Recreational Use of Nitrous Oxide as a Source of Frostbite Injuries to the Skin: A Review of the Literature and a Case Report
Sebastian Holm, Reza Tabrisi, Johann Zdolsek

TL;DR
This paper reviews how recreational use of nitrous oxide can cause frostbite injuries, especially in young adults, and highlights the need for public awareness.
Contribution
This is the first literature review summarizing frostbite injuries caused by recreational nitrous oxide use.
Findings
Most frostbite injuries from nitrous oxide occur in young adults, predominantly females, and are localized to the inner thighs.
Conservative management is the primary treatment for these injuries, with skin grafting used less frequently.
The incidence of such injuries has increased in recent years, with most cases reported between 2022 and 2024.
Abstract
Nitrous oxide has a wide range of medical applications, such as being used as an analgesic in general anesthesia, dental procedures, childbirth and sedation. Lately, it has also been employed as an inhalant recreational drug to induce brief euphoria. Recent studies indicate a worldwide rise in the incidence of skin frostbites associated with nitrous oxide use. A scoping review was conducted to synthesize and summarize the existing literature published in English regarding frostbite injuries associated with the recreational use of nitrous oxide. The literature search was carried out in July 2024 using databases such as Embase, Web of Science and PubMed®. From an initial pool of 83 publications, 8 studies were ultimately selected for full-text review as they met our inclusion criteria for analysis. Additionally, we provide a representative clinical case involving a 21-year-old male who…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
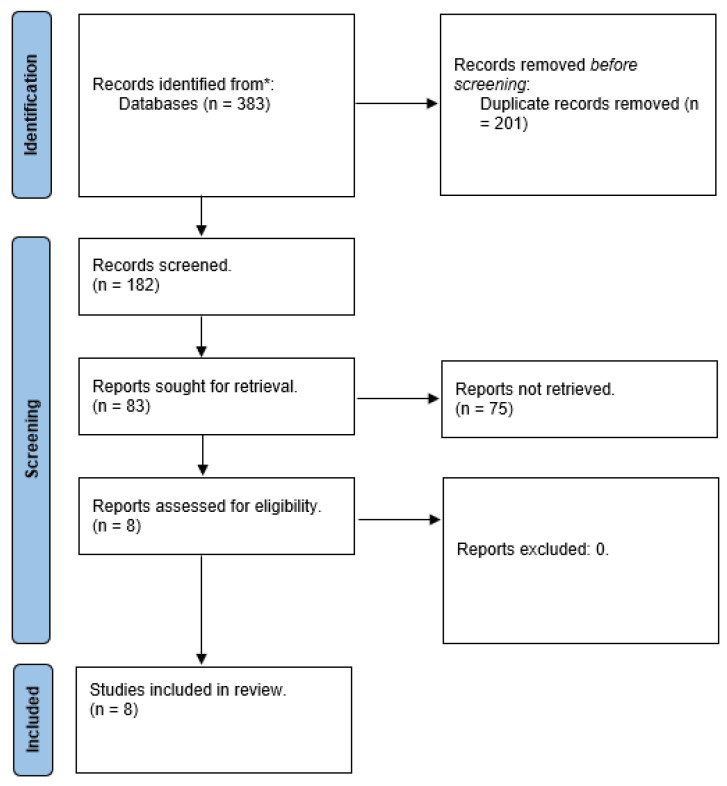 Figure 1
Figure 1 Figure 2
Figure 2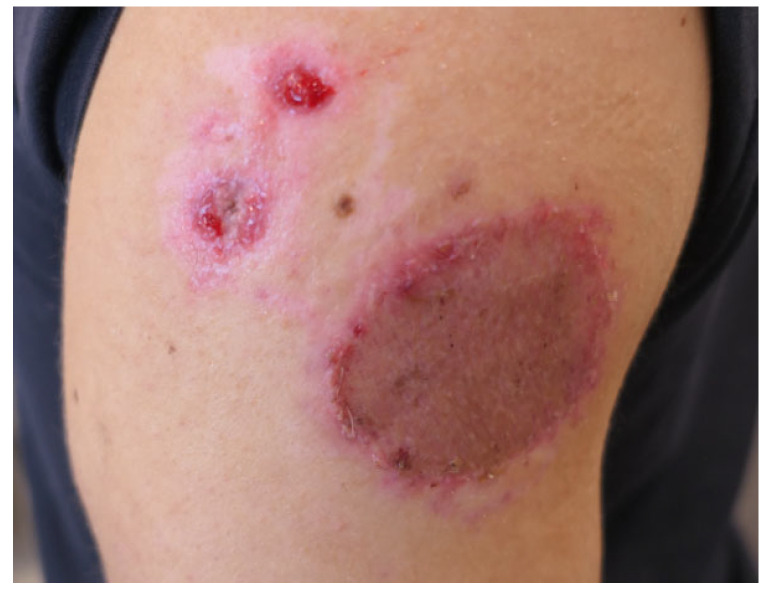 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurn Injury Management and Outcomes · Restraint-Related Deaths · COVID-19 and healthcare impacts
1. Introduction
Hypothermic injuries to the skin, or frostbite, seldom present at burn centres [1,2]. Frostbite is, however, not entirely uncommon in military personnel and mountain climbers exposed to cold or arctic weather conditions. Other risk factors for frostbite include homelessness, psychiatric conditions, high alcohol consumption, drug usage, car accidents or other occupational hazards in cold environments [2,3,4].
