Characteristics and outcomes of older patients undergoing out‐ versus inpatient surgery in Europe. A secondary analysis of the Peri‐interventional Outcome Study in the Elderly (POSE)
Linda Grüßer, Mark Coburn, Matthias Schmid, Rolf Rossaint, Sebastian Ziemann, Ana Kowark, Alina Schenk, Alina Schenk, Ralf‐Dieter Hilgers, Federico Bilotta, Leo C Bollheimer, Wolfgang Buhre, Ulf Guenther, Andreas Hoeft, Peter Lee, Idit Matot, Steffen Rex, Jacob Steinmetz

TL;DR
This study compares older patients undergoing outpatient versus inpatient surgery in Europe, finding that outpatients generally have better outcomes and lower mortality.
Contribution
The study provides new insights into the characteristics and outcomes of older patients in outpatient versus inpatient surgical settings in Europe.
Findings
Outpatients had fewer comorbidities, medications, and underwent minor procedures more often than inpatients.
Outpatients showed better baseline and follow-up functional and cognitive status compared to inpatients.
Outpatient surgery was associated with a significantly higher 30-day survival probability than inpatient surgery.
Abstract
The number of older patients undergoing surgical procedures with anaesthesia care is projected to rise. In order to cope with the increased demand, the expansion of outpatient surgery may play a decisive role. We aim to investigate the characteristics and outcomes of the older outpatient population. The Peri‐interventional Outcome Study in the Elderly in Europe (POSE) was a prospective multicenter study investigating characteristics and outcomes in 9497 patients aged 80 years and older undergoing a procedure with anaesthesia care. This secondary analysis of the POSE data investigated characteristics, functional and cognitive outcomes, and mortality in the outpatient in comparison to the inpatient population. Functional status was assessed as independent, partially dependent, and totally dependent at baseline and 30 days postinterventional. Cognitive status was defined by the number of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
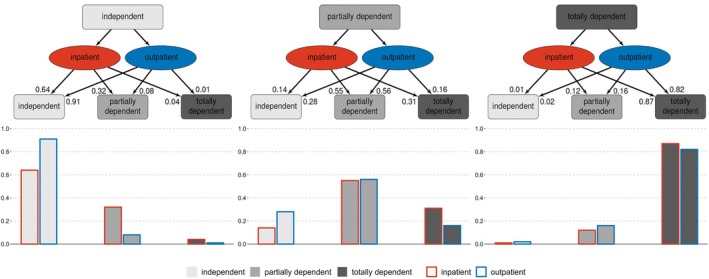 FIGURE 1
FIGURE 1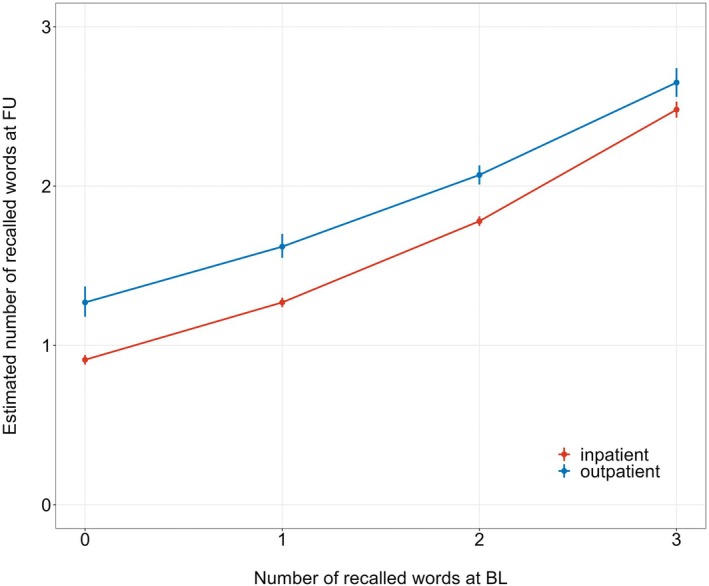 FIGURE 2
FIGURE 2| Outpatient ( | Inpatients ( | Overall ( | |
|---|---|---|---|
| Age (year) | 83.0 (81.0–86.0) | 84.0 (81.0–87.0) | 83.0 (81.0–86.0) |
| Sex | |||
| Male | 911 (47.1%) | 3574 (47.3%) | 4485 (47.2%) |
| Female | 1024 (52.9%) | 3988 (52.7%) | 5012 (52.8%) |
| Height (cm) | 164 (157–170) | 165 (159–171.0) | 165 (158.0–170.0) |
| Weight (kg) | 70.0 (61.0–79.0) | 70.0 (60.0–80.0) | 70.00 (60.0–80.0) |
| ASA score | |||
| 1 | 74 (3.8%) | 96 (1.3%) | 170 (1.8%) |
| 2 | 1023 (52.9%) | 2476 (32.7%) | 3499 (36.8%) |
| 3 | 808 (41.8%) | 4298 (56.8%) | 5106 (53.8%) |
| 4 | 29 (1.5%) | 663 (8.8%) | 692 (7.3%) |
| 5 | 0 (0%) | 23 (0.3%) | 23 (0.2%) |
| Referring facility | |||
| Home | 1765 (91.2%) | 6455 (85.4%) | 8220 (86.6%) |
| Other hospital | 8 (0.4%) | 176 (2.3%) | 184 (1.9%) |
| Rehabilitation | 3 (0.2%) | 57 (0.8%) | 60 (0.6%) |
| Nursing home | 74 (3.8%) | 596 (7.9%) | 670 (7.1%) |
| Other | 85 (4.4%) | 275 (3.6%) | 360 (3.8%) |
| Multimorbidity | 1319 (68.2%) | 6015 (79.5%) | 7334 (77.2%) |
| Haemoglobin (g dL−1) | 13.1 (11.8–14.2) | 12.4 (11.0–13.6) | 12.5 (11.1–13.7) |
