Influence of Urban and Rural Areas, Type of School, and Parents’ Education Level on Nutrition Habits and Their Relationship with Dental Caries in Schoolchildren in Mallorca
Daniela Vallejos, Irene Coll, Nora López-Safont

TL;DR
This study shows how nutrition habits and dental caries in Mallorcan schoolchildren are influenced by urban/rural location, school type, and parents' education.
Contribution
The study identifies specific dietary patterns and their link to caries risk based on geographic and socioeconomic factors in schoolchildren.
Findings
Rural 5–6-year-olds consume more sweets than urban children, increasing caries risk.
Public school 15-year-olds eat more potato chips than those in subsidized/private schools.
Lower maternal education correlates with fewer students eating dinner regularly.
Abstract
Background/Objectives: Habits such as a diet high in sugars and poor dental biofilm control are linked to a higher prevalence of caries and low socioeconomic status. This study aimed to analyze the nutrition habits of schoolchildren in Mallorca and their relationship with the presence of dental caries, depending on the type of school, geographic location, and parents’ education level. Methods: A cross-sectional study was conducted to examine the prevalence of dental caries based on World Health Organization (WHO) standards and nutritional practices following guidelines from the Food and Agriculture Organization of the United Nations (FAO) and the European Food Safety Authority (EFSA). This study included 718 students from three age groups: first-year elementary students (ages 5–6), sixth-year elementary students (age 12), and fourth-year secondary school students (age 15). Relevant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
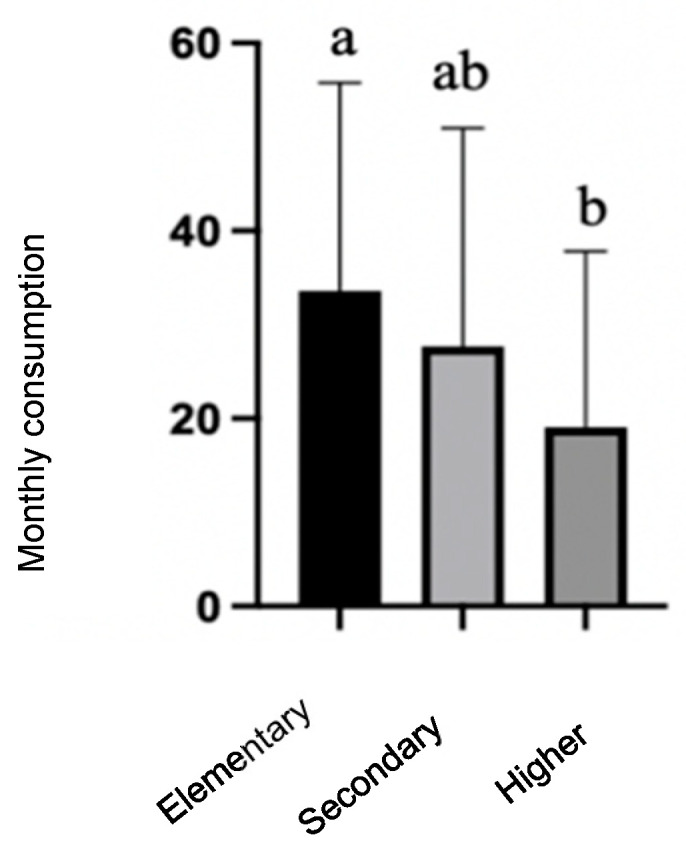 Figure 1
Figure 1- —ADEMA+ Foundation
- —SESPO
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Child Nutrition and Water Access · Nutritional Studies and Diet
1. Introduction
The developmental years between childhood and adolescence are a fundamental period of socialization, during which eating habits are formed that are maintained into adulthood. This process is affected by socioeconomic, cultural, and environmental factors [1]. Thus, childhood experience is crucial to future health due to the continuous malleability of biological systems, and there is evidence that healthy habits, such as good nutrition and exercise, are influenced by the examples of parents and peers [2]. Students spend a significant part of their day at school, so it is reasonable to expect that the school environment plays an important role in teaching and shaping eating habits [3].
