution
The study systematically evaluates Ki-67's role as a prognostic marker in vulvar cancer, highlighting methodological differences in staining interpretation.
Findings
Most studies found no significant link between Ki-67 and lymph node involvement.
Some studies showed Ki-67 was associated with overall survival, especially with pattern-based staining.
Results on Ki-67's prognostic value for survival were inconsistent across studies.
Abstract
Background/Objectives: To evaluate the prognostic impact of immunohistochemical ki-67 staining analysis regarding lymph node involvement and survival data (overall/progression-free survival) in squamous cell carcinoma of the vulva. Methods: A systematic literature search of English and German articles was conducted (PubMed, Embase, Scopus, Web of Science) from 1980 to December 2023, including the search terms “vulvar Neoplasms”, “vulvar cancer”, “vulvar carcinoma”, “vulvar tumor”, ”vulvar tumour”, “vulvar malignancy”, “vulvar malignant”, “ki-67”, “MIB-1”, “MIB1”, “proliferative index”, “proliferative activity”, “mitotic index”, and “mitotic count”. Study quality was assessed using a two-step “mixed-criteria” approach; to synthesize study results, a narrative summary is provided. Results: In total, 13 studies were included in this systematic literature review. In general, two distinct…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
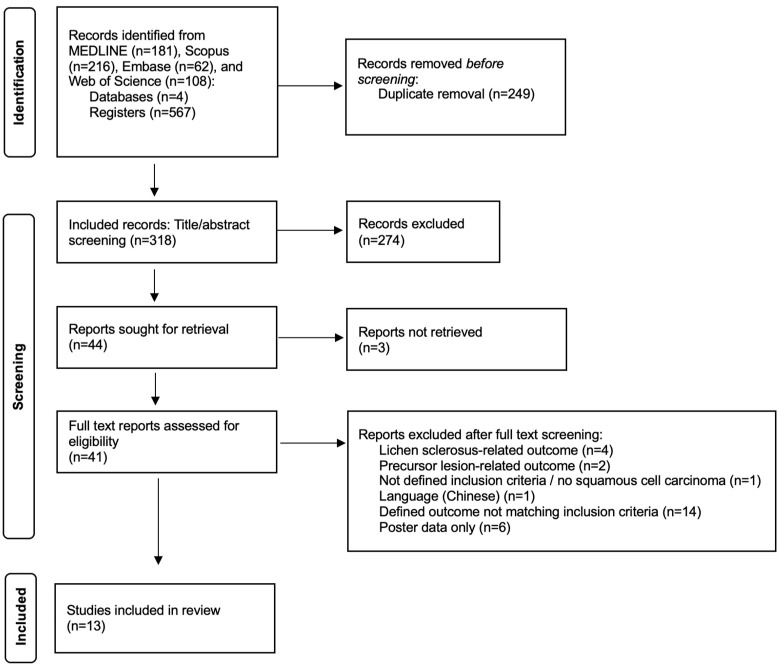 Figure 1
Figure 1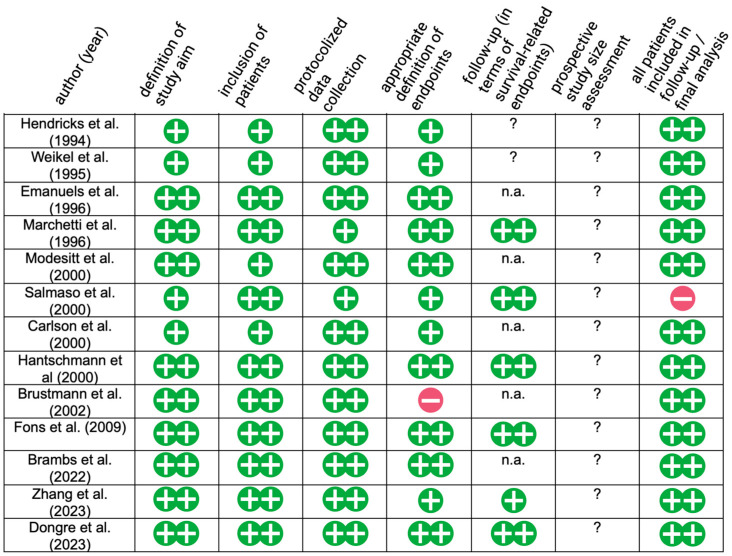 Figure 2
Figure 2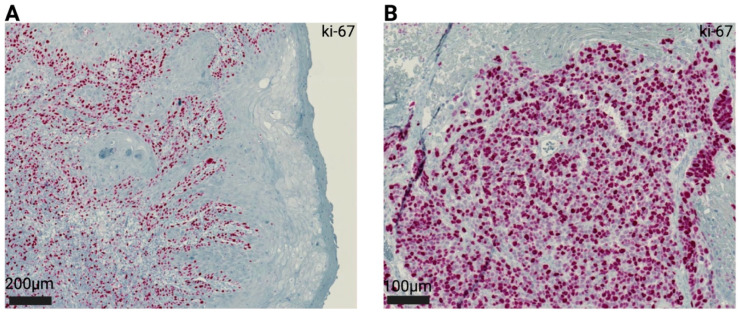 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Colorectal and Anal Carcinomas · Nonmelanoma Skin Cancer Studies
1. Introduction
Since the ki-67 antibody was first described in 1983, its ability to estimate the proportion of cell growth has already proven to be particularly valuable in histopathological tumor diagnostics [1]. Labeling proliferative cells targeting the ki-67 (MKI67) nuclear protein, which is encoded by the MKI67 gene and exclusively expressed in cells that are in a cell cycle state outside of G0, it is feasible not only to determine the character of a neoplasia (benign/malignant), but also to determine the degree of differentiation (grading) in various tumor entities [2,3,4,5,6]. For example, the histopathological evaluation of the ki-67 proliferation index is integrated within the grading system of gastroenteropancreatic