The effect of HA380 blood adsorption on patients with acute infective endocarditis undergoing cardiac surgery: a retrospective study
Xiao Jiefei, Cao Lu, Shi Han, Shi Yongxu, Mo Shaoyan, Qin Kai, Li Yonghua, Zhu Yanling, Jiang Yumei, Rong Jian

TL;DR
This study examined whether HA380 blood adsorption improves outcomes for patients with infective endocarditis undergoing surgery, finding no significant reduction in postoperative sepsis but a shorter hospital stay.
Contribution
The study provides new evidence on the clinical impact of HA380 blood adsorption in acute infective endocarditis surgery.
Findings
HA380 use was not associated with a lower incidence of postoperative sepsis.
Patients receiving HA380 had a significantly shorter postoperative hospital stay.
HA380 patients showed lower fibrinogen levels and a higher albumin-to-fibrinogen ratio.
Abstract
Sepsis is a major cause of ICU admission and mortality in patients with infective endocarditis patients. This study aimed to explore the effect of intraoperative HA380 blood adsorption on surgical outcomes in infective endocarditis patients, given its ability to adsorb inflammatory factors. We retrospectively analyzed the clinical data of patients who underwent surgical treatment for infective endocarditis at our hospital. After propensity score matching, eligible patients were matched in a 1:1 ratio between HA380 users and non-users. The primary endpoint was the incidence of postoperative sepsis, while secondary outcomes included ICU stay, postoperative hospital stay, and the need for CRRT, IABP, and ECMO therapies. Laboratory results were compared at 24, 48, and 72 h postoperatively. A total of 148 patients were included in the analysis. After 1:1 matching, 39 pairs were further…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
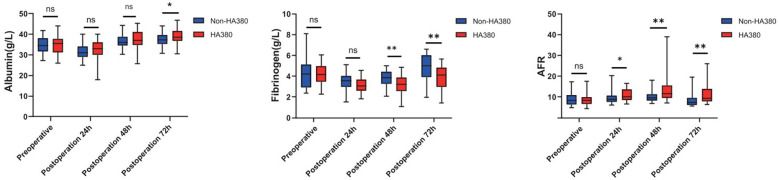 Figure 1
Figure 1| Preoperative characteristics and surgical information | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | After PSM | |||||
| Non-HA380 | HA380 | Non-HA380 | HA380 | |||
| ( | ( | ( | ( | |||
| Demographic information | ||||||
| Age, years | ||||||
| Mean (SD) | 46.9 (15.7) | 49.5 (15.0) | 0.342 | 48.1 (16.2) | 48.2 (14.7) | 0.983 |
| Gender | ||||||
| Female | 26 (24.5%) | 12 (28.6%) | 0.765 | 12 (30.8%) | 12 (30.8%) | 1 |
| Male | 80 (75.5%) | 30 (71.4%) | 27 (69.2%) | 27 (69.2%) | ||
| BMI, kg/m2 | ||||||
| Mean (SD) | 21.1 (4.17) | 20.5 (3.45) | 0.408 | 20.3 (3.40) | 20.4 (3.40) | 0.836 |
| Preoperative comorbidities | ||||||
| Diabetes | ||||||
| 10 (9.4%) | 8 (19.0%) | 0.182 | 3 (7.7%) | 5 (12.8%) | 0.709 | |
| Pulmonary disease | ||||||
| 16 (15.1%) | 13 (31.0%) | 0.0498* | 10 (25.6%) | 10 (25.6%) | 1 | |
| Nephropathy | ||||||
| 8 (7.5%) | 5 (11.9%) | 0.601 | 3 (7.7%) | 3 (7.7%) | 1 | |
| Preoperative tracheal intubation | ||||||
