Vestibular Assessment in Infants with Congenital or Early Onset Sensorineural Hearing Loss: Is Neonatal Vestibular Screening Required? A Scoping Review
Lauren Farquhar, Amr El Refaie

TL;DR
This review examines whether infants with hearing loss are at higher risk of balance issues and if vestibular screening should be part of newborn hearing programs.
Contribution
The study provides a scoping review of vestibular assessment in infants with hearing loss, highlighting the feasibility and prevalence of vestibular dysfunction.
Findings
Infants with congenital or early onset SNHL are at higher risk of vestibular dysfunction.
cVEMP is the most commonly used and effective vestibular assessment tool in infants.
Findings suggest the need for vestibular screening in infants identified through hearing loss programs.
Abstract
Background/Objectives: Children with congenital or early onset sensorineural hearing loss (SNHL) are at a greater risk of vestibular dysfunction (VD), hypothesized to occur from the close embryological relationship between the cochlear and vestibular systems. Even with increasing focus on early detection and rehabilitation through Universal Newborn Hearing Screening (UNHS) programmes in many countries, few studies have focused on the prevalence and feasibility of vestibular assessment in infant populations. The objectives of this review are to 1. identify the prevalence of VD infants with congenital or early onset (<12 months old) SNHL, 2. identify which vestibular assessment tests/protocols are conducted on this population, 3. report sensitivity and specificity values for identified vestibular assessment tests/protocols. Methods: Studies that included infants aged 0–12 months, with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
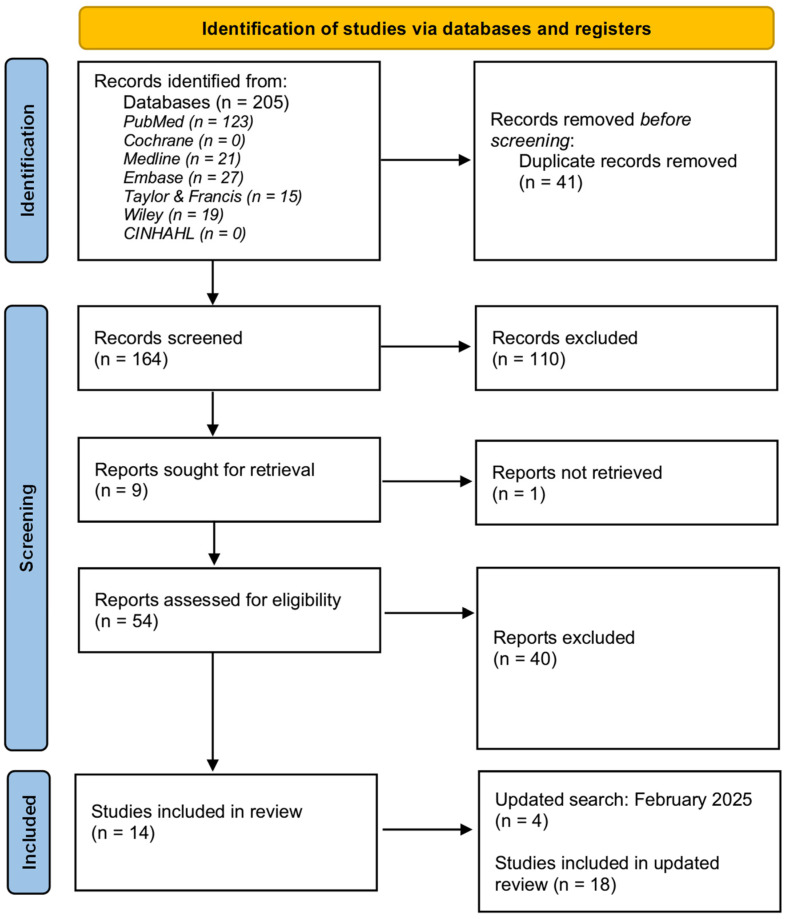 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing, Cochlea, Tinnitus, Genetics · Hearing Loss and Rehabilitation
1. Introduction
In recent years, research has increasingly focused on the prevalence and assessment of vestibular dysfunction (VD) in children with hearing loss, particularly sensorineural hearing loss (SNHL) [1,2,3,4,5]. Many studies have reported an increased prevalence of VD in older paediatric populations with SNHL, with and without cochlear implantation (CI) [6,7,8,9]. However, estimates of the prevalence of VD among these populations vary widely, ranging from 20% to 85% [10]. Despite high prevalence rates of VD reported among paediatric populations with SNHL, relatively limited focus has been observed among infant populations.