neuroendocrine neoplasms [7]. Particularly noteworthy is also the fact that ki-67 staining is related to overall survival in breast cancer patients and that several clinical applications are integrated within the standard routine: On the one hand, ki-67 is used to define the intrinsic subtype (luminal A / luminal B tumors) of breast cancer; on the other hand, it can be used (together with other parameters) for risk assessment and identification of patients who benefit from chemotherapeutical treatment in addition to endocrine therapy. More recently, its ability as a dynamic biomarker (following repeated measurements on both the biopsy material and the surgical specimen during short-term neoadjuvant endocrine therapy) has been described [8,9]. To date, joined efforts tackling interlaboratory inconsistencies aiming for standardized interpretation, as well as scoring of immunohistochemical data, culminated in the International ki-67 in Breast Cancer Working Group [10].
In addition to established risk factors (e.g., lymph node metastases) within HPV-associated/independent squamous cell carcinoma of the vulva, clinicopathological parameters of uncertain prognostic relevance, such as ulceration and perineural sheath infiltration, remain [11,12,13]. To date, neither the mode of immunohistochemical ki-67 detection (either analysis of different expression patterns or numeric quantity of positive cells) nor the prognostic associations with overall/progression-free survival or lymph node metastasis in vulvar cancer has been translated into clinical practice.
For this study, medical libraries were systematically screened for literature regarding ki-67 staining in vulvar cancers, and relevant study results were depicted to examine and summarize existing knowledge about the prognostic relevance of ki-67 immunohistochemistry with regard to lymph node metastasis and survival data in squamous cell carcinoma of the vulva.
2. Materials and Methods
This systematic review was conducted in line with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) using an a priori established protocol outlining methodological data screening and data collection [14]; institutional review board approval was waived, since only published studies were reviewed. For an additional overview, PICO questions to be answered by this systematic review are listed and summarized within the Supplementary Materials [15,16].