| 5 (4.7%) | 5 (11.9%) | 0.227 | 1 (2.6%) | 3 (7.7%) | 0.608 | |
| Preoperative score | ||||||
| NYHA | ||||||
| Ⅱ | 38 (35.8%) | 17 (40.5%) | 0.00439* | 17 (43.6%) | 17 (43.6%) | 0.0955 |
| III | 52 (49.1%) | 10 (23.8%) | 17 (43.6%) | 10 (25.6%) | ||
| Ⅳ | 16 (15.1%) | 15 (35.7%) | 5 (12.8%) | 12 (30.8%) | ||
| Euroscore II | ||||||
| Mean (SD) | 4.09 (3.84) | 8.41 (14.1) | 0.0571 | 3.93 (3.92) | 6.08 (11.6) | 0.278 |
| APACHEII | ||||||
| Mean (SD) | 3.71 (3.19) | 5.52 (5.67) | 0.0558 | 3.67 (2.67) | 4.72 (5.02) | 0.253 |
| Preoperative blood transfusion and medication | ||||||
| Blood products transfusion preoperative | ||||||
| 10 (9.4%) | 6 (14.3%) | 0.573 | 3 (7.7%) | 4 (10.3%) | 1 | |
| Gamma globulin transfusion preoperative, g | ||||||
| Mean (SD) | 1.37 (8.38) | 4.52 (16.4) | 0.242 | 1.28 (6.56) | 1.41 (7.34) | 0.935 |
| Preoperative culture | ||||||
| Blood culture | ||||||
| Gram-positive cocci(exclude staphylococcus) | 41 (38.7%) | 13 (31.0%) | 0.757 | 13 (33.3%) | 13 (33.3%) | 0.718 |
| Gram-negative bacilli | 3 (2.8%) | 2 (4.8%) | 2 (5.1%) | 2 (5.1%) | ||
| Abiotrophia | 2 (1.9%) | 2 (4.8%) | 0 (0%) | 2 (5.1%) | ||
| Staphylococcus | 5 (4.7%) | 3 (7.1%) | 2 (5.1%) | 1 (2.6%) | ||
| Resistant organism | 2 (1.9%) | 2 (4.8%) | 1 (2.6%) | 2 (5.1%) | ||
| Fungus | 1 (0.9%) | 0 (0%) | 1 (2.6%) | 0 (0%) | ||
| Surgical information | ||||||
| Surgry | ||||||
| Aortic valve and/or ASD/VSD | 29 (27.4%) | 11 (26.2%) | 0.52 | 11 (28.2%) | 10 (25.6%) | 0.788 |
| Mitral valve and/or ASD/VSD | 47 (44.3%) | 20 (47.6%) | 19 (48.7%) | 19 (48.7%) | ||
| Tricuspid valve and/or ASD/VSD | 4 (3.8%) | 4 (9.5%) | 2 (5.1%) | 4 (10.3%) | ||
| Multiple valves and/or ASD/VSD | 24 (22.6%) | 7 (16.7%) | 6 (15.4%) | 6 (15.4%) | ||
| Valve replacement and CABG | 2 (1.9%) | 0 (0%) | 1 (2.6%) | 0 (0%) | ||
| Redo | ||||||
| 8 (7.5%) | 2 (4.8%) | 0.806 | 1 (2.6%) | 2 (5.1%) | 1 | |
| Perfusion time, min | ||||||
| Mean (SD) | 159 (74.0) | 152 (73.5) | 0.601 | 136 (56.4) | 149 (75.2) | 0.375 |
| Aortic clamping time, min | ||||||
| Mean (SD) | 94.7 (46.8) | 88.7 (45.5) | 0.473 | 80.8 (37.6) | 86.5 (46.0) | 0.555 |
| Endpoint | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | After PSM | |||||
| Non-HA380 | HA380 | Non-HA380 | HA380 | |||
| ( | ( | ( | ( | |||
| Sepsis | ||||||
| 19 (17.9%) | 6 (14.3%) | 0.772 | 8 (20.5%) | 6 (15.4%) | 0.724 | |
| Time from operation to discharge days, d | ||||||
| Mean (SD) | 24.6 (13.3) | 23.2 (12.6) | 0.549 | 28.1 (14.1) | 21.2 (10.3) | |
| Length of stay, d | ||||||
| Mean (SD) | 37.5 (16.1) | 34.1 (13.5) | 0.204 | 40.3 (18.2) | 32.2 (11.0) | |
| ICU stay time, h | ||||||
| Mean (SD) | 70.4 (138) | 136 (310) | 0.193 | 79.2 (171) | 56.3 (81.6) | 0.452 |
| Ventilator use time, h | ||||||
| Mean (SD) | 34.9 (82.9) | 91.2 (255) | 0.168 | 28.2 (61.8) | 29.2 (67.6) | 0.944 |
| CRRT | ||||||
| 11 (10.4%) | 9 (21.4%) | 0.132 | 7 (21.9%) | 3 (7.7%) | 0.289 | |
