Postherpetic Pseudolymphomatous Angiosarcoma Concealed Within Milia en Plaque: Expanding the Spectrum of Wolf Isotopic Response with a Literature Review
Marina Corral-Forteza, Noelia Pérez-Muñoz, Maria-Teresa Fernández-Figueras

TL;DR
A rare case of angiosarcoma with pseudolymphomatous reaction is reported in a site of healed herpes zoster, expanding the understanding of the Wolf isotopic response.
Contribution
This case expands the known spectrum of postherpetic WIR by documenting a rare coexistence of pseudolymphomatous angiosarcoma and milia en plaque.
Findings
A 96-year-old woman developed pseudolymphomatous angiosarcoma at a site of resolved herpes zoster.
The case highlights the potential for diverse pathologies in areas of prior skin disease under WIR.
The review provides updated pathogenic theories and a compilation of postherpetic reactions.
Abstract
The Wolf isotopic response (WIR) refers to the development of cutaneous lesions in areas of previously healed but unrelated skin disease. While most are observed in healed herpes zoster, WIR has been reported in various other contexts. Affected areas are believed to exhibit immune dysregulation, lymphatic dysfunction, and altered neuromediator activity, increasing susceptibility to inflammatory, neoplastic, and infectious conditions. This phenomenon aligns with the broader concept of the “immunocompromised district”, which also encompasses the Koebner phenomenon and its reverse. Herein, we present the case of a 96-year-old woman who developed multiple cysts and comedones at the site of a resolved herpes zoster. Due to persistent and refractory inflammation, curettage was performed, and histopathological examination revealed angiosarcoma with a pseudolymphomatous reaction interspersed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
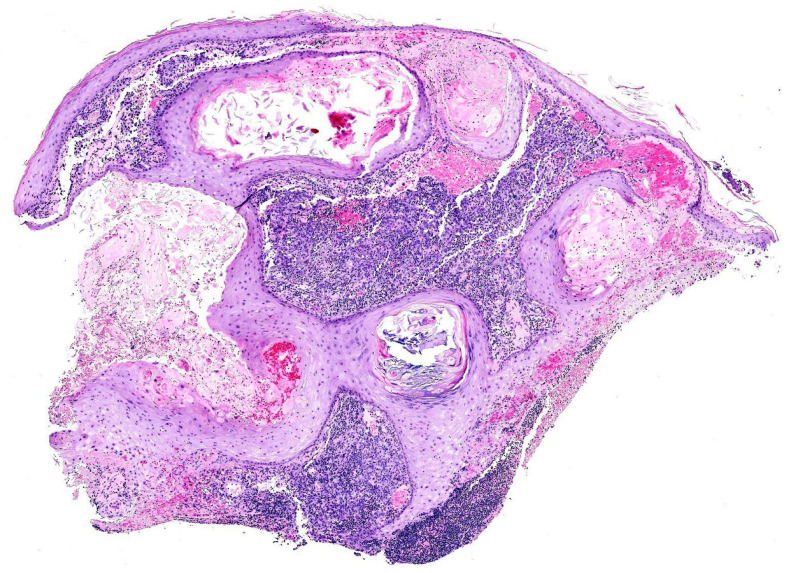 Figure 1
Figure 1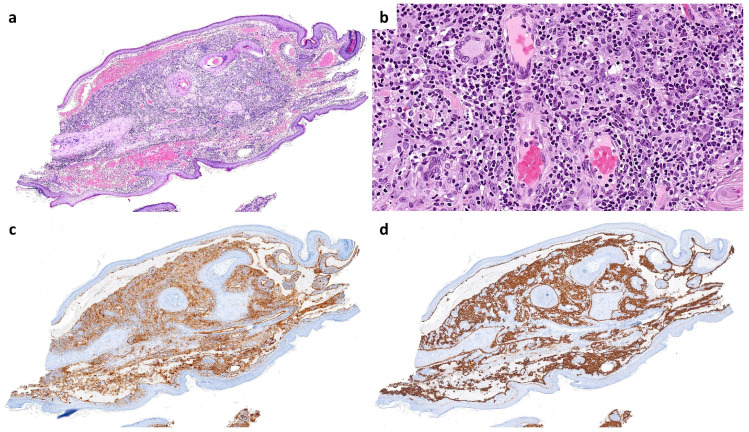 Figure 2
Figure 2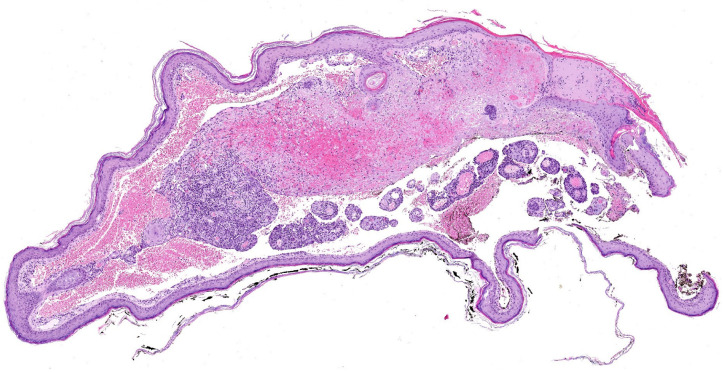 Figure 3
Figure 3| Inflammatory Diseases | Infections |
|---|---|
| Acne | Molluscum contagiosum |
| Acneiform lesions | Warts and papillomata |
| Actinic granuloma (O’Brien) [ | Candidiasis |
| Bullous pemphigoid [ | Dermatophytosis |
| Chronic cutaneous graft-versus-host disease | |
| Chronic small vessel vasculitis (Extrafacial eosinophilic granuloma or Lever granuloma) [ | |
| Chronic urticaria [ | |
| Comedones | |
| Comedonic-microcystic reactions | |
| Contact dermatitis | |