2.1. Systematic Search Strategy
The (bibliographic) databases MEDLINE, Scopus, Embase, and Web of Science were searched to identify reports of interest published between 1980 and 2023 (time of last consultation: December 2023), employing the search terms: “vulvar Neoplasms”, “vulvar cancer”, “vulvar carcinoma”, “vulvar tumor”, ”vulvar tumour”, “vulvar malignancy”, “vulvar malignant”, “ki-67”, “MIB-1”, “MIB1”, “proliferative index”, “proliferative activity”, “mitotic index”, and “mitotic count”, using the Boolean AND/OR operators. See Supplementary Table S1 for the individual search strategies and search terms listed for each database.
2.2. Inclusion and Exclusion Criteria
Studies applying the ki-67 antibody on HPV-associated/independent squamous cell carcinoma of the vulva were included (inclusion criteria); all studies not meeting the inclusion criteria, or which applied the antibody of interest on other tumor entities of the vulva, precursor lesions, inflammatory/autoimmune conditions such as lichen sclerosus, as well as articles in languages other than English or German and conference posters without publicity available data were excluded (exclusion criteria).
2.3. Outcomes
As outcome criteria, a reported association of ki-67 immunohistochemistry and the occurrence of lymph node metastasis and/or its association with overall/progression-free survival were defined.
2.4. Study Selection and Data Extraction
Duplicates were removed and title/abstract screening was performed to identify eligible reports via Rayyan© (Rayyan Systems, Inc, Cambridge, MA, USA) [17]. Consecutively, full texts were screened and relevant data (method of ki-67 quantification, outcome parameter of interest, method and result of underlying statistical analysis) was extracted and collected within an internal data sheet (Microsoft Office Word, version 16) by two authors (GGK, MPN).
2.5. Assessment of Study Quality and Risk of Bias
Initial assessment of study quality was employed using a “mixed-criteria” two-step screening approach (study participation, prognostic factor measurement, outcome measurement, analysis) in which eligible studies were screened for relevant quality items; see Supplementary Table S2 [18]. In order to systematically assess the risk of bias in each study, the Methodological Index for Non-Randomized Studies (MINORS) protocol was employed using 7 items: (1) definition of a clear aim, (2) inclusion of patients, (3) protocolized data collection, (4) appropriate definition of endpoints, (5) follow-up (>/< 5 years), (6) prospective study size assessment, and (7) patients included in follow-up/final analysis [19]. In cases of incomplete result presentation, studies were extra highlighted to assess risk of bias due to missing results [20]. Incongruences were resolved by consensus-reaching discussion of the subject by all authors.
2.6. Data Synthesis
To synthesize included studies, a narrative summary (outlining not only quantitative data, but also point/interval estimates if specified), combined with visualization of individual study characteristics, was presented. All data collected underwent no further modification. Given the significant methodological heterogeneity in terms of ki-67 assessment, we refrained from performing a meta-analysis of outcomes.
3. Results
In total, 567 database entries were retrieved, and 249 duplicates were removed. The abstracts of 318 records were screened using our a priori defined inclusion criteria, and 274 records were excluded, after which 44 publications were sought for retrieval and the full texts of 41 publications were assessed for eligibility; thereby, 28 reports were excluded ([21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]) and 13 reports ([49,50,51,52,53,54,55,56,57,58,59,60,61]) were included in this study. See Figure 1 for a flow diagram presenting the study selection. Figure 2 presents the results of bias assessment. Regarding bias, 5 out of 13 studies were at low risk of bias, 6 were at middle risk, while 2 were at high risk. The technical details of the ki-67 staining protocols are depicted in Supplementary Table S3.
3.1. Interpretation of Positive Ki-67 Staining and Its Respective Cut-Off Values
To date, there is no common definition of ki-67 analysis and interpretation in vulvar cancer as a prognostic factor; in general, two approaches were determined. On the one hand, some researchers take a pattern-based approach, categorizing the distribution of ki-67-positive cells within the tumor mass into a distinct subgroup; on the other hand, there exists a subgroup division based on positive cell count in accordance with a defined amount of generally visible (tumor) cells.