Over the past decade, many studies have attempted to substantiate the direct causal mechanisms for VD in children with SNHL [11,12,13]. It is theorized that the close embryological relationship between the cochlear and vestibular systems may contribute to this comorbidity [7,14], as any underlying aetiologies causing SNHL may also cause direct disturbance to the vestibular structures [4,15]. VD in infants can vary depending on the degree and configuration of SNHL, with severe-to-profound SNHL being the most associated with significant VD [16]. This is likely due to the shared susceptibility of both the cochlear and vestibular systems to congenital, perinatal, and acquired risk factors [17].
The vestibular system plays a crucial role in the mechanism of motor function, such as gaze and neck stability and coordination of head and neck movement relative to the body [16]. Consequently, children with SNHL and unilateral or bilateral vestibulopathy often exhibit delays in motor and balance performance, including crawling and walking [17]. In infants, this manifests as delayed gross motor development resulting from reduced ‘postural control, locomotion, and gait’ [4]. Early unilateral vestibulopathy could affect motor development due to slower development of vestibular compensation in infants, especially if a progressive vestibulopathy is observed [18,19].
The comorbidity of hearing loss, VD, and subsequent motor function delays can adversely impact an infant’s ‘spatial orientation, self-concept, and joint attention’ development [4,6]. Additionally, this association may indirectly and adversely affect cognition, literacy, learning skills, and broader psychosocial development [4].
Since the establishment of Universal Newborn Hearing Screening (UNHS) programmes in many countries, increasing attention has been given to the value of early detection and rehabilitation of infants with permanent childhood hearing loss [20]. Despite the growing body of evidence regarding the association between SNHL and VD in paediatric populations, vestibular assessments are not commonplace practice for infants with confirmed SNHL and are more commonly restricted to CI candidacy assessments [21]. However, Martens et al., 2020 [16] have been exploring the prevalence of VD and the feasibility of conducting vestibular assessments on Belgian infants with congenital or early onset SNHL. VIS-Flanders has implemented a vestibular screening pathway whereby all 6-month-old infants with congenital or early onset SNHL undergo vestibular screening using cVEMPs. It was reported that a significant proportion of the demographic screened elicited abnormal vestibular responses, particularly those with severe-to-profound SNHL and/or other comorbidities such as ‘meningitis…syndromes…congenital CMV [cCMV] and cochleovestibular anomalies’ [16].
While early vestibular assessment in infants with SNHL could enable more personalized and ‘deficit-specific’ rehabilitation plans, arguments against its widespread implementation include the role of connexin 26 gene mutations that leave the vestibular system without anomaly, cost-effectiveness concerns, and the lack of large-scale studies providing substantial evidence to support its inclusion in UNHS programmes [1].
Therefore, conducting a scoping review is a crucial first step in determining if the addition of a vestibular screening component to UNHS pathways is supported by evidence.
Objectives
Which vestibular assessment tests or protocols are undertaken in infants with congenital or early onset (<12 months old) SNHL?What are the measures of association regarding VD in infants with congenital or early onset (<12 months old) SNHL?What are the sensitivity and specificity values of the vestibular assessment tests or protocols in infants with congenital or early onset (<12 months old) SNHL?
2. Materials and Methods
2.1. Protocol and Registration
This scoping review (ScR) was conducted in accordance with the JBI Manual for Evidence Synthesis [22] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMAScR) extension statement [23]. The scoping review was also conducted in accordance with the UCC Code of Research Conduct policy [24]. No prior registration was required for this review as it was conducted as partial fulfilment of the MSc Audiology in University College Cork.
2.2. Eligibility Criteria
Before commencing, clear eligibility criteria for included data sources were established by utilizing the Population, Concept, and Context (PCC) framework.
The inclusion parameters were as follows:
- Population: Infants with congenital or early onset (<12 months old) SNHL, with or without cochlear implantation. For this review, infants were defined as human beings aged 0–12 months of age [25]. Any data sources combining results from infants and older paediatric age groups had to report them separately.
