Sociodemographic and early-life predictors of being overweight or obese in a middle-aged UK population– A retrospective cohort study of the 1958 National Child Development Survey participants
Glenna Nightingale, Karthik Mohan, John Frank, Sarah Wild, Sohan Seth

TL;DR
This study explores how early-life and sociodemographic factors influence obesity in middle-aged individuals in the UK.
Contribution
The study quantifies the long-term impact of early-life and maternal factors on obesity risk, showing their persistence over time.
Findings
Maternal obesity strongly predicts obesity in offspring at ages 16 and 42.
Maternal smoking increases the risk of obesity in offspring across multiple age points.
Females are more likely to be overweight at 16 but less likely to develop obesity later.
Abstract
Obesity has become a global public health concern. However, its precise origins and causation are still hotly debated, especially the relative importance of individual-level genetics and behaviours, as opposed to obesogenic environmental factors. Our key objective is to quantify the impact of sociodemographic and early-life course predictors of being overweight or obese at 16, being overweight/obese/severely obese42 years of age, and on the incidence of a status of being overweight/obese/severely obese between 16 and 42 years of age, spanning the years before and after marked increases in obesity prevalence in the UK. We used data collected from participants and their mothers from the 1958 National Child Development Survey. The outcomes of interest were being overweight (defined as 25kg/m2<BMI≤29.9kg/m2 ) or obese (defined as BMI > 30 kg/m2) at 16 and 42 years of age and incident…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
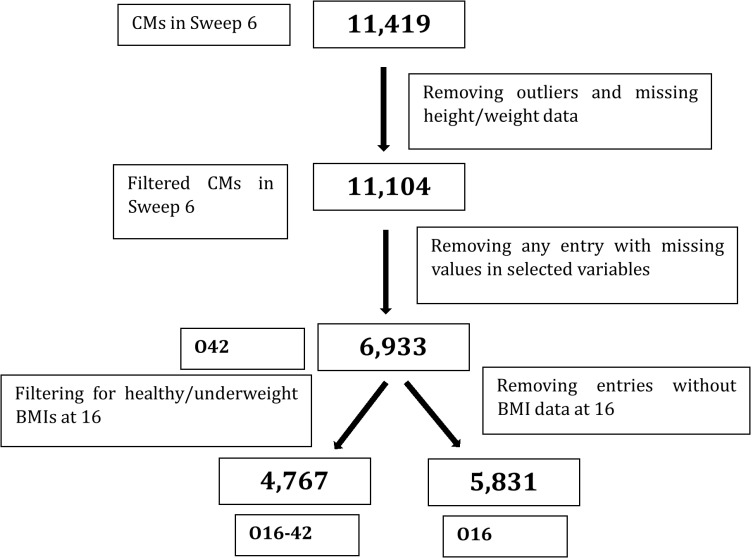 Fig 1
Fig 1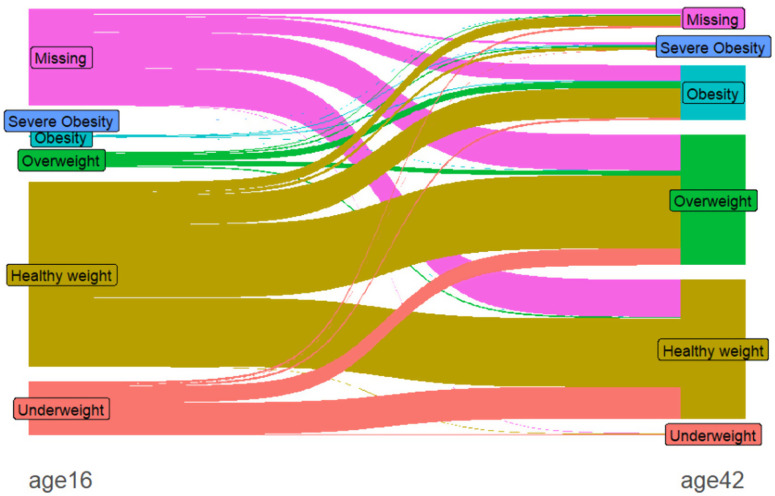 Fig 2
Fig 2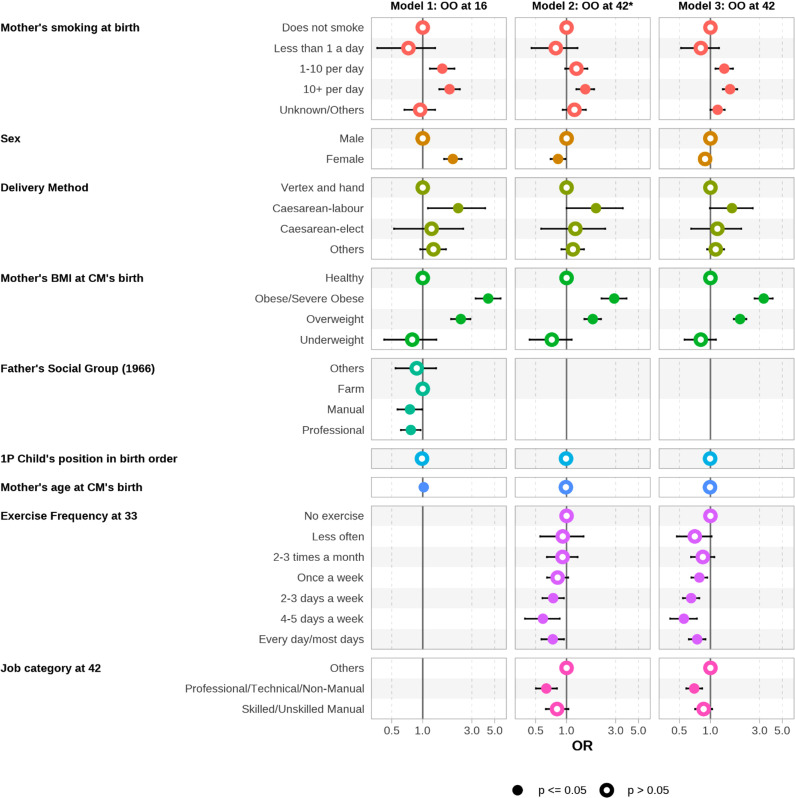 Fig 3