| History of falls during the last 6 months | |||
| None | 1567 (81.0%) | 4859 (64.3%) | 6426 (67.7%) |
| 1 time | 244 (12.6%) | 1561 (20.6%) | 1805 (19.0) |
| >1 time | 105 (5.4%) | 1076 (14.2%) | 1181 (12.4%) |
| Limited timed up and go test | 1074 (55.5%) | 5387 (71.2%) | 6461 (68.0%) |
| Unintentional weight loss≥4.5kg in the last year | 238 (12.3%) | 1476 (19.5%) | 1714 (18.0%) |
| Functional status at baseline | |||
| Independent | 1431 (74.0%) | 4414 (58.4%) | 5845 (61.5%) |
| Partially dependent | 430 (22.2%) | 2473 (32.7%) | 2903 (30.6%) |
| Totally dependent | 73 (3.8%) | 670 (8.9%) | 743 (7.8%) |
| Mini‐Cog | |||
| 0 | 180 (9.3%) | 1212 (16.0%) | 1392 (14.7%) |
| 1–3 | 812 (42.0%) | 3189 (42.2%) | 4001 (42.1%) |
| 4–5 | 830 (42.9%) | 2831 (37.4%) | 3661 (38.5%) |
| Mini‐Cog − mean number of correctly recalled words | 2.01 ± 1.05 | 1.80 ± 1.12 | 1.84 ± 1.11 |
| Mini‐Cog − mean number of clock draw points | 1.11 ± 0.995 | 0.960 ± 0.999 | 0.989 ± 1.00 |
| Outpatients ( | Inpatients ( | Overall ( | ||
|---|---|---|---|---|
| Urgency | ||||
| Elective | 1891 (97.7%) | 5285 (69.9%) | 7176 (75.6%) | |
| Urgent | 33 (1.7%) | 1809 (23.9%) | 1842 (19.4%) | |
| Emergency | 11 (0.6%) | 468 (6.2%) | 479 (5.0%) | |
| Severity of surgery | ||||
| Minor | 895 (46.3%) | 1052 (13.9%) | 1947 (20.5%) | |
| Intermediate | 991 (51.2%) | 2621 (34.7%) | 3612 (38.0%) | |
| Major | 49 (2.5%) | 3889 (51.4%) | 3938 (41.5%) | |
| Type of intervention | ||||
| Abdominal | 62 (3.2%) | 1087 (14.4%) | 1149 (12.1%) | |
| Cardiovascular and thoracic | 47 (2.4%) | 849 (11.2%) | 896 (9.4%) | |
| ENT and ophthalmic | 970 (50.1%) | 624 (8.3%) | 1594 (16.8%) | |
| Gynaecologic and urological | 218 (11.3%) | 1219 (16.1%) | 1437 (15.1%) | |
| Interventional | 327 (16.9%) | 699 (9.2%) | 1026 (10.8%) | |
| Neurosurgery | 3 (0.2%) | 193 (2.6%) | 196 (2.1%) | |
| Orthopaedic, trauma and plastic | 233 (12.0%) | 2627 (34.7%) | 2860 (30.1%) | |
| Other surgery | 75 (3.9%) | 264 (3.5%) | 339 (3.6%) | |
| Laparoscopic surgery | 28 (1.4%) | 522 (6.9%) | 550 (5.8%) | |
| Cancer surgery | 132 (6.8%) | 1294 (17.1%) | 1426 (15.0%) | |
| Median anaesthesia duration (min) | 33.0 (23.0–55.0) | 105.0 (65.0–160) | 90.00 (48.0–142) | |
| Anaesthesia technique | ||||
| General | 438 (22.6%) | 4614 (61.0%) | 5052 (53.2%) | |
| Regional | 289 (14.9%) | 1339 (17.7%) | 1628 (17.1%) | |
| Sedation | 1021 (52.8%) | 734 (9.7%) | 1755 (18.5%) | |
| Combination | 187 (9.7%) | 875 (11.6%) | 1062 (11.2%) | |
| Premedication before the intervention | 463 (23.9%) | 1088 (14.3%) | 1551 (16.3%) | |
| Application of safe surgery checklist | 1397 (72.2%) | 5682 (75.1%) | 7079 (74.5%) | |
| Transfusion of platelets | 0 (0%) | 64 (0.8%) | 64 (0.7%) | |
| Transfusion of plasma | 0 (0%) | 141 (1.9%) | 141 (1.5%) | |
| Transfusion of RBC | 2 (0.1%) | 573 (7.6%) | 575 (6.1%) | |
| ICU admission | 11 (0.6%) | 1646 (21.8%) | 1657 (17.4%) | |
| Admission to geriatric support unit | 18 (0.9%) | 661 (8.7%) | 679 (7.1%) | |
| Mean hospital length of stay (days) | 0.173 ±1.60 | 7.31 ± 7.48 | 5.86 ±7.31 | |
- —The main study was supported by the European Society of Anaesthesiology and Intensive Care (ESAIC) as an ESAIC Research Group. MS received funding from the ESAIC POSE Research Group for this secondary