| “Dysimmune” reactions | |
| Eosinophilic dermatosis | |
| Erythema annulare centrifugum | |
| Fibroelastolytic papulosis | |
| Folliculitis (granulomatous or eosinophilic [ |
|
| Follicular mucinosis [ | Angiosarcoma |
| Furunculosis | Basal cell carcinoma |
| Granuloma annulare [ | Basosquamous carcinoma |
| Granulomatous folliculitis | Benign lymphangioendothelioma [ |
| Granulomatous reactions (necrotizing or non-necrotizing) | Bowen disease |
| Granulomatous vasculitis | Breast carcinoma |
| Grover disease (personal case) | Kaposi sarcoma |
| Infections | Leukemia |
| Keloid | Lymphangiogenesis (pseudotumoral) [ |
| Lichen planus | Lymphomas |
| Lichen sclerosus et atrophicus-morphea | Mastocytosis [ |
| Lichen simplex | Metastases (from breast carcinoma and others) |
| Lichenoid dermatitis | Pseudolymphoma |
| Linear IgA dermatosis | Rosai-Dorfman disease |
| Lupus erythematosus [ | Squamous cell carcinoma |
| Milia | Syringoid eccrine carcinoma [ |
| Mucinosis | Tufted Angioma [ |
| Nodular solar degeneration | |
| Palpable purpura | |
| Pityriasis rosea (atypical) [ | |
| Prurigo-like eruption | |
| Psoriasis | |
| Reactive perforating collagenosis | |
| Rosacea | |
| Sarcoidosis | |
| Unilateral nevoid telangiectasia [ | |
| Vitiligo [ | |
| Xanthoma [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cutaneous lymphoproliferative disorders research · Eosinophilic Disorders and Syndromes
1. Introduction
Wolf isotopic response (WIR) is defined as the appearance of new skin lesions at the site of a previously healed, unrelated skin disease [1]. This intriguing phenomenon was first described in 1955 by Wyburn-Mason [2], but it remained relatively unrecognized until 1995 when Wolf formally established the concept and introduced the term “isotopic response [3]”. This terminology was intended to distinguish it from the Koebner isomorphic phenomenon, in which a disease develops in a previously healthy area that has undergone inflammation due to trauma, infection, or other conditions. Until that moment, cases of WIR had traditionally been considered variants of the Koebner phenomenon [4]. The terms “isotopic” and “isomorphic” highlight the fundamental differences between these two reactions “isotopic” refers to the development of two distinct diseases at the same site, and “isomorphic” (from Greek, “equal shape”) emphasizes that the new condition reproduces the outline of the preceding lesion [5].