- Concept: Articles that included at least one vestibular test in evaluating vestibular function in the target population. Vestibular tests in this study were defined as any test that measures the vestibulo-ocular reflex (VOR), vestibulo-collic reflex (VCR), or vestibulo-spinal reflex (VSR) in isolation.
- Context: Articles were required to report one or more of the following: (i) Measures of association of VD in the target population (with/without cochlear implantation) or in comparison to healthy controls or other groups of children with SNHL (with/without CI). (ii) Types of vestibular function tests carried out on the target population (with/without CI) in isolation or in comparison with other vestibular tests. (iii) Sensitivity and specificity of vestibular test(s).
- Other: Primary, secondary data, or grey literature published in the English language and sourced during the searching period between 1 February and 21 April 2023 and updated in February 2025 were evaluated for inclusion. Literature was required to be accessible through full text or granted access through contact with author(s) or other libraries.
The exclusion criteria were as follows:
Articles with infants with temporary or isolated conductive hearing loss. Articles conducting vestibular assessments solely on infants with (i) hearing within normal limits or (ii) infants with hearing within normal hearing limits AND medical conditions that could be risk factors for the future development of SNHL. Articles using animal or non-human models. Position or opinion papers that do not correlate or are outside the parameters of the study objectives.
2.3. Information Sources
The following databases were searched for relevant literature: PubMed, CINAHL, Cochrane Library, Embase, MEDLINE, Wiley, and Taylor & Francis.
2.4. Search
An initial preliminary search of Google Scholar was conducted to provide an overview of the size and scope of available literature on the subject using keywords (Appendix A.1). JBI recommends using at least two databases for initial searching while establishing a complete search string; thus, preliminary searches of PubMed and Embase were conducted [23]. It is important to note that Google Scholar was used as a primary exercise and was not utilized during comprehensive searching. All relevant papers were assessed to establish appropriate text words, keywords, MeSH, and index terms to create a comprehensive search string to be adapted for use across the databases being searched. Once two completed search strings had been established (Appendix A.2 and Appendix A.3), a comprehensive search was conducted on the stated databases. Two separate search strings were created for databases with and without a MeSH index. Comprehensive searching of all databases was conducted from 1 to 7 February 2023, updated on 21 April 2023, and updated again on 21 February 2025.
2.5. Selection of Sources of Evidence
All returned articles were manually logged in Microsoft Excel and assessed for inclusion eligibility as per a phased process stated below.
Phase 1—Identification: All selected databases were search with the resulting articles arranged in alphabetical order (author, year). All duplicates were removed manually.Phase 2—Screening: All titles and abstracts of string searches across all selected databases were screened according to the eligibility criteria. In cases where no abstract was available or there was any uncertainty regarding eligibility, articles were referred directly to phase 3.Phase 3—Eligibility: Full-text screening was conducted for articles which were considered for inclusion after title and abstract screening. In any case of uncertainty regarding the inclusion of articles, a supervisor within the UCC Audiology Department was consulted.Phase 4—Inclusion: Eligible articles were documented and included in the review.
2.6. Data Charting Process
The objectives of the review were analysed before designing appropriate extraction tables for charting all relevant data. The data charting process was begun by separately assessing all included articles and presenting key information relating to the review objectives. Extraction tables were utilized to systematically map and collate all relevant information across all included articles. Completed extraction tables can be viewed in Section 3.
2.7. Data Items
Data items extracted from each article were article type, year of publication, subject source, time range of data collection, total number of subjects, age range of subjects, aetiology and diagnosis of SNHL, laterality, degree and configuration of SNHL, cochlear implantation status, vestibular assessment type, vestibular assessment protocols and normative values, sensitivity and specificity values of reported vestibular assessments and measures of association between SNHL and vestibular dysfunction.
2.8. Critical Appraisal of Included Sources of Evidence
Critical appraisal of all articles included in the review was conducted where applicable using critical appraisal forms formulated by JBI [26] (Appendix B). Critical appraisal of included articles was completed to systematically assess the overall quality and risk of bias across the included articles.