Dietary patterns have important implications, especially for the prevention or development of chronic diseases. Although children’s eating habits are difficult to change directly, parental eating habits are considered a good target for interventions aimed at preventing unhealthy eating behaviors in children [4,5].
Dental caries is a non-communicable disease strongly linked to lifestyles and harmful behaviors, mainly related to inadequate dietary patterns, and is linked to a dysbiosis of the dental biofilm caused by exposure to free sugars [6].
The most relevant modifiable behavioral factors correlating with a higher prevalence of caries are a diet high in sugars and poor dental biofilm control. Many studies seem to indicate that these unhealthy habits are associated with low income [6,7,8,9,10].
The frequency and type of foods consumed as well as dietary consistency significantly impact oral health. Diets high in sugars and carbohydrates are associated with an increased risk of dental caries, periodontal disease, and oral cancer. In addition, oral health influences the ability to maintain a nutritious diet, affecting chewing, taste perception, and nutritional intake [11].
Additional research indicates that processed food containing sugar and starch increases the risk of dental caries [12]. In contrast, the intake of natural sugars from cereals, fruits, vegetables, and milk does not substantially contribute to the onset of dental caries or other non-communicable diseases, owing to protective elements such as fiber, water content, polyphenols, and calcium [11,12]. In addition, chewing these foods stimulates salivary flow, mitigating the risk from sugars [13,14].
The amount and frequency of sugar consumption are risk factors for developing dental caries. Animal and human studies have shown that both variables significantly influence the development of caries [14,15,16]. Therefore, both the amount and frequency of sugar intake should be considered to prevent caries and other non-communicable diseases. However, the relationship between other nutritional patterns, such as skipping meals or eating outside the home, has not been as extensively studied.
Despite the increasing body of research regarding the link between nutrition and oral health, no studies have specifically investigated this relationship in schoolchildren in Mallorca.
This study aimed to analyze the influence of the type of school, geographic location, and parents’ education level on the nutrition habits of schoolchildren in Mallorca and their relationship with the presence of dental caries.
2. Materials and Methods
2.1. Study Design and Target Population
A cross-sectional observational epidemiological study was conducted in the school population in Mallorca between October 2018 and December 2019. The sample size was calculated as follows. For a population of 12,000 children and a caries prevalence of 0.35 extracted from the National Institute of Statistics, the minimum sample size was approximately 340 children to achieve a 95% confidence level with a 5% margin of error. However, we wanted to increase the sample size to enhance the accuracy of our effect estimates, reduce the margin of error, and increase the statistical power of this study. For that, we analyzed 718 students in three age groups—5–6 years (first-year elementary school), 12 years (sixth-year elementary school), and 15 years (fourth-year secondary school)—in the 28 schools selected. The epidemiological study design used a stratified cluster sampling technique, following the Pathfinder method [17]. This method allows the most important population subgroups that may have different levels of disease to be included. The selected age groups are WHO-designated “index ages”, recommended for examination. Schools were chosen using a systematic random sampling method, grouping the sample into three strata based on the population characteristics of Mallorca, as shown in Table 1.
The sampling sites (schools) for the study population were identified using data from the General Directorate of Planning, Organization, and Schools of the Autonomous Community of the Balearic Islands (CAIB) and the National Institute of Statistics (INE). Students aged 5–6, 12, and 15 years were selected, corresponding to first-grade and sixth-grade elementary and fourth-year secondary school in the chosen schools across Mallorca. The design, protocol, and methodology of the transversal study are described in more detail elsewhere [17,18].
Fieldwork and data collection were conducted on-site at the schools. Seven examining dentists performed the inspections under standardized conditions, utilizing a headlamp, a #5 intraoral flat mirror, and a WHO periodontal probe according to the WHO recommendations for oral health surveys [19]. The calibration and training of the examining dentists followed WHO guidelines. The simple agreement rate was 98.7%, and the Kappa index, evaluated using the Landis and Koch scale, was 0.757. This indicated a high level of agreement (greater than 95% for simple agreement and greater than 0.61 for Kappa), which was deemed sufficient to commence this study.