Fig 3- —Challenge Investment Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · Birth, Development, and Health · Obesity and Health Practices
Introduction
The public health concern of obesity and, to a lesser degree, overweight, is a critical research priority globally [1–4] Obesity increases the risk of cardiovascular disease, osteoarthritis, type 2 diabetes, and some cancers [5]. Addressing the obesogenic environment and promotion of healthy behaviours in individuals form components of public health intervention. In recent years, the life course approach [6] has demonstrated that maternal factors, early-years characteristics and socio-economic status at all stages of life are associated with weight-for-height, i.e., body mass index (BMI) trajectories. This study uses the National Child Development Survey (NCDS), also known as the 1958 British Cohort Study, (Power & Elliott, 2006) to investigate the life-course determinants of obesity among individuals during whose lifetime the obesity “pandemic” has developed in the UK. The NCDS begun in 1958 and has been following individuals born in a single week of March 1958 to present. There have been 10 sweeps so far and the last sweep was in 2020 where the cohort members were 62 years of age. For the first survey sweep, the total number of individuals surveyed was 17,415 and were born in either England, Scotland or Wales – this has been reported to be 98% of all births across England, Scotland and Wales.
The childhood experiences of the cohort were different from that experienced by children in the 2020s [7] and the levels of obesity were not as high as at present. During the childhood period of the cohort, most households lacked basic facilities, and breast-feeding and maternal smoking were common.
Notably, the cultural and physical environments in the UK, especially features related to access to and consumption of food and facilitators of/barriers to physical exercise habits, have changed markedly over the cohort’s lifetime.