2.9. Synthesis of Results
The handling and summarization of charted data collated all results from the included articles. As each article reported results differently, data were summarized and collated using extraction tables. Synthesis of results followed the order of the objectives stated at the start of the review.
3. Results
3.1. Selection of Sources of Evidence
The article selection process is illustrated in Figure 1. PRISMA flow diagram. A total of 205 articles were identified in the initial search. After removing 41 duplicates, the remaining 164 articles underwent title and abstract screening. During title and abstract screening, 110 articles were excluded as they did not align with the study objectives. 9 articles were sought for retrieval from other libraries or contacting the author(s). 1 article was unable to be retrieved. 54 articles were assessed for eligibility by full text, and 14 articles met the inclusion criteria. An updated search was conducted in February 2025 and a further 4 articles met the inclusion criteria. Therefore, a total of 18 articles were included in this review.
3.2. Characteristics of Sources of Evidence
This review comprised 18 articles, including seven prospective cohorts (three with specified longitudinal follow-up), one observational cohort, two cross-sectionals, five case controls, two case studies, and one methodological study [4,16,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] (Table 1). The researchers observed a wide geographical variation between the included articles from Europe to Asia to North America and were published from 2005–2023. Most articles were of European origin [4,16,27,28,29,30,31,32,33,36,37,38,39,40,41,42] and conducted within hospital settings, some using medical registries to recruit the sample population. Sample sizes varied significantly, with recently published articles generally having larger sample sizes. Most studies reported age-matched controls, with a few comprising older children or adults as comparator groups. The age range of study participants ranged from two to twelve months.
3.3. Critical Appraisal Within Sources of Evidence
JBI critical appraisal tools [26] were used to assess the methodological quality and risk of bias in all included articles. Completed critical appraisal forms are included in Appendix B. Most articles were deemed as having a low risk of bias. Three articles were deemed as having a low-moderate risk of bias and one article was deemed as having a moderate risk of bias. All risk of bias ratings are stated in Table 2.
3.4. Results of Individual Sources of Evidence
From the 18 included articles, two articles did not report how SNHL was assessment and diagnosed in the study subjects. Most articles reported comprehensive reports of how VD was assessed and diagnosed in the study subjects. Three articles reported corresponding sensitivity and specificity values for the vestibular assessments used. Eight articles reported details on the type of VD recorded. All but two articles reported measures of association between SNHL and VD across the study subjects. Further details are provided in ‘3.5. Synthesis of Results’.
3.5. Synthesis of Results
3.5.1. Characteristics of SNHL and Diagnosis
The articles primarily reported the aetiology of SNHL as ‘congenital’ and/or ‘early onset’, with some articles focusing on specific target aetiology such as Usher syndrome Type 1, congenital cytomegalovirus (cCMV), connexin 26 mutations, rubella, and autosomal recessive hereditary nonsyndromic deafness. Diagnostic approaches for SNHL varied across the articles, with several using otoscopy, tympanometry, and TEOAEs or DPOAEs. All articles reported using some form of auditory brainstem response (ABR) assessment. Click-evoked ABR (Click-ABR) was the most reported method, with three articles using automated ABR (AABR) screening. Few articles detailed the frequencies tested during ABR assessments. Most articles reported the laterality and degree of SNHL, ranging from mild to profound. Several articles reported the proportion of participants with cochlear implantation at the time of vestibular assessment, although some articles did not report on this for subjects with severe–profound SNHL (Table 3).
3.5.2. Vestibular Assessments and Corresponding Sensitivity and Specificity Measures
The timing of vestibular assessments varied across articles, with the youngest infants assessed at 2.3 months and others at six to twelve months. The most common vestibular test was cervical vestibular-evoked myogenic potentials (cVEMPs) [4,16,28,29,30,31,32,33,34,35,37,38,39,40,41,42]. Five articles conducted video head impulse testing (vHIT) on infants aged six to twelve months [28,29,30,33,38]. Five articles conducted calorics on infants [38,39,40,41,42]. Modified rotatory chair assessments were conducted on infants across three included articles [28,33,36] and was determined as the least commonly used test. Further information on the vestibular assessments, protocols and normative cut-off values are reported in Table 4. Testing protocols and normative cut-off values varied across articles, with only three articles reporting both sensitivity and specificity values [29,37,39]. The cVEMP technique and protocols specified in the three articles that reported sensitivity and specificity values for cVEMPs are reported in Table 5.