The data were collected using the form specified by the WHO Oral Health Surveys: Basic Methods [19] (Annex 2 of the Oral Health Surveys: Basic Methods Manual) and the oral health questionnaire for children (Annex 8 of the same manual).
The nutrition habits of students were also studied through surveys that provide information on diet-related knowledge, attitudes, and practices, adaptable KAP questionnaires extracted from the FAO publication “Guidelines for assessing nutrition-related Knowledge, Attitudes and Practices” (FAO, 2014) [20]. A questionnaire on food consumption patterns was also administered, following the guidelines proposed by the European Food Safety Authority (EFSA, European Food Safety Authority). These guidelines are part of the “EUMenu Project” in Europe and are included in the European methodological guide of 2009, “General principles for the collection of national food consumption data in the view of a pan-European dietary survey” (EFSA, 2009) [21].
The questionnaires on knowledge and nutritional habits were administered by a multidisciplinary team of health care professionals (dentists, doctors, biologists, and nutritionists) who posed the questions to the schoolchildren and recorded the responses. Unanswered questions were considered missing values (excluded from the analysis). The design, protocol, and methodology of the surveys are described elsewhere [22].
2.2. Study Variables
The study variables are as follows.
Sociodemographic variables:
- Age;
- Type of school: public or subsidized/private;
- Geographic location: urban or rural;
- Education level of parents/guardians: includes the educational level of both the mother and father, categorized as elementary, secondary, or higher education.
Nutritional variables:
- Frequency of food consumption: the number of times consumed per month;
- Nutrition-related attitudes and practices: an assessment of the number of meals per day, where they were eaten, and the purchase of snacks.
Oral health variables:
- Experience of caries is determined through the DMFT index in permanent teeth, where D=decayed teeth, M=missing teeth due to caries, and F=filled teeth corresponding to the unit being assessed. The analysis of caries experience uses the total sample (for children aged 5–6 years, among those who had mixed dentition, only permanent teeth were considered).
2.3. Ethical Treatment of the Data
Prior to beginning this study, approval was granted from the ethics board of the Balearic Islands (CEI: IB3737/18) in compliance with prevailing legislation, and this study was implemented in conformity with the principles outlined in the Declaration of Helsinki and the standards of good clinical practice. Before data collection, the data sheet and the informed consent form were given to the children’s parents/guardians; only those children who had previously submitted the consent form signed and dated by their parents/guardians participated in this study.
All the collected data were entered into an automated file with restricted access, and personal data were encrypted to guarantee confidentiality.
2.4. Statistical Analysis
The data were analyzed using the SPSS 27.0.1.0^®^ statistics application, depending on the type of variable and the groups to be analyzed. The effects of the following factors on the different variables were assessed: the type of school (public or subsidized/private), geographic location (urban or rural), and education level of the mothers/guardians and fathers/guardians (elementary, secondary, and higher education). To compare means, Student’s t-test or a one-way analysis of variance (ANOVA) was used in conjunction with the Bonferroni post hoc analysis. The percentages were compared with chi-square tests using the cross-table procedure—the cross-tabulation tool analyzed risk by calculating the odds ratio (OR), and this analysis was used to determine the effect size. In every case, the 95% confidence interval estimate (p < 0.05) was used to determine the precision of the random error present in the data.
3. Results
3.1. Sample Description
During the period in which this study was conducted, 718 students in the first year of elementary school (5–6 years), sixth year of elementary school (12 years), and fourth year of secondary school (15 years) were explored. Table 2 shows the students’ distribution according to age, sex, and school type.
3.2. Nutrition Habits
3.2.1. Frequency of Food Consumption
From the data collected through the survey on the frequency of consumption of the food groups that form part of the students’ diets, foods that are related to the development of dental caries were selected and detailed by the children’s age.