Based on initial analysis of ki-67 pattern distributions in bladder cancer, as well as reports employing protease cathepsin-D and pro-cathepsin-L staining within a cohort of vulvar carcinomas, early studies defined two patterns of ki-67 staining on vulva carcinomas: a “localized” distribution of ki-67-positive nuclei restricted to basilar components of tumor clusters and a “diffuse” pattern, with ki-67-positive nuclei spreading universally all over the tumor mass [49,62,63]. Figure 3 shows both types of staining distributions in an exemplary manner. In 2000, Hantschmann et al. further subdivided the localized pattern. The already-defined localized pattern was named “basal type”; in case staining primarily occurs at the tumor invasion front, the pattern was defined as “infiltrative type” [56]. Brambs et al. (2022) [59] then again re-defined three patterns of ki-67 staining based on previous findings in penile squamous cell carcinoma and, in comparison to the physiological vulva epithelium: “Low-grade patterns” in the case of ki-67-positive nuclei were solely based on the outer cell layers of tumor clusters, “intermediate patterns” if ki-67-positive nuclei extended from the infiltrating zone to the tumor centrum, and “high-grade patterns” in the case of diffuse positive intratumoral staining [64].
In contrast, the ki-67 index is defined as the amount of positive stained cells per (total) number of tumor cells or, alternatively, per area [51]. Interpretation is widely based on a dichotomous approach, splitting up the study group in line with a priori defined cut-off values into a “ki-67-high group” and a “ki-67-low group”. In cases for which two subgroups were defined, the cut-off values <25%/>25% (Weikel et al.), as well as <50% / >50% (Zhang et al.), were established [50,60]. Another cut-off value was employed by Fons et al. (2009), who defined three groups according to the immunohistochemical cell count—“negative” in the case that less than 10% of nuclei stain positive, “weak positive” if up to 50% show positive nuclear staining, and “strong positive” if >50% of tumor nuclei are ki-67-positive [58].
Certain approaches employed both aforementioned methods: Marchetti et al. (1996) determined the number of ki-67-positive cells per 2000 tumor cells and also noted the specific staining pattern (diffuse/localized), subgrouping the latter into two distinct clusters (cut-off values: 0.2%–6% positivity / 7–9% positivity) [52]. Hantschmann et al. (2000) differentiated among three staining types (see above), but, moreover, divided their cohort into different proliferative indices (cut-off values: <10%, 11 to 50%, and >50%) by counting ki-67-positive cells per 200 tumor cells [56].
3.2. Association of Ki-67 with Lymph Node Metastasis
In total, ten studies examined the association of immunohistochemical ki-67 assessment with lymph node status; see Table 1 for a detailed realization. Hereby, only one group reported a statistically significant association, namely when analyzing the connotation between ki-67 staining pattern and lymph node metastasis (rho = 0.388, p = 0.0001; Spearman’s Rho and Cox Model) in relation to patient survival data [54], whereas all other studies confirmed no association. Since the interpretation of ki-67 staining varied widely (two patterns / three patterns / cell count), and negative study results were presented unbiased by the study population (variation: between 16 and 145 tumor cases), the observed effect (no correlation) seems to be independent of the analysis method per se.
3.3. Association of Ki-67 with Survival Data
Nine studies evaluated ki-67 as a prognostic marker in relation to overall survival (alternatively: disease-specific survival, with causes of death other than vulvar carcinoma excluded) and/or progression-free survival; refer to Table 2 for a comprehensive overview of study details. Whilst four studies found no statistically significant association of ki-67 with survival data, five studies determined differences in survival times based on ki-67 analysis. Although these mentioned studies all postulate a distinct connotation, with overall survival as their endpoint (only defined endpoint in terms of survival data of Marchetti et al. and Salmaso et al. [52,54]), an association with disease-free survival (progression-free survival) was not statistically significantly proven by Hantschmann et al. (p = 0.076), whereas it was, in contrast, statistically significant in the research by the groups of Dongre et al. (univariate analysis, p = 0.004) and Zhang et al. (p = 0.042, HR: 3.680) [56,60,61]. Regarding the mode of ki-67 analysis, only one of four studies employing the pattern-based approach determined no significant association between ki-67 analysis and survival data, whereas all three other studies did; percentage labeling of ki-67-positive nuclei or establishment of a proliferative index based on cell count (five studies in total) only proved successful in one study [61].