Common frostbite injuries usually occur due to cold weather conditions and cold exposure for longer periods of time. As the body re-directs its blood flow from the cold-exposed periphery to centrally placed organs, frostbite injuries mostly occur in the fingers, toes, ears and nose. Normal dermal blood flow is around 250 ML/min, but with hypothermia it can drop to 20–50 ML/min, and at temperatures below 0 °C blood flow stops. A cessation of dermal blood flow then causes progressive and deepening ischemia with cellular damage. This damage is either indirect due to dehydration [5,6,7] or due to freezing with intra- and extracellular crystal formation causing necrosis and cell death [6].
Vasodilatation with inflammatory processes occurs as a defence mechanism in order to ensure heat transport through the cold tissue, which, upon prolonged exposure, eventually also freezes, which increases the area of frostbite necrosis even further [7,8]
Nitrous oxide has many medical applications and has for more than a century found use as an analgesic in general anesthesia for dental procedures, childbirth and sedation [9]. Nitrous oxide is also commonly used at parties to fill balloons. It has, however, been used as an inhalant party drug for the induction of a short euphoria in recent decades [10,11].
Nitrous oxide is generally stored in gas cylinders in either liquid or compressed form under high pressure. The temperature of the liquified gas under normal pressure can be between −55 °C and −88.5 °C. When the gas is released, its temperature rapidly increases to −40 °C [12]. Direct skin contact with cold nitrous oxide directly from the container can cause frostbite depending on the length of exposure as well as exposure to the metal outer casing of the aerosol can by the cooled gas. The time needed for nitrous oxide to cause a deeper frostbite is not known [12].
Recent data suggest a small but globally increased number of skin frostbite cases caused by nitrous oxide [12,13].
2. Objective
This scoping review seeks to synthesize and draw conclusions from the existing English-language literature regarding frostbite injuries associated with the recreational use of nitrous oxide. Additionally, we provide a representative clinical case involving a 21-year-old male who experienced frostbite following skin exposure to nitrous oxide.
3. Method
3.1. Search Strategy
A literature search was performed and structured by a health science librarian. The databases utilized included Embase, Web of Science and PubMed^®^ as of 4 July 2024, with no restrictions on the time frame. The search terms incorporated various synonyms for “frostbites”, “cold injuries”, “cold burn”, “nitrous oxide”, “laughing gas”, and “nitrogen protoxide”. The overall count of scientific publications identified was 383. Following the elimination of duplicates, 182 articles were available for abstract screening. (Table 1). The PICO parameters used were P—recreational use of nitrous oxide; I—exposure to nitrous oxide; C—no/limited nitrous oxide exposure; and O—outcomes of cutaneous frostbite caused by recreational use of nitrous oxide.