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Frailty in Older Adults · Intensive Care Unit Cognitive Disorders
INTRODUCTION
1
Worldwide, people aged 65 years and older are the fastest‐growing age group.1 In Europe, the number of older people aged 85 years and older is expected to increase by up to 130% from 2018 to 2050.2 These demographic changes suggest a sharp rise in the number of older patients undergoing surgical procedures with anaesthesia care. In order to cope with the increased demand in already overstrained health care systems, expansion of outpatient surgery may play a decisive role. Besides the economic benefits, it has been argued that older patients recover more rapidly from surgery within their familiar home environment with less disruption of their normal schedule.3 Furthermore, common risks of hospitalization, such as nosocomial infections, are reduced.4 However, little is known about the older outpatient population in Europe. It is unclear which older patients are currently being offered outpatient surgical care, and only a few studies have investigated outcomes after outpatient surgery.5 One international prospective multicentre cohort study in 372 older patients undergoing minor surgery revealed a lower incidence of postoperative cognitive dysfunction in older outpatients compared with inpatients.6 Of note, the prevalence rate of pre‐operative cognitive impairment in the older surgical outpatient population in the United States was already presented as slightly lower for the general and elective surgery population.7, 8, 9 Overall, studies investigating the advantages of enhanced recovery pathways on postoperative cognitive decline and functional status in the older patient population have shown shortened lengths of stay and beneficial outcomes.10, 11 However, these are not focused on outpatients.
The Peri‐interventional Outcome Study in the Elderly in Europe (POSE) was a prospective multi‐centre study investigating characteristics and outcomes in 9497 patients aged 80 years and older undergoing any kind of out‐ and inpatient surgical or nonsurgical procedure with anaesthesia care.12 The present secondary analysis of the POSE data is the first study that analyses the older European outpatient population. We aim to describe differences in the characteristics and outcomes in the outpatient in comparison to the inpatient population.
METHODS
2
Study design
2.1
We performed a secondary analysis of the prospective observational European multicentre POSE study.12 The original study was registered with ClinicalTrials.gov (NCT03152734), and the study protocol is available at www.pose-trial.org/study-documents. The study design has been described in detail previously.12 This secondary analysis was pre‐planned before the database closing, and the study proposal has been approved by the POSE Steering Committee.13 This work is reported in concordance with the STROBE statement. Following approval or a waiver from each respective centre's research ethics board (REB), written informed consent was obtained as required according to national laws.12 A separate REB approval for this secondary analysis was not required.