4. Discussion
Despite the tremendous progress in modern pathology—aiming for both precise, biologically determined tumor diagnostics, as well as a preferably unbiased and observer-independent approaches to tissue diagnostics—certain advantages result from continuously testing and reviewing standard and routine laboratory methods and markers such as ki-67. Due to their widespread use in clinical day-to-day practice, they hold potential in being a cheap, fast, and easily applicable tools, allowing for risk stratification in a global diagnostic setting, even though scientific discussions about the choice of the preferred antibody and threshold values in the evaluation of positive cells are still ongoing [65,66].
Within squamous cell carcinomas of the vulva, there is no established standard for the interpretation of proliferation-based immunohistochemical staining results. So far, each research team defined their own method and parameters of analysis; within our review, we could, in general, determine two semantically different approaches: a pattern-based approach and an analysis based on positive cell count. With regard to our a priori defined outcome parameters of interest, namely lymph node metastasis and survival data, we determined 13 studies meeting our inclusion criteria—as a limitation of our review, three studies ([67,68,69] potentially worthy of inclusion could not be retrieved even after contacting the authors and were thus not considered. We found convincing and broad evidence of a lacking statistically significant correlation—according to nine out of ten studies—between ki-67 staining and lymph node involvement in vulvar cancer. In contrast, the prognostic relevance of ki-67 immunohistochemistry regarding survival data was reported ambivalently in the literature—contradictory study results were published, although the majority of studies (five out of nine) postulated a prognostic impact of ki-67. Interestingly, four of the nine studies used a pattern-based method of analysis, three of which showed an association of ki-67 staining with overall survival, thus providing clear evidence of the preferrable method, aiming at sufficient evaluation of ki-67 immunohistochemistry in terms of prognosis in vulvar cancer. The remaining study, which also employed a pattern-based approach, but did not observe a statistically significant correlation, included the smallest number of participants (17 cases, in comparison to min. 73 patients in the other studies) and was therefore potentially underpowered [49,52]. From a histopathological point of view, a potential association between the degree of tumor cell differentiation and ki-67 distribution could be assumed. Indeed, within the examined study cohort, only the two oldest studies determined no significant correlation of tumor grade with a distinct ki-67 staining pattern (Hendricks et al. (p = 0.545) and Marchetti et al. [49,52]), whereas the remaining groups described an association of well-differentiated tumors with focal / basal staining patterns (Salmaso et al. (Spearman’s Rho = 0.344, p = 0.0001), and Hantschmann et al. (p = 0.024)) and consistently found a correlation of poor tumor differentiation with diffuse ki-67 staining pattern (Modesitt et al. (p = 0.013, CI 1.59 –7.60) [53,54,56]. In alignment, Brambs et al. employed the ki-67 staining pattern itself as a grading tool (low/intermediate/high grade pattern) in 2022 [59].
Within this area of research, our systematic review highlights several structural shortcomings, all of which naturally contribute to its limitations. Although the above-listed retrospective research projects all evaluated the prognostic impact of ki-67 staining in vulvar carcinoma, several studies included a small sample size (for example n = 16 or n = 17) [49,55]. That said, eligible studies show a distinct clinical (e.g., tumor stages included) and technical (e.g., different commercially available ki-67-clones provided by several manufacturers) heterogeneity, which should be carefully considered when interpreting a comparison between them. It is also striking that the studies included show a definite methodological heterogeneity, employing different strategies of statistical data analysis (see Table 1 and Table 2), which not only impacts comparability, but also yields a potential for bias. While some of these methodological differences may be explained by individual methods of data handling and analysis (e.g., interpretation of the type of variable, differences in data distribution within single studies), standardized methods of both data collection—the need for a defined cut-off arises from the diverse and wide range of cut-offs used in the studies reviewed here—and data analysis remain key within future study approaches. Such efforts would usually culminate in the establishment of international working groups that define an a priori standardized research design, aimed at producing reproducible and reliable results in histopathological research.