We were able to identify only one study [8] that uses the NCDS dataset to assess the influence of childhood life-course risk factors on obesity through multivariate analysis, using data from 11,752 participants with BMI measurements at 23, 33 and 42 years of age as outcome. The study only investigated the influence of four variables, i.e., low or high birthweight; never breastfed; physical activity at age 11; and at least one obese parent at age 11. The only other relevant primary study is based on a much smaller (n = 762) Dutch cohort, modelling BMI in a cohort born between 1977 and 1986 (when the obesity pandemic had already begun) [9]. This study only modelled BMI at three ages between 2 and 6 years as continuous variables. Other recent studies [10] using multiple risk factors in the Growing Up in Scotland Cohort data [11,12]and using Born in Bradford Cohort data [13] have used more potential risk factors and performed better in predicting later-onset of obesity as measured by AUC-ROC.
Our study models the influences of not only early-life predictors but also socioeconomic factors such as father’s social class. Our study also uses exercise frequency at age 33, which is the only “lifestyle” risk factor on which adequately complete data were available (with only 13.28% data missing).
The epidemiological association, between maternal characteristics and childhood obesity is well established [2,14,15]. Smoking during pregnancy, maternal BMI and parental socioeconomic status have frequently been implicated as risk factors for obesity in the offspring. For example, mothers’ smoking during pregnancy was weakly associated (OR 1.56 CI 1.13 to 2.15) with obese growth trajectories in children [2,15].
Low birthweight (LBW) has been linked (Oken , 2009) to obesity, and adult chronic health conditions [16,17]. However, absence of reliable gestational age data at the time of our cohort’s birth, i.e., well before ultrasound was available, precluded analysing small-for-gestational age subjects separately from premature births, which we felt precluded sensible interpretation of such an analysis. However, we did examine whether the three obesity outcomes were associated with lower birth weight, but have not presented the results in this paper.
Aims
Our aim was to describe the sociodemographic and early-life predictors of being overweight or obese (O16) at 16 years of age, of being overweight, obese or severely obese at 42 years of age(O42), and additionally of accruing obesity between 16 and 42 years of age. That is, not being overweight nor obese at 16 years of age but being overweight or obese or severely obese at 42 years of age (O16-42). Note that in our study, the BMI categories underweight, healthy, overweight, obese and severely obese are categorized by , , , , and respectively, where BMI is measured in kg/m^2^. The corresponding research questions are:
What are the sociodemographic and early-life predictors of being overweight/obese at 16 years of age [O16]?What are the sociodemographic and early-life predictors of being overweight/obese/severely obese at 42 years of age [O42]?What are the sociodemographic and early-life predictors of not being overweight/obese at 16 years of age but being obese or severely obese at 42 years of age [O16-42]?
Data variables used in this study.
We conducted a retrospective cohort study using the NCDS [7] dataset on a cohort of individuals all born within the same week in 1958. Data have been collected 12 times between 1958 and 2020 with each data collection known as a ‘sweep’. Notably, because this cohort’s members were all born in the same week of 1958, we do not need to account for period (calendar-time) effects. The dataset contained information at 0, 7, 11, 16, 23, 33, 42, 44, 46, 50, 55, and 62 years of age. For this project, we used data collected at 0, 7, 11, 16, 33 and 42 years of age (corresponding to sweeps 0, 1, 2, 3, 4, 5 and 6 respectively) [18].
The age of 42 years was chosen because of limited missingness and to provide data for early middle age – prior to the perimenopause for most women. Additionally, the age of 16 was chosen to compare early and middle adulthood. Of the data sweeps available in our dataset, the one at age 16 was closest to what most people think of as “the end of childhood”. At age 16, female members, would have already experienced menarche and the potential weight fluctuations associated with puberty.
The data variables considered in this study are BMI (participant’s mother at birth, and participant at 16 and 42 years of age), exercise frequency at 33 years of age, method of delivery at birth, father’s social class at birth, participant’s birth weight, birth order, whether or not the mother smoked at birth, age of mother at birth, and participant’ sex. The reference/comparison group for each of the categorical variables was guided by reported associations for these variables observed in the literature such as in (Doi et al., 2016).