| IABP | ||||||
| 9 (8.5%) | 3 (7.1%) | 1 | 3 (7.7%) | 3 (7.7%) | 1 | |
| ECMO | ||||||
| 2 (1.9%) | 1 (2.4%) | 1 | 2 (5.1%) | 1 (2.6%) | 1 | |
| SOFA score and laboratory examination | ||||||
|---|---|---|---|---|---|---|
| Unadjusted | After PSM | |||||
| Non-HA380 | HA380 | Non-HA380 | HA380 | |||
| ( | ( | ( | ( | |||
| Before surgery | ||||||
| SOFA | ||||||
| Mean (SD) | 1.58 (2.17) | 2.14 (4.43) | 0.439 | 1.00 (1.95) | 1.77 (4.15) | 0.299 |
| ALT, U/L | ||||||
| Mean (SD) | 33.4 (54.5) | 29.0 (23.2) | 0.498 | 24.0 (17.2) | 26.4 (16.7) | 0.537 |
| ST, U/L | ||||||
| Mean (SD) | 34.6 (45.6) | 37.1 (33.9) | 0.719 | 29.4 (19.5) | 33.8 (26.6) | 0.409 |
| TNT, ug/L | ||||||
| Mean (SD) | 0.829 (4.67) | 0.145 (0.214) | 0.136 | 0.645 (2.99) | 0.134 (0.211) | 0.089 |
| BNP, pg/ml | ||||||
| Mean (SD) | 2,780 (5,420) | 4,140 (7,900) | 0.312 | 1,280 (1,380) | 3,250 (6,930) | 0.089 |
| PCT, ng/ml | ||||||
| Mean (SD) | 2.49 (12.9) | 1.10 (1.02) | 0.275 | 1.21 (1.08) | 1.11 (1.03) | 0.704 |
| WBC, ×109/L | ||||||
| Mean (SD) | 8.94 (3.92) | 9.85 (4.80) | 0.279 | 8.59 (3.94) | 9.87 (4.93) | 0.212 |
| Hb, g/L | ||||||
| Mean (SD) | 109 (21.2) | 104 (19.8) | 0.174 | 108 (18.6) | 105 (19.9) | 0.57 |
| 24 h after surgery | ||||||
| SOFA | ||||||
| Mean (SD) | 2.43 (4.82) | 1.86 (3.30) | 0.407 | 2.97 (5.70) | 1.92 (3.42) | 0.327 |
| ALT, U/L | ||||||
| Mean (SD) | 64.3 (151) | 125 (604) | 0.524 | 34.8 (22.3) | 132 (627) | 0.335 |
| AST, U/L | ||||||
| Mean (SD) | 132 (280) | 459 (2,430) | 0.389 | 72.1 (37.3) | 489 (2,520) | 0.309 |
| TNT, ug/L | ||||||
| Mean (SD) | 1.97 (5.42) | 1.52 (1.78) | 0.456 | 1.25 (0.899) | 1.56 (1.84) | 0.282 |
| BNP, pg/ml | ||||||
| Mean (SD) | 2,520 (6,100) | 2,380 (4,130) | 0.871 | 1,500 (3,190) | 2,110 (4,090) | 0.484 |
| PCT, ng/ml | ||||||
| Mean (SD) | 2.42 (10.9) | 0.611 (0.983) | 0.094 | 1.79 (6.62) | 0.532 (0.904) | 0.24 |
| WBC, ×109/L | ||||||
| Mean (SD) | 15.8 (6.59) | 15.1 (6.41) | 0.554 | 14.2 (6.38) | 15.4 (6.49) | 0.353 |
| Hb, g/L | ||||||
| Mean (SD) | 98.4 (13.2) | 95.1 (12.3) | 0.157 | 97.8 (14.1) | 95.8 (12.3) | 0.524 |
| 48 h after surgery | ||||||
| SOFA | ||||||
| Mean (SD) | 1.91 (3.31) | 1.40 (2.67) | 0.34 | 2.28 (3.74) | 1.49 (2.75) | 0.289 |
| AST, U/L | ||||||
| Mean (SD) | 164 (402) | 70.9 (72.4) | 70.0 (51.5) | 72.2 (74.9) | 0.876 | |
| TNT, ug/L | ||||||
| Mean (SD) | 1.57 (4.23) | 1.26 (2.87) | 0.612 | 0.936 (1.64) | 1.28 (2.98) | 0.529 |
| BNP, pg/ml | ||||||
| Mean (SD) | 4,320 (7,600) | 3,760 (4,800) | 0.598 | 3,360 (4,850) | 3,510 (4,860) | 0.898 |
| PCT, ng/ml | ||||||
| Mean (SD) | 6.00 (18.3) | 1.97 (2.04) | 6.30 (21.9) | 1.77 (1.76) | 0.199 | |
| WBC, ×109/L | ||||||
| Mean (SD) | 14.2 (6.03) | 13.3 (5.58) | 0.38 | 13.6 (5.10) | 13.5 (5.59) | 0.966 |
| Hb, g/L | ||||||
| Mean (SD) | 93.0 (14.2) | 91.4 (12.4) | 0.496 | 96.4 (13.5) | 91.4 (12.7) | 0.091 |