3.2. Eligibility Criteria
The search was conducted without any language limitations, time constraints or restrictions on study design. The studies included focused on clinical cases involving patients who experienced frostbite to the skin as a result of recreational nitrous oxide use. Studies pertaining to the medical application of nitrous oxide were excluded, as were those involving frostbite injuries occurring in areas other than the skin and the medical use of nitrous oxide.
3.3. Study Selection
The abstract screening procedure was conducted utilizing Rayyan software 14. On this platform, a blinded review of the abstracts was executed. Two independent reviewers (S.H. and R.T.) assessed the studies for eligibility without prior knowledge of each other’s evaluations. The initial evaluation focused on the titles and abstracts, which was succeeded by a thorough examination of the full texts to determine the potential eligibility of the selected studies. Any discrepancies between the two reviewers were addressed through discussion until a consensus was achieved. If the two investigators disagreed and a consensus was not reached, a third investigator (J.Z.) was involved to cast the deciding vote.
3.4. Data Extraction
The data extraction was conducted using Excel (Microsoft Corp., Redmond, WA, USA). This pre-established spreadsheet encompassed details including the first author, country of publication, study design type, publication year, number of patients involved, average age, gender, frostbite location, treatment administered and outcomes achieved (see Table 2).
4. Results
Out of a total of 83 publications, 8 studies were selected for a full-text review as they meeting our inclusion criteria for analysis (see Figure 1). Our literature review included three case reports [15,19,20], four case series [10,12,16,17] and one Letter to the Editor [18]. The countries of publications were the UK (n = 3), the Netherlands (n = 2), Ireland (n = 2) and the USA (n = 1). The publication years spanned from 2020 to 2024, with one earlier study dating back to 1996 [19]. The majority of the studies were published between 2023 and 2024. Around 11 patients were injured on average each year between 2020 and 2024. The total number of patients included in the review was 54. The mean patient age was 25 years of age. The studies reported a higher number of female patients (n = 23) compared to male patients (n = 11). The most frequently affected area for frostbite was the inner thighs (n = 23), followed by the upper extremities, including the hands (n = 11), and the face (n = 3). Conservative wound management was the predominant treatment approach (n = 21), although debridement of necrotic tissue and split-thickness skin grafting were employed for deeper frostbite cases (n = 11). Most wounds demonstrated healing within a timeframe of 1 to 4 months (see Table 3).
Case Report
A previously healthy 21-year-old male was admitted to our outpatient clinic due to a frostbite injury to his right shoulder. No exact mechanism or length of exposure of the injury could be obtained due to him being unconscious after the recreational use of nitrous oxide. Through discussions and reasoning with the patient, it was assumed that, when unconscious, he had probably been lying on the cannister, leading to a prolonged exposure to both the released nitrous oxide and the cooled outside of the metal aerosol spray-can. The largest part of the frostbite on his right shoulder measured around 8 × 8 cm with two adjacent satellite lesions measuring 1 × 1 cm; Vaseline–gauze was applied. A week after the initial exposure to nitrous oxide, the wound was necrotic with clear signs of full-thickness skin damage (Figure 2). Wound debridement was performed and Vaseline–gauze applied. One week after debridement, the wound was covered with a split-thickness skin graft (STSG). The graft achieved a 100% take, and the wound was completely healed within one month of the initial injury (Figure 3).
5. Discussion
The occurrence of frostbite on the skin following recreational use of nitrous oxide appears to be on the rise, as indicated by various studies [12,15,17]. This pattern has been observed in countries such as the UK, Ireland, the Netherlands and, recently, Sweden as well [20]. In our department, we have noted a significant increase in frostbite cases associated with the recreational use of nitrous oxide. The presented case is one example of a patient have seen in our outpatient clinic after recreational misuse of nitrous oxide. Our literature review reveals that most relevant publications have emerged in recent years, particularly between 2022 and 2024. Notably, the first documented case reported in 1996 by Hwang et al. [18] involved a 54 year old male “sniffing” nitrous oxide. This case is distinct from more recent reports, which predominantly feature a younger demography using nitrous oxide as a party drug. A comparison of the seven additional studies included in our review indicates that such frostbite injuries are most frequently observed in young adults, with a higher prevalence among females, and are typically localized to the inner thighs. The prevailing treatment approach, as supported by the current literature, involves initial conservative management, and excision and split-thickness skin grafting (STSG) in the second place.