The exercise frequency at 33 years of age provides an indication of the impact of exercise on obesity incidence (in subsequent years, leading up to age 42, when BMI was measured). Variables such as father’s social class, participant’s sex, birth weight and birth order were considered to incorporate socio-demographically important factors into the analysis.
Further details on the data sweeps and variables used in this study can be found in S1 Table1 and S2 Table 2 in S1 File, respectively. The data transformations employed in this study are detailed in S3Text, S4 Table 3, S5 Text, S6 Text, S7 Table 4, S8 Text, S9 Text, and S10 Table 5 in S1 File).
Methods
Data missingness and anomalies
After excluding records for which the predictors of interest were missing, 6,933 individuals had data available for O42. Among these individuals, 5,831 individuals had both height and weight available at 16 years of age and were used for O16. Among these individuals, 4,767 individuals were not overweight at 16 years of age and were used for O16-42.
Finally, in sweep 6 we identified outliers due to missing values being encoded as a high value (9999 or similar). We also excluded values in the birthweight variable which were only estimates due to low accuracy.
Fig 1 depicts the process followed. The characteristics of key variables (xsee S11 Figure, S12 Figure, and S13 Figure in S1 File) for the complete cases dataset of 6,933 were similar to those of the full dataset of 11,419.
Flow diagram depicting the sample size for each research question.
Exploratory analyses and inferential statistics.
We summarised the variables used in our study in Table 1. Our modeling approach involves using logistic regression to describe the associations between risk factors of being overweight/obese at 16 years of age (O16), of being overweight, obese/severely obese at 42 years of age (O42) and being overweight/obese/severely obese at 42 years of age for individuals who are healthy or underweight at 16 years of age (O16-42). The predictors of the models considered are outlined in Table 1.
Table 1: Predictors and outcome for each model.
The predictors used for the model O42 are based on the results of stepwise elimination of predictors, starting with those with the least significant p-values under p = 0.05, informed by two considerations: a) AIC change: if the AIC was reduced by at least 2, the predictor was retained in the model under consideration, and b) any predictor which caused a change of more than 10% in any other predictors’ coefficient was retained [19], as there is evidence that it is a confounder of important effects (on the outcome variable). The selected predictors were also used for O16-42. For O16, the socio-economic status was indicated using father’s social class instead of using the participant’s job category. Additionally, in O16, exercise at age 33 was not used since this variable was not available at age 16.
Ethics approval for our study was obtained from the Ethics committee of the Nursing Studies department of the School of Health in Social Studies of the University of Edinburgh. The Ethics application ID is 22-23NUST021. This study did not involve collection of data in any form. All the data used in this study was obtained from the publicly available NCDS longitudinal dataset. This data is publicly available from the UK Data Service and the use of this data does not require obtaining consent from the participants of the NCDS study. The NCDS is 62 years old and details on the consent protocol followed by the NCDS can be found here: https://cls.ucl.ac.uk/wp-content/uploads/2017/07/NCDS-Ethical-review-and-Consent-2014.pdf.
Results
Exploratory analyses
Fig 2 (Sankey diagram) shows a striking difference in the BMI category profiles at 16 and 42 years of age. Interestingly, the proportion of individuals who were overweight at 42(36.96%) is similar to that of those who were of healthy weight (39.35%) at the same age. In contrast, at age 16, the majority of individuals were of healthy weight (52.43%), and a relatively small proportion of individuals were overweight (4.23%).
Sankey diagram depicting the BMI categories across the two sweeps corresponding to 16 and 42 years of age.
Table 2 provides summaries of the variables used in our study with percentages per level (and sample size). From Table 2 we note that for model [O16-42] in terms of Exercise frequency at age 33, the higher percentages of individuals who did not develop obesity were for those who exercised 4-5 times a week or every day.
Table 2: Descriptives for the variables used in the study.