| 72 h after surgery | ||||||
| SOFA | ||||||
| Mean (SD) | 0.96 (1.49) | 0.76 (0.75) | 0.167 | 1.21 (1.78) | 0.767 (0.77) | 0.167 |
| ALT, U/L | ||||||
| Mean (SD) | 69.6 (178) | 23.8 (18.6) | 24.4 (22.3) | 24.4 (19.1) | 1 | |
| AST, U/L | ||||||
| Mean (SD) | 140 (353) | 51.7 (50.5) | 51.1 (40.9) | 51.4 (51.9) | 0.977 | |
| TNT, ug/L | ||||||
| Mean (SD) | 0.926 (1.73) | 0.894 (2.30) | 0.936 | 0.628 (0.902) | 0.920 (2.39) | 0.481 |
| BNP, pg/ml | ||||||
| Mean (SD) | 5,990 (10,400) | 4,640 (5,210) | 0.295 | 4,840 (6,420) | 4,590 (5,380) | 0.859 |
| PCT, ng/ml | ||||||
| Mean (SD) | 110 (581) | 39.8 (43.9) | 0.222 | 52.3 (43.3) | 42.6 (44.4) | 0.328 |
| WBC, ×109/L | ||||||
| Mean (SD) | 17.8 (7.19) | 16.4 (6.28) | 0.254 | 17.2 (7.27) | 16.7 (6.31) | 0.758 |
| Hb, g/L | ||||||
| Mean (SD) | 91.4 (12.9) | 88.8 (11.8) | 0.235 | 93.5 (13.8) | 89.0 (12.2) | 0.109 |
| PLT, ×109/L | ||||||
| Mean (SD) | 138 (60.9) | 143 (67.0) | 0.667 | 139 (56.3) | 150 (64.2) | 0.436 |
- —Beijing Huikang Charity Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Sepsis Diagnosis and Treatment · Streptococcal Infections and Treatments
Background
1
The incidence of infective endocarditis varies by region, ranging from 2 to 10 cases per 100,000 individuals (1–3). Despite significant advancements in diagnosis, treatment, and perioperative management, the in-hospital mortality rate remains high, exceeding 20% (4–7). Surgical intervention is the primary approach for valve reconstruction in infective endocarditis, and in-hospital mortality is closely associated with sepsis-induced multiple organ dysfunction syndrome (MODS) (8, 9).Sepsis-related inflammatory factors are believed to trigger an excessive systemic inflammatory response (SIRS), which can lead to MODS (10). Therefore, reducing inflammatory factors through intraoperative blood adsorption is considered a promising strategy. While the HA380 adsorption filter has demonstrated efficacy in vitro (4, 11–14), its in vivo effectiveness remains a subject of debate. This study aims to evaluate the impact of HA380 blood adsorption on surgical outcomes in patients with infective endocarditis.
Materials and methods
2
Patients
2.1
This single-center, retrospective observational study analyzed data from 148 patients with infective endocarditis who underwent cardiac surgery at our hospital between January 1, 2019, and March 1, 2022.
Inclusion criteria: Patients with acute infective endocarditis undergoing valve reconstruction surgery were included.
Exclusion criteria: (1) Inability to undergo valve reconstruction surgery. (2) Incomplete clinical information. (3) Postoperative pathological results indicating non-bacterial endocarditis, such as marantic endocarditis related to malignancy or Libman-Sacks endocarditis associated with systemic lupus erythematosus (15).