In the group of 5–6 year olds, higher consumption of processed and sugary foods such as pastries, sausages, sugary soft drinks, commercial juices, and sweets in children from rural sectors than those residing in urban areas is illustrated in Table 3.
In the group of 12 year olds, the results show a higher frequency of consumption of foods such as pastries, potato chips, sugary soft drinks, and sweets in rural students compared to those living in urban areas. No differences were observed according to the type of school attended, as shown in Table 4.
In the case of the 15 year olds, higher consumption of potato chips and sausages was observed in students from rural areas and public schools compared to urban areas and subsidized or private schools. Commercial juices were consumed more frequently in public schools, as shown in Table 5.
The results indicate that a lower education level of the parents/guardians was associated with a higher consumption of sausages. The mean frequency of consumption was significantly higher in students with parents who had only elementary education (33.57 ± 22.190) than in those with parents/guardians with higher education (19.08 ± 18.72; p = 0.004), as shown in Figure 1.
3.2.2. Meals During the Day
Another important factor that was evaluated to assess nutrition habits was whether schoolchildren consumed all the main meals of the day and where they ate them.
Snacks between meals and whether they bought these foods with their own money were also considered.
As illustrated in Table 6, in the 5–6-year-old group, more children from urban areas (99.3%) ate breakfast at home than schoolchildren from rural areas (93.7%; p = 0.043).
Table 7 shows that a higher proportion of 12 year olds in urban areas (97.1%) ate lunch than those in rural areas (86.3%; p = 0.010). Additionally, 5–6 year olds from rural areas (90.1%) and public schools (85.9%; p = 0.037) tended to have lunch at home in a higher proportion than students from urban areas (77.6%) and subsidized/private schools (73.6%; p = 0.043).
Table 8 shows the proportion of students who ate dinner and where they ate it; in this case, no significant differences were observed between the groups.
Among 15 year olds, a higher percentage of students in rural areas (29%) and public schools (25.5%; p = 0.004) reported purchasing snacks with their own money compared to those in urban areas (13%) and subsidized/private schools (7%; p = 0.008).
3.2.3. Parents/Guardians’ Education Levels
The findings indicate that the education level of the mother/guardian affected the proportion of 15 year olds who had dinner. Fewer adolescents who ate dinner were noted among students with mothers with a lower education level (elementary: 75%; secondary 91%; higher: 98%; p = 0.003).
The influence of the father/guardian’s education level was related to where the 15 year olds had dinner; a higher education level was related to a higher proportion of children eating at home (elementary: 93%; secondary 98%; higher 100%; p = 0.031).
3.3. Effect of Nutrition Habits on the Experience of Caries in Schoolchildren
3.3.1. Consumption of Sugary Foods
In an analysis of the impact of food consumption on students’ experience of caries, using an OR analysis, we found an increased likelihood of caries in permanent teeth among schoolchildren who reported a higher frequency of sweets consumption than those with lower consumption rates (OR= 1.757; CI= 1.036–2.978; p = 0.035), as shown in Table 9. According to our results, the other processed foods were unrelated to a higher caries frequency.
3.3.2. Meals During the Day
The results show that habits that respected compliance with the main meals were related to better oral health. As shown in Table 10, a higher proportion of students with experience of caries ate breakfast (93.6% vs. 86.7; p = 0.004) and dinner (97.6% vs. 92.8%; p = 0.004) than those with an experience of caries.
Conversely, where lunch was eaten seemed to influence the experience of caries. More children with an experience of caries ate lunch outside of home or school (19%) than children with no experience of caries (11% p = 0.009).
The results show no significant difference in the experience of caries between schoolchildren who ate snacks (yes: 64.4%; no: 35.6% p = 0.853) and those who bought food with their own money (yes: 18.9%; no: 81.1% p = 0.310)
4. Discussion
The data analysis in this study indicates that the sociodemographic factors analyzed, such as geographic location, school type, and parents’ level of education, influenced the nutrition habits of the schoolchildren who participated in the project. In addition, we noted that some of these habits were related to the experience of caries in students.