Models
Here we present in Fig 3, the results for the three models [O16], [O16-42], and [O42] considered in this study. Table 3–5 provide details on the odds ratios (OR) for each model. Note that the outcome variable for [O16] is being overweight or obese at 16 years of age, that for [O16-42] is being healthy at 16 years of age but overweight, obese or severely obese at 42 years of age, that for [O42] is being overweight, obese or severely obese at age 42.
Table 3: Results for Obesity at 16 years of age (n = 5831, 33.261% of N).
Table 4: Results for Obesity at 42 years old for individuals healthy/underweight at 16 years old (n = 4767, 27.192% of N).
Table 5: Results for obesity at 42 years old (n = 6933, 39.547% of N).
Forest plots for (left) odds of being overweight/obese at age 16 denoted as [O16], (middle) odds of being overweight/obese/severely obese at age 42 for those who were healthy/underweight at age 16 denoted as [O16-42], and (right) odds of being obese/overweight at age 42, denoted as [O42].
The associated sample sizes for these models are: 5,831, 4,767, and 6,933 respectively, as described in Fig 1
We have provided results for the full model in S15 Table in S1 File.
Discussion
We begin the discussion by addressing the study’s research questions.
Research question 1 [O16]: We found associations between sex, maternal factors (BMI, smoking, mode of delivery), father’s socio-economic position and being overweight at 16 years of age (in 1974). Higher odds ratios (see Table 3) were observed for females, for increasing maternal age, for mothers who smoked 10 cigarettes or more per day (compared to those who did not smoke), for caesarean-labour-delivery (compared to normal delivery), and for maternal obesity (compared to the mothers being healthy or underweight). The odds ratio (4.33, CI 3.26 to 5.71) for maternal obesity is the largest amongst the variables considered. Father’s socioeconomic position showed modest protective effects for “Manual” and “Professional” categories compared to “Farming” category, and birth order was not associated with obesity at 16 years of age.
With regards to the finding on caesarean-labour-delivery, one possible explanation is that mothers who are overweight and with gestational diabetes often require C-sections and their babies are likely to be overweight. This predisposes the babies to later weight gain [20–22].
Research question 2 [O16-42]: Similar risk factors were associated with incident obesity between 16 and 42 years of age, albeit with generally slightly smaller odds ratio, compared to those described above for obesity at 16 years of age, although the association with sex changed direction so that being male was a risk factor for incident obesity between 16 and 42 years of age. An additional risk factor, exercise frequency at age 33 (with a reference/comparison group of “No exercise”), showed clinical and statistically significant associations (see Table 4) with incident obesity, in a close-to-monotonic dose-response pattern (OR for 2-3 days a week of exercise 0.74, CI 0.58 to 0.94; OR for 4-5 days a week of exercise 0.59, CI 0.39 to 0.85), similarly to findings in previous studies [23–25].
Research question 3 [O42]: We note that the estimates for [O16-42] and [O42] for early life and parental risk factors were similar -this may be largely because obesity was so rare at age 16 in 1974, that the adult-onset cases consist mostly of incident obesity between 16 and 42 years of age.
Mother’s BMI and maternal smoking remain important risk factors in O16-42 for adult-onset obesity, between ages 16 and 42 years of age. The persistent importance of maternal factors well into their children’s adult life illustrates the “long reach” of intergenerational influences. The effect of mother’s BMI for example is the largest (OR 3.90, CI 2.69 to 4.03). Details are provided in Table 5.
Geoffrey Rose, considered by some to be the father of modern chronic disease epidemiology, provided a conceptual framework of direct relevance to our findings. In his landmark paper [26] “Sick Individuals and Sick Populations” he provided sage advice to researchers looking for the causes of widespread changes in the prevalence of chronic diseases, such obesity (a topic he addressed directly, even though the modern pandemic was only beginning at that time.) His advice was to suspect a major role for “upstream” risk factors operating at the level of entire societies/communities and to “seek the causes of incidence (at the population level) rather than the causes of cases (at the individual level)”.