Finally, we were not able to perform subgroup analysis/interpretation because most of the included studies were performed prior to the current 2020 WHO Classification of Female Genital Tumors and its classification of vulvar cancers based on their HPV-association/HPV-independence [70]. Future studies may even go beyond this and place the search for histological biomarkers in the context of the newly proposed molecular classification of vulvar cancer (HPV+/HPV-p53wildtype/HPV-p53mutant) [71]. Nevertheless, before results can be implemented into clinical routine, confirmation of the postulated evidence in ideally prospective, multicenter (to overcome interlaboratory variability), and regularly powered (to avoid statistical bias and allow further subgroup analysis) studies remains a fundamental necessity.
Breaking new methodological ground, the team of Zhang et al. was able to establish prognostic nomograms by using the parameters of age, HPV status, ki-67 index, PDL-1 analysis, and tumor-infiltrating t-cells. Thereby, the scoring of patients into two distinct groups could be established, proving a high concordance with survival data (overall survival p = 0.049, progression-free survival p = 0.0012) Additionally, future potential methodological improvements include the use of tissue micro arrays or automatic positive cell counts; in that regard, Fons et al. proved the valid use of either tissue micro arrays or full sections / full slide analysis in vulvar cancer ki-67 staining detection, and Choschzick et al. showed that deep convolutional neural network-based analysis was capable of detecting ki-67 indices (low <2%, medium 2–20%, high >20%), setting the base for less time-consuming and reliable data annotation [27,30]. That said, in the era of digital pathology, the implementation of novel tools, including artificial intelligence / machine learning may be not only less time consuming, but also more reproducible, contributing to further standardization of ki-67 interpretation by overcoming the high inter- and intra-observer variability reported, which probably arises due to a local heterogeneity in staining distribution, as well as varying color intensities within larger tumor sections [72]. Despite the aforementioned study by Choschzick et al., other research efforts in this field also aim to detect ki-67 using deep learning models in breast cancer or cervical intraepithelial lesions, or to develop a virtual ki-67-stained slide based solely on regular hematoxylin/eosin staining of squamous cell carcinomas [73,74,75]. Whether ki-67 could also play a contributing role as a distinct variable within a set of parameters used, e.g., in supervised machine learning approaches to calculate predictive probabilities in vulvar cancer, remains to be seen in future studies.
Beyond question, there are additional research interests making use of ki-67 examination in vulvar carcinoma. Thinking outside the box, Okon et al. aimed at addressing tumor heterogeneity; their unsupervised statistical approach using k-means clustering did determine different tumor sub-classes based on, among others, age and p53 expression, but not with statistically significant differences in ki-67-positively stained nuclei [26]. In another approach, ki-67 analysis was proposed to be associated with HPV status [21], and alternative immunohistochemical studies, despite ki-67 application, aim inter alia at p16 and p53, vascular endothelial growth factor, endothelial growth factor, estrogen receptor, HER2/neu, PD-L1 or epithelial–mesenchymal transition marker, and microsatellite marker detection / analysis [24,25,31,76,77,78]. Furthermore, ki-67 staining was evaluated as part of a dual staining approach in an immunocytochemistry study to distinguish between precursor lesions of the vulva and invasive vulvar neoplasia [48]. Two studies aimed at the comparison of ki-67 with alternative proliferative markers/activity; Brustmann et al. looked at nucleolar organizer regions and Topoisomerase II-alpha visualizations and did not determine a significant association of one of these proliferation markers with survival data; meanwhile, Emanuels et al. evaluated the ki-67 cell count, the proliferation marker Ag-NOR, and the mitotic index, but did not find an association of any proliferative markers with inguinofemoral lymph node metastases [51,57]. Whether prognostic impact can be derived from new proliferation markers—such as Phosphorylated Histone H3 (PHH3) staining, precisely solely mitotic cells and thereby holding potential to overcome invariances based on observer-dependent mitotic figure count—remains to be evaluated [79,80].