The classification of WIR remains a topic of ongoing debate in dermatology. Over time, a diverse and sometimes inconsistent terminology has emerged in the literature, with terms such as locus minoris resistentiae, isomorphic, isopathic response, and pseudoisomorphic response being used to describe similar phenomena [6]. Additionally, the distinction between WIR and the Koebner phenomenon has been widely questioned, with some experts strongly disputing their classification as separate entities [4].
In 2014, Ruocco et al. introduced the concept of the immunocompromised cutaneous district (ICD) to unify these terminologies and provide a broader pathophysiological framework encompassing WIR and related phenomena [6]. The ICD model emphasizes localized immune dysregulation as a key factor in creating vulnerable skin regions predisposed to secondary dermatological conditions. However, growing evidence suggests that WIR development is influenced by additional mechanisms, including structural alterations, neural dysfunction, and vascular damage [6].
A wide range of conditions has been proposed to predispose the WIR, including congenital malformations such as primary lymphedema or skin mosaicisms as well as acquired conditions such as secondary lymphedema, neural diseases, trauma, burns, tattoos, and intradermal vaccinations [6]. However, the most common underlying causes of this localized vulnerability are herpetic infections, with herpes zoster being far more frequent than herpes simplex. The link between herpetic infections and WIR is particularly significant, as these infections appear to induce long-term alterations in the cutaneous immune microenvironment. Even after the initial infection resolves, the affected skin remains in a localized immunocompromised state, making it more susceptible to the development of new, unrelated dermatological conditions.
The spectrum of WIR manifestations following herpetic infections is remarkably diverse, encompassing a variety of skin disorders such as granulomatous reactions, lichenoid eruptions, psoriasis, and even malignant transformations. Additionally, these compromised areas may exhibit an increased susceptibility to metastatic deposits or local involvement by systemic lymphoproliferative disorders. Furthermore, the heightened incidence of lesions in these compromised regions can lead to the coexistence of multiple pathologic conditions at the same site, posing significant diagnostic and therapeutic challenges for dermatopathologists and clinicians [7].
2. Case Report
The 96-year-old woman had a history of herpes zoster involving the right side of her face, corresponding to the second branch of the trigeminal nerve, which resolved spontaneously. Two years later, she developed numerous milia and comedones in the same area, accompanied by edema, erythema, serous transudation, and severe pain. Magnetic resonance imaging revealed microcystic subcutaneous lesions in the right infraorbital region. Based on these findings, a clinical diagnosis of inflamed milia en plaque was made. Despite treatment with topical agents and oral antibiotics, only partial improvement was achieved, necessitating surgical curettage.
Histopathological examination of the curetted material, composed of numerous skin fragments, revealed features of inflamed milia en plaque (Figure 1). In many fragments, an abundant lymphocytic infiltrate obscured a population of highly atypical cells arranged in cords and sheets that co-expressed CD31 and D2-40 (Figure 2), an immunoprofile characteristic of angiosarcoma.
Additionally, occasional cavities lined by atypical endothelial cells were observed, containing free-floating tumor aggregates with central vessels and abundant stromal lymphocytes (Figure 3). This finding corresponds to the “fish in the creek” pattern, which is also characteristic of angiosarcoma [8]. These features led to a final diagnosis of pseudolymphomatous angiosarcoma associated with multiple comedones.
Given the patient’s advanced age and her preference, conservative management with palliative care was chosen.
3. Discussion
The clinicopathological case we present is paradigmatic of WIR, with the coexistence of three distinct pathologic conditions at the site of a healed herpes zoster infection: angiosarcoma, pseudolymphomatous infiltrates, and comedones [9,10,11]. The occurrence of multiple synchronous WIR pathology conditions is rare but not unique, with reports documenting two [12] or even three [7] pathologic conditions at the same site. In this patient, the pseudolymphomatous infiltrates were likely related to WIR, given the well-documented inflammatory processes associated with this phenomenon. However, an alternative explanation could attribute the infiltrates to a rare pseudolymphomatous variant of angiosarcoma [13], with the lymphocytic component being primarily tumor-related rather than part of a WIR. While definitive proof is lacking, the rarity of this angiosarcoma variant and the presence of multiple simultaneous entities in the same site strongly suggest that WIR played a role in driving the inflammatory response. Conversely, comedones have not been previously described in association with angiosarcoma, which has been linked only to verrucous epidermal hyperplasia [14].