Our findings support this strategy in future research into the aetiology of obesity. Specifically, we found remarkably similar relative risks for several early-life risk factors for later-life obesity, spanning a period starting before the obesity pandemic really began (at least in the UK) to well after its peak. Those early-life risk factors predicted, with persistently powerful relative risks, both prevalent obesity at age 16 (rather uncommon in this cohort) and also incident obesity between ages 16 and 42. This finding suggests that such individual-level risk factors are unlikely to explain the pandemic itself. However, to illuminate the role in the pandemic of society/community-level risk factors, those would have to be measured, across societies/communities with varying patterns of emergence for the pandemic over recent decades – ideally in a multi-level study design.
Such designs are not typical of classical epidemiology. Indeed, the British birth cohort we analysed was aimed at the measurement and analysis of only individual- level, not society/community-level risk factors for the many health and development outcomes it collected. If one were to follow Rose’s advice, significant additional data collection in such a cohort study would be needed, reflecting changes in relevant society/community-level risk factors – such as the profoundly transformed nature of food production, marketing and distribution systems between the 1970s through to the early 2000s. We suspect such a novel study design, because it would have to span global national settings with major variation in how and when the pandemic began, would have to be international in scope, perhaps sampling a set of societies with contrasting pandemic patterns of timing – a daunting prospect, but a project we suspect Rose would strongly support.
Conclusion
The main strengths of this study are that our paper is unique in showing that those predictors were just as powerful (and prevalent) in the era before the current obesity pandemic began. This lends great credibility to a central idea of Geoffrey Rose.
Our work supplements previous studies [8,12,27] showing that maternal influences such as BMI, are important predictors of obesity across four decades of offsprings’ lives. Our study also documents persistent sociodemographic influences on obesity over the life course. Additionally, our study is providing a rare glimpse into socio-demographic and early-life influences on obesity onset before and after the appearance of the obesogenic environment in the UK.
One limitation is that regrettably, birthweight data collected in 1958 on the NCDS cohort could not include ultrasound estimates of gestational age, making it impossible to separate premature from small-for-gestational-age newborns. After preliminary analyses in which raw birthweight and birthweight adjusted for the mother’s estimated last menstrual period showed no association with the outcomes under study, we decided not to use the birthweight data in our final analyses, despite past studies showing a link between fetal weight and adult obesity.
As indicated in the Introduction, the only study identified [8] which assesses early-life risk factors for obesity in the 1958 British Birth Cohort considers a much narrower range of predictors than our study. Our study confirms the major finding in this paper, pinpointing maternal factors as being important in predicting adult-onset obesity. Our study, however, reveals that other factors such as father’s social class and exercise frequency (at 33 years of age) are also important. The identification of exercise frequency as an important predictor resonates with current public health efforts at promoting wellbeing through physical activity.
Our work has highlighted the importance for future work to investigate the impact of sociodemographic and early-life biological/familial factors’ association with adult obesity, in a cohort whose childhood occurred prior to onset of secular trends in increasing obesity prevalence among both children and adults. The importance for future work of investigating differences in risk factors between obesity in early life, versus adult onset, and especially how this plays out so differently in males and females, has also been shown. Finally, the need for investigating the importance of cultural/environmental conditions in epidemiological studies, not just individual-level characteristics/exposures has been clearly illustrated. Public health officials and researchers (in the 1970s and 1980s) did not anticipate subsequent massive, population-level increases in the prevalence of obesity/overweight, let alone conceptualize the then-emerging obesogenic environment as a key driver of that pandemic. Therefore, it is not surprising that existing cohort datasets from that period do not include credible measures of the “dose,” of specific obesogenic influences within that environment, to which individual subjects were exposed.
The impact of dietary habits on the onset of obesity is one aspect not covered in our analyses. The quality of the available dietary data in the NCDS did not allow for this. Similarly, our analyses did not include the impact of personality traits. In terms of future research, we are planning to conduct a larger study which examines the impact of sociodemographic predictors on the onset of obesity during the 2020s. This study would allow us to determine how different those predictors are in the present era to those observed in the NCDS and inform public health policy regarding health promotion and protection. Another aspect that we will be investigating is the impact of “place”: whether the area where one’s lives in the UK impacts their likelihood of being obese.