Outcome
2.2
The primary outcome of this study was the incidence of postoperative sepsis, with sepsis diagnosed based on the third international consensus definition (16, 17). Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Patients with an increase in Sequential Organ Failure Assessment (SOFA) score of ≥2 and suspected or proven infection were considered to have sepsis.
Secondary outcomes included length of stay, postoperative hospital stay, use of continuous renal replacement therapy (CRRT), intra-aortic balloon pump (IABP) and extracorporeal membrane oxygenation (ECMO).
Data collection
2.3
General clinical data of patients were collected, such as patient gender, age, medical history, preoperative laboratory test results. Intraoperative data included surgical approach, intraoperative transfusion and blood product usage, and cardiopulmonary bypass-related data (aortic cross-clamp time, hypothermic time). Postoperative data included the occurrence of sepsis, length of hospital stay, ICU stay, major postoperative complications, use of CRRT or ECMO, and postoperative continuous laboratory test results.
Use of HA380
2.4
The HA380 blood perfusion device was integrated with the cardiopulmonary bypass (CPB) circuit for blood perfusion. Venous blood initially entered the reservoir and subsequently flowed into the oxygenator, driven by the pump. After oxygenation, the majority of oxygenated blood was directed into the arterial circulation for perfusion, with approximately 700 ml/min (14%–18%) undergoing blood filtration through the HA380 blood perfusion device. The filtered blood was then returned to the reservoir and mixed with venous blood. No additional equipment was required for this process.
Data analysis
2.5
Statistical analysis was performed using SPSS software, and propensity score matching (PSM) analysis was conducted using the R language. The propensity score (PS) was derived from a multivariate logistic regression model that estimated the group affiliation (HA380 vs. non-HA380) based on variables such as gender, age, medical history, preoperative laboratory test results, and more. The nearest neighbor algorithm was employed for 1:1 PSM to minimize potential confounding effects and achieve covariate balance between the groups. Given the high mortality rate associated with infective endocarditis but its relatively low incidence, a caliper was not applied to maximize the use of patients who received HA380. To After matching, comparisons between groups were made using the paired t-test or rank sum test for continuous variables and the McNemar test for categorical variables. A p-value of <0.05 was considered statistically significant.
Ethics
2.6
This study was designed in accordance with the principles outlined in the the Helsinki Declaration and complied with the regulations set forth in the Law on Medical Research Involving Human Subjects and the Good Clinical Practice (GCP) guidelines. This study was approved by the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University. The relevant document numbers was 45362023653.
Results
3
Baseline characteristics
3.1
From January 1, 2019, to March 1, 2022, a total of 148 patients with definitive infective endocarditis who underwent surgical therapy with cardiopulmonary bypass were included in our study. The cohort consisted of 110 males and 38 females, with a mean age of 48.2 years. Preoperative blood cultures were negative in 72 cases and positive in 76 cases. Among these patients, 106 did not receive HA380, while 42 received HA380. The period of HA380 use ranged from September 1, 2020 and March 1, 2022. After PSM, 78 patients were evenly distributed into the HA380 group and the non-HA380 group. The baseline characteristics of the patients are detailed in Table 1. The proportion of patients with preoperative lung disease was higher in the HA380 group compared to the non-HA380 group (31% vs. 15.1%, p = 0.049). The preoperative albumin level was lower in the HA380 group (34.5 vs. 36.2 g/L, p = 0.048). The difference in New York heart association (NYHA) functional class scores between the two groups was statistically significant (HA380 vs. non-HA380, NYHA II 35.8% vs. 40.5%; NYHA III 49.1% vs. 23.8%; NYHA IV 15.1% vs. 35.7%). No other clinical variables showed statistically significant differences. However, after PSM, none of the baseline differences remained statistically significant.
Endpoint events
3.2
The summary of the endpoint events is presented in Table 2.
Primary outcome
3.2.1
Before PSM, the incidence of postoperative sepsis did not show a statistically significant difference (17.9% vs. 14.3%, p = 0.722). After PSM, no statistically significant difference was found between the HA380 group and the control group (15.4% vs. 20.5%, p = 0.724).