3.5.3. Measures of Association Between Vestibular Dysfunction and SNHL in Infants
Most articles reported increased prevalence rates of VD in infants with congenital or early onset SNHL. Three articles reported the specific types of VD observed among the sample population [27,28,29]. The methodological study primarily reported success rates of vestibular assessment in the specified target population [37]. Full details on measures of association are reported in Table 6.
4. Discussion
Summary of Evidence: This scoping review was conducted to preliminarily assess the size and scope of available evidence regarding vestibular assessment on infants with congenital or early onset SNHL (with or without cochlear implantation) under twelve months of age. The primary objectives of this review were to 1. identify the prevalence of VD infants with congenital or early onset SNHL, 2. identify which vestibular assessment tests/protocols are conducted on this population, 3. report sensitivity and specificity values for identified vestibular assessment tests/protocols.
Given that paediatric vestibular assessment is rarely performed outside the realms of cochlear implant candidacy, few articles have focused on the infant population. This scarcity of literature justified the need for a scoping review to map the available evidence on this subject area. This review included mainly observational studies, as they were deemed the most appropriate in providing robust evidence for the research question.
The primary purpose of conducting vestibular assessments on infants is to differentiate between normal and abnormal vestibular function while accounting for the developmental and maturation stage of the infant. Four vestibular function tests were identified across included articles: cVEMPs, vHIT, calorics, and modified rotational chair testing. The cVEMP was the most commonly observed assessment tool in the target population across the included articles. Martens et al. (2023) [33] reported a 90% success rate for cVEMPs in six-month-olds compared to 70% for vHIT and 72.9% for the rotatory chair. This agreed with Verrecchia et al. (2019) [37], who reported cVEMPs to be highly reproducible and feasible in infants as young as 2.3 months. Zagólski O (2007) [39] reported similar results among his cohort of eighteen three-month-old infants, stating that this form of assessment was feasible in this age group, although issues relating to cooperation could impact clinicians’ ability to obtain reliable and reproducible results. These reports closely correlate with studies conducted on older children, indicating cVEMPs are both feasible and child friendly.
Other vestibular assessments, such as ‘minimized rotational chair’, were deemed easy to perform and favoured by Teschner et al., 2008 [36] due the reduced ability of young children to suppress gaze fixation. This test was reported as an altered version of the ‘Rotatory Intensity Damping Test’ that involved the child sitting on the lap of the parent while the chair rotated in a single, vigorous motion, and abruptly stopped. The child was then directly observed for nystagmus without the use of ENG [36]. Similar findings were reported in older children by Maes et al. (2014) [2]. Caloric testing in infants was reported to be more invasive and presented more limitations than cVEMPs, whereby reduced responses could be misinterpreted as bilateral vestibular hypofunction [40,42]. Other issues relating to correct irrigation due to smaller ear canal size were reported as a concern potentially leading to high levels of interindividual result variability [40,42]. Dhondt et al. (2022) [29] reported vHIT to be sensitive in detecting dysfunction in six-to-twelve-month-olds, similarly reported in older paediatric populations with more pronounced VD.
The age at which vestibular assessments were conducted varied widely across the studies. Shen et al. (2022) [34] reported that vestibular organ maturation at three months allowed for response rates equivalent to adults when using bone-conducted cVEMPs. However, Martens et al. (2023) [33] recommended conducting assessments at six months old to ensure increased cooperation and reduce confounding factors related to maturation development. However, Sheykholesami et al. (2005) [35] stated that accurate and reproducible results could be obtained from 2.3-month-old infants, although longer latencies in P13 and N23 were observed due to immature maturation.