This study has identified early-life (and potentially more “biologically mediated”) risk factors for obesity which have been sustained in their importance, for a cohort whose childhood preceded the pandemic, suggesting roles for both biology and environment in obesity time trends.
Supporting information
S1 TableNCDS data sweeps and corresponding years.(DOCX)
S2 TableVariables used in modelling from NCDS.(DOCX)
S1 TextData transformations and processing.(DOCX)
S3 TableTransformations for the smoking variable.(DOCX)
S2 TextMethod of Actual Delivery.(DOCX)
S3 TextFather, male head’s socio-economic group (GRO 1966).(DOCX)
S4 TableTransformation of father’s occupation.(DOCX)
S4 TextMother’s BMI at birth.(DOCX)
S5 TextCurrent Job – Social Class.(DOCX)
S5 TableTransformations for job categories.(DOCX)
S1 FigComparison of BMI categories.(DOCX)
S2 FigComparison of exercise frequency.(DOCX)
S3 FigComparison of mother’s BMI.(DOCX)
S6 TableModel diagnostics.(DOCX)
S7 TableResults for the full model for O42 (with all variables).(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Carrasquilla G, Ängquist L, Sørensen T, Kilpeläinen T, Loos R. Child-to-adult body size change and risk of type 2 diabetes and cardiovascular disease. Diabetologia. 2023:1–10.10.1007/s 00125-023-06058-4PMC 1095491938085289 · doi ↗ · pubmed ↗
- 2Doi L, Williams A, Frank J. How has child growth around adiposity rebound altered in Scotland since 1990 and what are the risk factors for weight gain using the Growing Up in Scotland birth cohort 1? BMC Public Health. 2016;16:1–9. doi: 10.1186/s 12889-016-2720-527737667 PMC 5064913 · doi ↗ · pubmed ↗
- 3Hughes CA, Ahern AL, Kasetty H, Mc Gowan BM, Parretti HM, Vincent A, et al. Changing the narrative around obesity in the UK: a survey of people with obesity and healthcare professionals from the ACTION-IO study. BMJ Open. 2021;11(6):e 045616. doi: 10.1136/bmjopen-2020-045616 34193488 PMC 8246368 · doi ↗ · pubmed ↗
- 4Koliaki C, Dalamaga M, Liatis S. Update on the Obesity Epidemic: After the Sudden Rise, Is the Upward Trajectory Beginning to Flatten? Curr Obes Rep. 2023;12(4):514–27. doi: 10.1007/s 13679-023-00527-y 37779155 PMC 10748771 · doi ↗ · pubmed ↗
- 5Kivimäki M, Kuosma E, Ferrie JE, Luukkonen R, Nyberg ST, Alfredsson L, et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. 2017;2(6):e 277–85. doi: 10.1016/S 2468-2667(17)30074-9 28626830 PMC 5463032 · doi ↗ · pubmed ↗
- 6Power C, Elliott J. Cohort profile: 1958 British birth cohort (national child development study). International Journal of Epidemiology. 2006;35(1):34–41.16155052 10.1093/ije/dyi 183 · doi ↗ · pubmed ↗
- 7Potter C, Ulijaszek S. Predicting adult obesity from measures in earlier life. J Epidemiol Community Health. 2013;67(3):223–4. doi: insert_doi_here 10.1136/jech-2012-20197824052512 · doi ↗ · pubmed ↗
- 8de Kroon MLA, Renders CM, van Wouwe JP, Hirasing RA, van Buuren S. Identifying young children without overweight at high risk for adult overweight: the Terneuzen Birth Cohort. Int J Pediatr Obes. 2011;6(2–2):e 187-95. doi: 10.3109/17477166.2010.526220 21091137 · doi ↗ · pubmed ↗