The exact etiopathogenesis of WIR remains unclear. Various factors have been proposed, and it is likely that multiple mechanisms are involved in different cases, which are listed as follows:
Viral persistence: This may explain some postherpetic reactions since viral DNA has been isolated in certain cases. However, after herpetic infections resolve, viral DNA is no longer detected. This mechanism likely applies only to reactions occurring within a short interval (less than four weeks) after the herpes infection [6,15].Lymphovascular microvasculature alteration: Damage to the microcirculation can render an area unable to respond adequately to subsequent insults, leading to localized inflammation at the same site [6].Local immune dysregulation: The initial skin disease may impair normal immunological functions in the affected area. Altered regional immunity, including the contribution of resident memory T cells, could predispose the site to new cutaneous diseases following a trigger [6,16].Neural injury: Damaged dermal nerve fibers can contribute to disease pathogenesis, either directly through neuropeptide release or indirectly via immune system activation [6]. Specifically, neuropeptides such as nerve growth factor (NGF), which regulates skin epithelization, angiogenesis, and the formation of an extracellular matrix [17], as well as substance P from damaged nerve endings, which might play a crucial role in inducing the development of epidermal changes [18].
In addition, a plausible explanation for the milia could be related to sebaceous gland lipogenesis stimulated by substance P, followed by the proliferation of Propionibacterium acnes [11].
Postherpetic reactions represent the most common scenario for WIR, and a wide spectrum of pathologic conditions have been described in this context. Ruocco and colleagues [6] collected a large series of cases, which has since been expanded with additional reports. We provide an updated list of the inflammatory, infectious, and neoplastic postherpetic reactions reported to date, arranged in alphabetical order to facilitate the search for their histopathological features and ensure none are overlooked (Table 1).
Most WIR cases involve inflammatory dermatoses, granulomatous reactions being the most frequent. The spectrum also includes infections, reactive processes such as milia or pseudolymphomas, and tumors. Among the latter, vascular lesions, including angiosarcoma, have occasionally been reported in areas previously affected by herpes zoster [9,10,19,20].
The history of WIR exemplifies the ongoing evolution of knowledge in dermatological sciences. What began as a keen clinical observation, initially imprecise but insightful, gradually evolved into a refined model of WIR, which has been expanded and redefined over time. As our understanding of the intricate relationship between skin integrity, immune function, and disease manifestations has evolved, certain subclassifications of cutaneous reactions now appear redundant. A logical approach involves categorizing these reactions based on their proposed pathophysiological mechanisms, leading to broader, more integrative concepts, such as the ICD, which provide a unifying framework for these phenomena.
This process began in 1955 when Wyburn-Mason first published a series of cases highlighting an apparent increased risk of malignant changes in skin previously affected by herpes zoster [2]. He described 10 cases on the face and 15 on the thorax. Notably, while the facial cases involved cutaneous malignancies (five basal cell carcinomas, four squamous cell carcinomas, and two cases with mixed features), only one of the thoracic cases was a cutaneous tumor (squamous cell carcinoma). The remaining 14 cases were mammary gland carcinomas that, despite involving the same breast whose overlying skin had been previously affected by herpes zoster, would not be considered WIR by the present standards, but rather a coincidental occurrence.
The term isotopic response was later coined by Wolf in 1985 to describe this phenomenon, emphasizing the development of a new, unrelated skin disorder at the exact site of a previous, healed skin condition. However, the word isotopic is also widely used in medical fields to refer to radioactive isotopes, a coincidence that may have led to confusion and difficulties in retrieving specific scientific literature on this topic. To avoid ambiguity, the eponym Wolf was added, making Wolf isotopic response (WIR) the preferred and most used term.
Today, WIR is recognized as a distinct dermatological entity, with a wide range of predisposing conditions. These include congenital malformations (such as primary lymphedema, and skin mosaicisms) and acquired conditions (such as secondary lymphedema, neural diseases, trauma, burns, tattoos, or intradermal vaccinations). Its clinical significance underscores the importance of considering the dermatological history of every patient when evaluating new skin lesions.