Secondary outcomes
3.2.2
Before PSM, there were no significant differences in time from operation to discharge (24.6 vs. 23.2 days, p = 0.549), length of stay (37.5 vs. 34.1 days, p = 0.204), ICU stay time (70.4 vs. 136 h, p = 0.193) and Ventilator use time (34.9 vs. 91.2 h, p = 0.168). Additionally, there were no differences in the use of CRRT (10.4% vs. 21.4%, p = 0.132), IABP (8.5% vs. 7.1%, p = 1.0) or ECMO (1.9% vs. 2.4%, p = 1.0) therapy between the two groups. After PSM, Time from operation to discharge was shorter in the HA380 group (21.2 vs. 28.1, p = 0.014), as well as length of stay (32.2 vs. 40.3, p = 0.024). There were no differences in ICU stay time (79.2 vs. 56.3 h, p = 0.452) and ventilator use time (28.2 vs. 29.2 h, p = 0.994), CRRT (21.9% vs. 7.7%, p = 0.289), IABP (7.7% vs. 7.7%, p = 1.0) or ECMO (5.1% vs. 2.6%, p = 1) therapy between the two groups.
SOFA scores and postoperative laboratory results
3.3
We collected relevant SOFA scores and postoperative laboratory results of the patients, as shown in Table 3. The difference in postoperative SOFA scores between the two groups was not statistically significant (24 h: 2.97 vs. 1.92, p = 0.327; 48 h: 2.28 vs. 1.49, p = 0.289; 72 h 1.21 vs. 0.767, p = 0.167). In the HA380 group, fibrinogen levels were significantly lower than in the non-HA380 group (24 h: 3.15 vs. 3.51, p = 0.053; 48 h: 3.14 vs. 3.82, p = 0.002; 72 h: 3.94 vs. 4.80, p = 0.006). Conversely, the albumin-to-fibrinogen ratio (AFR) was significantly higher in the HA380 group compared to the non-HA380 group (24 h: 10.9 vs. 9.53, p = 0.038; 48 h: 13.4 vs. 10.0, p = 0.005; 72 h: 11.1 vs. 8.57, p = 0.009) (Figure 1). The differences in other laboratory results were not statistically significant.
Boxplot of albumin, fibrinogen and AFR throughout the perioperative period.
Discussion
4
CPB may induce a sudden release of inflammatory cytokines. Theoretically, the application of HA380 could facilitate the adsorption of inflammatory mediators, thereby contributing to improved postoperative outcomes (14, 18). However, in our study, no statistically significant difference in the incidence of sepsis was observed between the HA380 and non-HA380 groups. Additionally, compared to the non-HA380 group, the HA380 group exhibited shorter postoperative hospital stay, shorter total hospital stay, lower fibrinogen level and a higher AFR.
Wang et al. found that although the serum IL-6 levels increased more rapidly in the control group than in the HA380 group after surgery, the incidence of postoperative acute kidney injury(AKI) and acute respiratory distress syndrome(ARDS) was lower in the HA380 group. However, the incidence of other postoperative complications, including ventilation time, ICU stay, hospital stay, and in-hospital mortality were not significantly different between the two groups (14). While in a 2022 study, patients in the HA380 group had significantly lower IL-6 levels, required less vasopressin, had shorter mechanical ventilation duration, and had shorter ICU stays. The authors concluded that HA380 was effective in reducing SIRS and promoting postoperative recovery (19). In studies of blood adsorption using other perfusion devices, several studies have reported no differences in the incidence of sepsis, ICU length of stay, ventilator treatment, and 30-day mortality rate following blood adsorption. Haidari et al. indicated that the sepsis-related mortality rate was lower in patients who underwent blood adsorption (34% vs. 43%, p = 0.041), while there were no differences in the incidence of sepsis or in-hospital mortality (11, 20, 21). Our study failed to demonstrate that the use of HA380 could reduce the incidence of postoperative sepsis. Despite shorter hospital stays, there were no differences in incidence of sepsis, ICU length of stay, ventilator use, CRRT, IABP or ECMO.
Blood adsorption effectively lowers fibrinogen levels, as evidenced by a significant reduction observed at the end of the procedure (22).Studies have linked lower fibrinogen levels in sepsis patients to higher mortality rates (23, 24), with thresholds below 1.6 g/L or 2.0 g/L showing a stronger correlation (25, 26). In the early stages of sepsis, fibrinogen levels rise, exacerbating inflammation (27, 28), while albumin levels typically decrease (29), reflecting the complex interplay of inflammation. As a novel biomarker, AFR has shown utility in various conditions, including cancer and autoimmune diseases (30–32). While cytokine adsorption has the potential to regulate immune responses, its clinical advantages remain poorly defined. Our research indicated significant reductions in fibrinogen levels and increases in AFR in the HA380 group; however, these findings did not translate into improved clinical outcomes. Consequently, the clinical significance of these results requires further investigation in the future.