Significant variations in sensitivity and specificity were reported across the vestibular tests, indicating that these tests may be complementary to each other rather than fixed substitutions. Several articles did not report these metrics, highlighting a gap in the literature. A previous systematic review conducted by Verbecque et al. (2017) [10] on older children (>3 y) reported cVEMP sensitivity between 48% and 100%, with a specificity range of 30% to 100%. This was similar to a previous study conducted on an adult population with SNHL that yielded a sensitivity of 91.4% and specificity of 95.8% [43]. In comparison, Zagólski O (2007) [39] reported a cVEMP sensitivity and specificity of 100% when utilizing calorics in comparison. Dhondt et al. (2022) [29] reported a vHIT of 30% sensitivity and 91% specificity in infants with congenital SNHL attributed to CMV, reported similarly by Duarte et al. (2022) [21]. Furthermore, in infants with cCMV and early onset SNHL, a sensitivity of 50% and a specificity of 91% was reported. Martens et al. (2023) [33] refrained from presenting such measures, stating that the validity of such measures could not be substantiated due to conflicts between results relating to other utilized vestibular tests.
Higher prevalence rates of VD in infants with congenital or early onset SNHL were observed across the majority of included articles [16,27,28,29,30,31,32,33,34,39,40,41,42]. The evidence included in this review reported that infants with severe–profound unilateral or bilateral SNHL were at a higher risk of VD compared to infants with mild–moderate SNHL. Often this risk was exacerbated by the presence of additional medical conditions rendering the infant more susceptible to presenting with SNHL. This finding correlates with articles conducted on older populations that reported higher prevalence of VD in those with greater degrees of SNHL. The observed high prevalence rates of VD in infants with congenital or early onset SNHL across included articles indicates that vestibular assessments potentially could be conducted on this population in an accurate, reliable, and reproducible modality. Martens et al. (2019) [4] have designed a potential pathway to implement vestibular screening seamlessly into UNHS programmes globally.
Vestibular assessment fulfils a potentially crucial role in the identification and management of opportunities for infants with SNHL who have been reported to be at a higher risk of VD [7]. Substantiating this link alongside developing the most appropriate method of assessing this population has the potential to provide valuable insights into more individualized rehabilitation processes. Through earlier detection of VD in infants with SNHL, clinicians can provide targeted intervention strategies in optimizing the developmental outcomes for this population.
Additionally, vestibular assessment can help identify particular aetiologies of sensorineural hearing loss [44]. Both hearing loss and VD are linked to specific prenatal abnormalities and genetic diseases [45]. Clinicians can acquire more diagnostic data by assessing the vestibular system, which may help identify the underlying cause of the hearing loss. This information is essential for genetic counselling, predicting developmental outcomes, and directing medical and surgical procedures.
Across the included articles, cVEMP was reported as a feasible test for infants due to high rates of successful measurements whether a response was present, absent, or inconclusive [4,16,28,29,30,31,32,33,34,35,37,38,39,40,41,42]. However, due to its limitation of which part of the system it assesses, other suitable and child-friendly assessments may be considered as potentially complementary tests to minimize any overlooked VD. Factors such as insufficient SCM muscle contraction, lack of cooperation, agitation, and protracted crying increased the risk of artifacts in cVEMP recordings [37]. Since vestibular assessments in infants can be more challenging in comparison with adults, most studies reported modifications to testing protocols. As infants cannot independently contract their SCM muscles, examiners used passive techniques, such as supporting the head during assessments or positioning the infant in a supine position [29,37,39]. Additionally, most studies favoured bone-conducted (BC) stimuli over air-conducted (AC) stimuli due to the higher prevalence of middle ear dysfunction in infants, such as middle ear effusion. In comparison to adults, infants often exhibited greater variability in response amplitudes and latencies, with some articles noting varying amplitudes and latencies in this population.
Overall, the results of this scoping review demonstrate that a higher prevalence of VD is observed in infants with congenital or early onset SNHL. The results also indicate that vestibular assessment can be both feasible and diagnostically accurate in infants with SNHL.
Directions for Future Research: The review emphasizes the need for further research and robust evidence before policy changes and implementation of targeted interventions are recommended. To progress knowledge development in this area, large-scale, prospective studies with longitudinal follow-up on cVEMPs are a priority research area. Research that refines and standardizes vestibular assessment protocols and normative cut-off values for cVEMPs is required to substantiate clearer prevalence estimates in infants with SNHL and risk factors for comorbidity, such as but not limited to Pendred syndrome, Usher syndrome, Waardenburg syndrome, and CHARGE syndrome [46]. Standardizing cVEMP protocols would lead to more defined sensitivity and specificity values. Research that compares the effect of bilateral versus unilateral vestibular dysfunction on functional motor development in infants with SNHL is also required. Cost analysis investigations are recommended to determine the cost associated with implementing an additional neonatal screening pathway in UNHS programmes.