Distinguishing WIR and Koebner’s isomorphic response or its reverse, the so-called Renboek phenomenon, remains relevant for the sake of diagnostic precision. However, overlapping pathophysiological mechanisms likely exist [4], including increased local expression of nerve growth factor (NGF) and vascular endothelial growth factor (VEGF), which may contribute to disease susceptibility in affected areas [33]. Clinicians and dermatopathologists sometimes struggle to classify their patients’ conditions. Table 2 provides definitions and examples to aid in the traditional classification of these entities and, most importantly, to distinguish them from pathergy.
In 2014, Ruocco et al. introduced the ICD concept, providing a unifying pathophysiological framework that encompasses WIR and related conditions. However, this terminology has not yet been widely introduced into clinical practice.
4. Conclusions
Shifting from traditional classifications exposed in Table 2 to newer frameworks where most of these reactions are grouped under the umbrella term of the Koebner phenomenon or the newer terminology of ICD, requires time. It will be necessary to overcome inertia and dismantle long-standing paradigms. In the meantime, the specific terminology used in clinical practice is of secondary importance, as long as scientific progress continues to refine our understanding of their likely shared underlying mechanisms and ensures that therapeutic strategies remain effective and evidence-based.
The clinicopathological case included in this review exemplifies the importance of recognizing the diverse spectrum of postherpetic WIR and closely monitoring patients who develop new lesions at previously healed sites of another skin disease. This is particularly critical given the potential for malignant tumors to develop. Early histopathological studies with adequately sized specimens are crucial to enable a prompt diagnosis. In the patient we are reporting, a superficial shave biopsy would have likely confirmed the presence of milia, comedones, and lymphocytic infiltrates, but could have missed the angiosarcoma. Dermatopathologists should be familiar with the patterns of WIR and remember that some patients may develop multiple synchronous lesions requiring meticulous evaluation.
5. Future Directions
Recent advances in understanding the complex interplay between nerve stimuli—mediated by neuropeptides and other soluble neurotransmitters—and the dermoepidermal tissues are shedding light on wound repair processes and the pathogenesis of inflammatory cutaneous diseases. These findings are expected to provide valuable insights into the physiopathology of WIR and, more broadly, the concept of the “immunocompromised district”. Grouping phenomena such as WIR, the Koebner phenomenon, and similar reactions under this unified concept offer a cohesive framework that may facilitate further research and enhance our understanding of these processes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wolf R. Wolf D. Ruocco E. Brunetti G. Ruocco V. Wolf’s isotopic response Clin. Dermatol.2011292372402139656410.1016/j.clindermatol.2010.09.015 · doi ↗ · pubmed ↗
- 2Wyburn-Mason R. Malignant change arising in tissues affected by herpes Br. Med. J.19552110611091326067110.1136/bmj.2.4948.1106 PMC 1981341 · doi ↗ · pubmed ↗
- 3Wolf R. Brenner S. Ruocco V. Filioli F.G. Isotopic response Int. J. Dermatol.199534341348760779610.1111/j.1365-4362.1995.tb 03616.x · doi ↗ · pubmed ↗
- 4Happle R. Kluger N. Koebner’s sheep in Wolf’s clothing: Does the isotopic response exist as a distinct phenomenon?J. Eur. Acad. Dermatol. Venereol.2018325425432908031810.1111/jdv.14664 · doi ↗ · pubmed ↗
- 5Sanchez D.P. Sonthalia S. Koebner Phenomenon Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 553108/(accessed on 8 February 2025)31971748 · pubmed ↗
- 6Ruocco V. Ruocco E. Piccolo V. Brunetti G. Guerrera L.P. Wolf R. The immunocompromised district in dermatology: A unifying pathogenic view of the regional immune dysregulation Clin. Dermatol.2014325695762516009810.1016/j.clindermatol.2014.04.004 · doi ↗ · pubmed ↗
- 7Jenkins A.M. Skinner D. North J. Postherpetic isotopic responses with 3 simultaneously occurring reactions following herpes zoster Cutis 201810119519729718015 · pubmed ↗
- 8Schmidt A.P. Tjarks B.J. Lynch D.W. Gone fishing: A unique histologic pattern in cutaneous angiosarcoma Cutis 201810127027229763477 · pubmed ↗