The mechanisms through which the environment affects the health behaviors of children and adolescents have been articulated in multiple ways, with some authors indicating that the social groups in which children engage transmit their social norms and attitudes by filtering and adapting the media messages that children encounter [4]. On the other hand, it is considered that the perception and knowledge shared about a healthy lifestyle are influenced by factors such as communication, socioeconomic level, and parenting practices and style [23].
Our findings suggest that the parents’ education level influences nutrition habits; a higher education level correlates with a lower consumption of some processed foods, such as sausages, and a greater number of children who eat dinner at home. Evidence has shown that children’s food preferences are related to parental eating habits, economic conditions, and nutritional knowledge [24]. The mother’s education level significantly affects the dietary habits of children and adolescents; children of mothers with low education levels exhibit increased consumption of sugar, fat, and protein [4,25].
Although we did not directly determine the socioeconomic levels of the students who participated in this study, the data provided by the National Statistics Institute (INE) [26] show that private or subsidized schools are always concentrated in high-income areas, unlike public schools, most of which are in areas with fewer resources, with a predominance of low and lower-middle-class students [27]. Regarding geographic location, our data showed that the proportion of caregivers with higher education is greater in urban than rural areas. These differences have been attributed to the greater difficulty that rural inhabitants have in accessing health care, education, job opportunities, technology, public transportation, and commerce [28,29]. This means that rural regions have distinct economic, social, and structural characteristics that lead to the development of social disparities and exacerbate social inequalities in health.
There is evidence of poorer oral health in rural areas, and this is associated with factors such as limited access to oral health care, low education levels, and less healthy lifestyles [8,9,10]. For example, adults living in rural areas visit the dentist less often, have less frequent cleanings, and have more extractions of permanent teeth than adults in urban areas [30].
These factors also exerted a certain influence on the students’ dietary habits in this study, and this is reflected in our results, where we noted more frequent consumption of some processed and sugary foods such as pastries, sugary soft drinks, commercial juices, sausages, potato chips, and sweets in rural areas and public schools compared to subsidized/private schools located in urban areas. We observed that schoolchildren who reported a higher frequency of candy consumption had a higher probability of caries in their permanent teeth, while sugary drinks and sodas did not show the same association. The possible reasons why only candy consumption was statistically significant may be related to consumption patterns. Sweets are generally eaten between meals, increasing prolonged exposure to sugar, while sugary drinks and sodas are typically consumed with main meals. These observations have a certain level of limitation in the 5–6-year-old group, as primary teeth were not considered in the analysis and may not fully reflect the impact of nutritional habits on caries in this age group; this limitation can be addressed in future studies.
In addition, there was greater compliance with the three daily meals in urban areas than in rural areas. These findings are relevant if we consider that some authors point out that dietary quality is influenced by practices such as breakfast [31,32] and that children who eat breakfast at home with their parents have a lower consumption of sugary drinks [33].
These disparities are ascribed to many variables; some authors characterize those with limited means as being at an elevated risk of experiencing economic hardship, rendering them more susceptible to consuming a less nutritious diet. This is because low-cost and more energetic foods are readily available in socioeconomically deprived areas, in addition to the influence of a higher education level on healthier nutrition habits related to knowledge, beliefs, and the ability to assimilate nutritional information [34,35,36,37].
Conversely, our study revealed an increased likelihood of caries in permanent teeth among schoolchildren who reported a higher frequency of sweet consumption, aligning with the existing literature that indicates a heightened risk of caries in individuals who frequently eat sugary foods [6].
Our findings indicate that habits such as eating breakfast and dinner correlate with a reduced incidence of caries. Additionally, where lunch is consumed appears to impact the oral health of schoolchildren, which can be explained by the association of these dietary patterns with a healthier diet [31,32].