5. Conclusions
In summary, our systematic review depicts the postulated evidence of ki-67 as a potential prognostic marker in vulvar cancer. Although an association between ki-67 staining and lymph node metastasis could not be convincingly demonstrated, a positive association, in terms of survival data, was found in several studies, especially with the pattern-based analysis approach, despite study inconsistencies, such as different sizes of patient cohorts and varying ki-67 antibody suppliers. Considering the great availability of ki-67-stained vulvar cancers in global pathological archives, due to the method’s ubiquitous routine usage in daily diagnostics, even in low-income countries, additional retrospective analyses / evaluations of already-existing tissue samples seem reasonable in order to achieve more solid evidence of its prognostic impact. Moreover, prospective research efforts evaluating the prognostic connotation of ki-67 staining with survival data could be implemented in a potentially beneficial way with manageable cost and effort, utilizing this commonly employed routine diagnostic marker.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gerdes J. Schwab U. Lemke H. Stein H. Production of a Mouse Monoclonal Antibody Reactive with a Human Nuclear Antigen Associated with Cell Proliferation Int. J. Cancer 198331132010.1002/ijc.29103101046339421 · doi ↗ · pubmed ↗
- 2Scholzen T. Gerdes J. The Ki-67 Protein: From the Known and the Unknown J. Cell Physiol.200018231132210.1002/(SICI)1097-4652(200003)182:3<311::AID-JCP 1>3.0.CO;2-910653597 · doi ↗ · pubmed ↗
- 3Kleer C.G. Giordano T.J. Braun T. Oberman H.A. Pathologic, Immunohistochemical, and Molecular Features of Benign and Malignant Phyllodes Tumors of the Breast Mod. Pathol.20011418519010.1038/modpathol.388028211266524 · doi ↗ · pubmed ↗
- 4Pirog E.C. Quint K.D. Yantiss R.K. P 16/CDKN 2A and Ki-67 Enhance the Detection of Anal Intraepithelial Neoplasia and Condyloma and Correlate with Human Papillomavirus Detection by Polymerase Chain Reaction Am. J. Surg. Pathol.2010341449145510.1097/PAS.0b 013e 3181 f 0f 52a 20871219 · doi ↗ · pubmed ↗
- 5Vang R. Barner R. Wheeler D.T. Strauss B.L. Immunohistochemical Staining for Ki-67 and P 53 Helps Distinguish Endometrial Arias-Stella Reaction from High-Grade Carcinoma, Including Clear Cell Carcinoma Int. J. Gynecol. Pathol.20042322323310.1097/01.pgp.0000130106.13533.3815213598 · doi ↗ · pubmed ↗
- 6Kolles H. Niedermayer I. Schmitt C. Henn W. Feld R. Steudel W.I. Zang K.D. Feiden W. Triple Approach for Diagnosis and Grading of Meningiomas: Histology, Morphometry of Ki-67/Feulgen Stainings, and Cytogenetics Acta Neurochir.199513717418110.1007/BF 021871908789658 · doi ↗ · pubmed ↗
- 7Tao Z. Xue R. Wei Z. Qin L. Bai R. Liu N. Wang J. Wang C. The Assessment of Ki-67 for Prognosis of Gastroenteropancreatic Neuroendocrine Neoplasm Patients: A Systematic Review and Meta-Analysis Transl. Cancer Res.2023121980199110.21037/tcr-23-24837701110 PMC 10493787 · doi ↗ · pubmed ↗
- 8Nahed A.S. Shaimaa M.Y. Ki-67 as a Prognostic Marker According to Breast Cancer Molecular Subtype Cancer Biol. Med.20161349610.20892/j.issn.2095-3941.2016.006628154782 PMC 5250608 · doi ↗ · pubmed ↗