Baran et al. [17] reported on treating 20 patients suffering from severe frostbite due to the misuse of nitrous oxide. This is the largest study of describing this specific patient group, although it is lacking detailed information regarding factors such as age, gender, the location of frostbite and the treatment administered to each individual. Notably, it was found that the most frequently affected area was the inner thighs, which aligns with the existing literature. The second largest case series by Chen et al. [12] includes 16 patients, with a mean age of 22.5 years. This series provides more comprehensive data on each patient and their subsequent treatment. The findings of this case series are consistent with the overall conclusions drawn from this literature review regarding gender and the site of injury, indicating that the typical patient is a young female in her twenties sustaining frostbite injuries to the inner thighs.
The inner thighs are the most common site of frostbite injury from nitrous oxide. This is most probably due to prolonged exposure to the metal canister held between the legs while filling balloons with gas [12,15,16,17]. Frostbite injuries following nitrous oxide exposure are frequently deep, with a full-thickness injury often requiring debridement and STSG, compared to frostbite caused by environmental conditions, where the majority of cases are treated conservatively with wound dressings.
6. Limitation
In our study, only one patient agreed to participate, and a case series was unfortunately not possible. During the past two years, eight patients have been treated at our unit due to a frostbite injury to the skin due to recreational use of nitrous oxide. Previous studies have described difficulties in follow-up with this group of patients after injuries due to the recreational use of nitrous oxide [12,16,17,19]. These patients often present within a few days, and they often miss or opt-out of planned appointments and are lost to follow-up, compared to other injuries such as burns. The delay in presentation and decreased compliance in follow-up can lead to increased risk of infection and scarring with poor esthetic results [16]. It is notable that we did not find any articles from, e.g., Asia, in our literature review, although this does not preclude the possibility that this is potentially a worldwide issue.
7. Conclusions
This study represents the first literature review summarizing frostbite injuries to the skin resulting from nitrous oxide misuse. There is a need for enhanced preventive measures, such as media attention, which may raise public awareness and possibly decrease the incidence of frostbite injuries associated with the recreational misuse of nitrous oxide.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Edlich R.F. Chang D.E. Birk K.A. Morgan R.F. Tafel J.A. Cold injuries Compr. Ther.19891513212676329 · pubmed ↗
- 2Kyösola K. Clinical experiences in the management of cold injuries: A study of 110 cases J. Trauma 197414323610.1097/00005373-197401000-000044149073 · doi ↗ · pubmed ↗
- 3Pinzur M.S. Weaver F.M. Is urban frostbite a psychiatric disorder?Orthopedics 199720434510.3928/0147-7447-19970101-099122052 · doi ↗ · pubmed ↗
- 4Valnicek S.M. Chasmar L.R. Clapson J.B. Frostbite in the prairies: A 12-year review Plast. Reconstr. Surg.19939263364110.1097/00006534-199309001-000128356126 · doi ↗ · pubmed ↗
- 5Basit H. Wallen T.J. Dudley C. Frostbite Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2024 Available online: http://www.ncbi.nlm.nih.gov/books/NBK 536914/(accessed on 13 October 2024)
- 6Robson M.C. Heggers J.P. Evaluation of hand frostbite blister fluid as a clue to pathogenesis J. Hand Surg.19816434710.1016/S 0363-5023(81)80010-X 7204918 · doi ↗ · pubmed ↗
- 7Mc Cauley R.L. Hing D.N. Robson M.C. Heggers J.P. Frostbite injuries: A rational approach based on the pathophysiology J. Trauma 19832314314710.1097/00005373-198302000-000136827634 · doi ↗ · pubmed ↗
- 8Nakae H. Endo S. Inada K. Yamashita H. Yamada Y. Takakuwa T. Kasai T. Ogawa M. Uchida K. Plasma concentrations of type II phospholipase A 2, cytokines and eicosanoids in patients with burns Burns J. Int. Soc. Burn Inj.19952142242610.1016/0305-4179(95)00022-48554682 · doi ↗ · pubmed ↗