The findings from the 2020 Spanish Oral Health Survey emphasize the ongoing challenges related to socioeconomic disparities in oral health, as children from lower socioeconomic backgrounds tend to have higher caries rates [38]. The survey shows improvements in dental health across various age groups. For 5–6 year olds, the DMFT index for permanent teeth is 0.06; in 12 year olds, the DMFT index for permanent teeth is 2.03, and in 15 year olds, it is 2.66 [38]. In fact, we can observe the same situation in the Balearic Islands in a previous study. Regarding the prevalence of caries prevalence, we indicate that at the ages of 5–6, 12, and 15, the trend is the same, dropping from 45.5% to 40%, from 34.9% to 27.9%, and from 60.2% to 45.49%, respectively (in 10 years) [18].
Although this study focused on nutritional habits, it would be interesting to explore in future studies the relationship between sociodemographic variables, such as gender, education level, geographic location, type of school, and parental education, and the prevalence of dental caries in children from Mallorca. This approach would provide a more comprehensive understanding of the factors influencing children’s dental health.
A limitation of this study is the sample size, which is focused only on the Mallorca population. Expanding the sample to include a broader, more diverse group from different regions of Spain or the Balearic Islands would enhance the generalizability of the findings. Additionally, due to the cross-sectional design, the main weakness of this study is the lack of follow up, which limits the ability to establish a causal relationship.
5. Conclusions
According to the results, the type of school, geographic location, and parents’ education level seem to influence children’s eating habits. The dietary habits of schoolchildren, particularly the consumption of sweets, were associated with the prevalence of caries. While the evidence suggests a link between dietary habits and oral health, further investigation is needed to fully understand the broader impact on overall health and the role of the surrounding environment in shaping these habits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cheikh Moussa K. Sanz-Valero J. Wanden-Berghe C. The social determinants of health of the child-adolescent immigration and its influence on the nutritional status: Systematic review Nutr. Hosp.201430100810192536500310.3305/nh.2014.30.5.7732 · doi ↗ · pubmed ↗
- 2Wilkinson R.G. Marmot M. Los Determinantes Sociales de Salud: Los Hechos Probados Organización Mundial de la Salud Geneva, Switzerland 2006
- 3Rovner A.J. Nansel T.R. Wang J. Iannotti R.J. Food sold in school vending machines is associated with overall student dietary intake J. Adolesc. Health 201148131910.1016/j.jadohealth.2010.08.02121185519 PMC 3011970 · doi ↗ · pubmed ↗
- 4Scaglioni S. De Cosmi V. Ciappolino V. Parazzini F. Brambilla P. Agostoni C. Factors Influencing Children’s Eating Behaviours Nutrients 20181070610.3390/nu 1006070629857549 PMC 6024598 · doi ↗ · pubmed ↗
- 5Wechsler H. Devereaux R.S. Davis M. Collins J. Using the school environment to promote physical activity and healthy eating Prev. Med.200031 S 121S 13710.1006/pmed.2000.0649 · doi ↗
- 6Giacaman R.A. Fernández C.E. Muñoz-Sandoval C. León S. García-Manríquez N. Echeverría C. Valdés S. Castro R.J. Gambetta-Tessini K. Understanding dental caries as a non-communicable and behavioral disease: Management implications Front. Oral Health 2022376447910.3389/froh.2022.76447936092137 PMC 9448953 · doi ↗ · pubmed ↗
- 7Khalid T. Mahdi S.S. Khawaja M. Allana R. Amenta F. Relationship between Socioeconomic Inequalities and Oral Hygiene Indicators in Private and Public Schools in Karachi: An Observational Study Int. J. Environ. Res. Public Health 202017889310.3390/ijerph 1723889333265929 PMC 7730931 · doi ↗ · pubmed ↗
- 8LešićS. DukićW. Šapro Kriste Z. TomičićV. KadićS. Caries prevalence among schoolchildren in urban and rural Croatia Cent. Eur. J. Public Health 20192725626210.21101/cejph.a 531431580564 · doi ↗ · pubmed ↗