5. Limitations
Although this scoping review provides promising results regarding the potential value of conducting vestibular assessment in infants with sensorineural hearing loss, the review must be viewed in light of several limitations. Firstly, the review was conducted by an independent novice researcher within a relatively short timeframe, which may have resulted in the omission of relevant articles during searching. Restricting the search to full-text articles published in the English language may have further limited the pool of eligible sources. This search yielded a small number of eligible articles for inclusion, which highlights a lack of research on the subject. Furthermore, variations in sample sizes observed across the included articles may lack generalizability. Unstandardized protocols and normative cut-off values could have introduced measurement bias, directly affecting prevalence estimation and sensitivity and specificity values in the sample populations. Variability in the signal-to-noise (SNR) ratio in infants could have impacted how present responses, absent responses, and inconclusive responses were reported in the articles. Many included articles did not report controlling for confounding factors.
6. Conclusions
The results of this review signal the potential value of conducting targeted vestibular assessment using cVEMPs in infants with congenital or early onset SNHL in UNHS programmes. Further prospective, large-scale research, with refined vestibular assessment protocols and normative cut-off values, is required to develop clearer prevalence estimates of VD and standardize assessments in the study demographic. As implementing such an intervention would be costly and time-consuming on already over-burdened healthcare systems, it is recommended that such targeted vestibular assessments could be conducted on infants with greater degrees of hearing loss and those with specific risk factors for comorbidity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angeli S. Value of Vestibular Testing in Young Children with Sensorineural Hearing Loss Arch. Otolaryngol.–Head Neck Surg.200312947810.1001/archotol.129.4.47812707199 · doi ↗ · pubmed ↗
- 2Maes L. De Kegel A. Van Waelvelde H. Dhooge I. Rotatory and Collic Vestibular Evoked Myogenic Potential Testing in Normal-Hearing and Hearing Impaired Children Ear Hear.201435 e 21e 3210.1097/AUD.0b 013e 3182 a 6ca 9124556969 · doi ↗ · pubmed ↗
- 3Oyewumi M. Wolter N.E. Heon E. Gordon K.A. Papsin B.C. Cushing S.L. Using Balance Function to Screen for Vestibular Impairment in Children with 55 Sensorineural Hearing Loss and Cochlear Implants Otol. Neurotol.20163792693210.1097/MAO.000000000000104627228014 · doi ↗ · pubmed ↗
- 4Martens S. Dhooge I. Dhondt C. Leyssens L. Sucaet M. Vanaudenaerde S. Rombaut L. Maes L. Vestibular Infant Screening–Flanders: The implementation of a standard vestibular screening protocol for hearing-impaired children in Flanders Int. J. Pediatr. Otorhinolaryngol.201912019620110.1016/j.ijporl.2019.02.03330849604 · doi ↗ · pubmed ↗
- 5Gadsbøll E. Erbs A.W. Hougaard D.D. Prevalence of abnormal vestibular responses in children with sensorineural hearing loss European Arch. Oto Rhino-Laryngol.20222794695470710.1007/s 00405-021-07241-235156132 · doi ↗ · pubmed ↗
- 6Wiener-Vacher S.R. Vestibular disorders in children Int. J. Audiol.20084757858310.1080/1499202080233435818821227 · doi ↗ · pubmed ↗
- 7Cushing S.L. Papsin B.C. Rutka J.A. James A.L. Gordon K.A. Evidence of Vestibular and Balance Dysfunction in Children With Profound Sensorineural Hearing Loss Using Cochlear Implants Laryngoscope 20081181814182310.1097/MLG.0b 013e 31817 fadfa 18758383 · doi ↗ · pubmed ↗
- 8Santos T.G.T. Venosa A.R. Sampaio A.L.L. Association between Hearing Loss and Vestibular Disorders: A Review of the Interference of Hearing in the Balance Int. J. Otolaryngol. Head Neck Surg.2015417317910.4236/ijohns.2015.43030 · doi ↗