Some reports suggest that propensity score matching (PSM) can reduce or even eliminate the impact of selection bias in both prospective and retrospective studies (33, 34). In this retrospective study, PSM was employed to match baseline characteristics, including demographic data, preoperative complications, medications, laboratory tests, and surgical details, aiming to reduce differences in disease severity and physical condition between groups. However, the matching for patients using HA380 was not strictly adjusted for confounding factors. Despite PSM's partial adjustment, the impact of unknown confounders persists. Additionally, the study did not collect or analyze more cytokines, such as interleukins and interferons, nor did it observe their specific changes.
Our study has several limitations. First, as a single-center retrospective study, it is limited by a relatively small sample size and inherent internal biases. Second, although PSM analysis was employed to balance baseline data, further multicenter, large-sample prospective clinical studies are required to validate our conclusions. Additionally, more detailed designs for laboratory tests should be implemented, such as collecting simultaneous data on inflammatory factors in patients, to better elucidate the specific effects and mechanisms of HA380.
Conclusion
5
The use of HA380 in surgical interventions for infective endocarditis did not result in a decreased incidence of postoperative sepsis. Although the HA380 group showed a shorter postoperative hospital stay, shorter total hospital stay, lower fibrinogen level, and a higher AFR, its overall effectiveness still requires further validation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Olmos C Vilacosta I Fernández-Pérez C Bernal JL Ferrera C García-Arribas D The evolving nature of infective endocarditis in Spain: a population-based study (2003 to 2014). J Am Coll Cardiol. (2017) 70(22):2795–804. 10.1016/j.jacc.2017.10.00529191329 · doi ↗ · pubmed ↗
- 2Malakan Rad E Momtazmanesh S Saeedi Moghaddam S Rezaei N Rezaei N Jamshidi H Infective endocarditis in north Africa and the Middle East, 1990‒2019: updates from the global burden of disease study 2019. Arch Iran Med. (2024) 27(5):229–38. 10.34172/aim.2024.3438690789 PMC 11097324 · doi ↗ · pubmed ↗
- 3Che D Hu J Zhu J Lyu J Zhang X. Development and validation of a nomogram for predicting in-hospital mortality in ICU patients with infective endocarditis. BMC Med Inform Decis Mak. (2024) 24(1):84. 10.1186/s 12911-024-02482-738515185 PMC 10958908 · doi ↗ · pubmed ↗
- 4Kalisnik JM Leiler S Mamdooh H Zibert J Bertsch T Vogt FA Single-centre retrospective evaluation of intraoperative hemoadsorption in left-sided acute infective endocarditis. J Clin Med. (2022) 11(14):3594. 10.3390/jcm 1114395435887719 PMC 9317304 · doi ↗ · pubmed ↗
- 5Cordeiro J Raposo LM Godoy PH. Mortality profile of deaths related to infective endocarditis in Brazil and regions: a population-based analysis of death records. Trop Med Infect Dis. (2024) 9(12):291. 10.3390/tropicalmed 912029139728818 PMC 11679184 · doi ↗ · pubmed ↗
- 6Rajani R Klein JL. Infective endocarditis: a contemporary update. Clin Med (Lond). (2020) 20(1):31–5. 10.7861/clinmed.cme.20.1.131941729 PMC 6964163 · doi ↗ · pubmed ↗
- 7Cresti A Baratta P De Sensi F Aloia E Sposato B Limbruno U. Clinical features and mortality rate of infective endocarditis in intensive care unit: a large-scale study and literature review. Anatol J Cardiol. (2024) 28(1):44–54. 10.14744/Anatol J Cardiol.2023.346338167795 PMC 10796247 · doi ↗ · pubmed ↗
- 8Mirabel M Sonneville R Hajage D Novy E Tubach F Vignon P Long-term outcomes and cardiac surgery in critically ill patients with infective endocarditis. Eur Heart J. (2014) 35(18):1195–204. 10.1093/eurheartj/eht 30323964033 · doi ↗ · pubmed ↗