Setting, participants, and data collection
2.2
All analyses were based on the POSE study data. POSE analysed 9497 patients from 177 participating centres in 20 countries.12 Patients aged at least 80 years and undergoing any kind of surgical or nonsurgical intervention with anaesthesia care were included. For this secondary analysis, outpatients were defined as any patients having pre‐planned outpatient surgery with discharge on the day of intervention. Recruitment per centre took place during a 30‐day self‐selected period between October 2017 and December 2018. Data on the pre‐operative status, including medical conditions, cognitive and functional status, and intraoperative surgical and anaesthesia characteristics, were collected. Each patient was followed up for 30 days after the procedure. As previously described, all data was collected prospectively on paper‐based case report forms and entered into an electronic database (OpenClinica, Boston, Massachusetts, USA).12
Outcome measures and covariates
2.3
Based on the pragmatic case report form of the POSE study, the following outcome variables were analysed at baseline and follow‐up: Functional status (three categories: independent, partially dependent, and totally dependent14), cognitive status (defined at baseline by the number of recalled words (0–3) in the Mini‐Cog test,15 and—in order to enable a telephone‐follow up comparison—defined at follow‐up by the number of recalled words (0–3) in the brief cognitive screening by one item of the BSCI16) and time to death (ranging between 0 and 30 days, 388 observed deaths). Baseline data was collected in person at the hospital. Follow‐up was performed in person, in case the patient was still at the hospital, or via telephone, if the patient was already discharged.
The following nine covariates were identified as possible confounders: (1) age at baseline (years, modelled as continuous covariate with linear effect), (2) sex (male and female), (3) ASA classification (five categories, modelled as continuous covariate with linear effect), (4) kind of referring facility (home, other hospital, rehabilitation, nursing home, and other), (5) multimorbidity defined as the presence of at least two of the assessed comorbidities (yes and no), (6) timed up and go (TUG) test17 (limited mobility defined as TUG test performed in 12 s,18 normal), (7) history of falls (none, once, and more than once), (8) application of premedication (yes and no), (9) anaesthesia technique (general, regional, sedation, and combination). In addition, we considered severity of surgery (minor, intermediate, and major), urgency of surgery (elective, urgent, and emergency), and surgical category (abdominal, cardiovascular and thoracic, ears, nose and throat (ENT) and ophthalmic, gynaecologic and urologic, interventional, neurosurgery, orthopaedic, trauma and plastic, and other). However, we excluded these variables from analysis, as they were very strongly correlated with outpatient surgery or even determined the outpatient/inpatient status.
Bias
2.4
POSE aimed at minimizing selection bias and providing generalizable results by the consecutive recruitment of all eligible patients in a selected 30‐day recruitment period.12 Legally incompetent and emergency patients were also included. Measures to decrease the risk of attrition and detection bias were implemented.12
Statistical analysis
2.5
The statistical analysis was carried out on the basis of the cleaned and closed POSE database.12 Statistical analysis was performed using R, version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were summarized using means with SD and medians with the 25% and 75% quantiles. Categorical variables were summarized using counts with percentages.
Changes in functional status (baseline vs. follow‐up) were analysed using cross tabulations with McNemar's test. An ordinal logistic regression model with outcome variable ‘functional status at follow‐up’ and covariates ‘functional status at baseline’ and ‘outpatient vs. inpatient surgery’ (including an interaction term) was fitted to the analysis data. To adjust the analysis for the effects of possible confounder variables, we additionally fitted a multivariable ordinal logistic regression model with outcome variable ‘functional status at follow‐up’ and covariates ‘functional status at baseline’, ‘outpatient vs. inpatient surgery’ (including an interaction term between the two aforementioned covariates), and the nine covariates listed above to the analysis data. Likelihood ratio tests were used to compute p‐values for the effect of ‘outpatient vs. inpatient surgery’. p < .05 was considered statistically significant in all analyses. Missing values in the nine confounder variables were imputed using multiple imputation with 12 runs, as described elsewhere, and the model was fitted 12 times.12 Estimated probabilities of functional status at follow‐up were computed from these models by averaging predictions in the subgroups defined by ‘functional status at baseline’ and ‘outpatient vs. inpatient surgery’.
Changes in cognitive status (baseline vs. follow‐up) were analysed using cross tabulations with McNemar's test. Furthermore, a quasi‐Poisson regression model with outcome variable ‘number of recalled words at follow‐up’ and covariates ‘number of recalled words at baseline’ and ‘outpatient vs. inpatient surgery’ (including an interaction term) was fitted to the analysis data. To adjust the analysis for the effects of possible confounder variables, we additionally fitted a multivariable quasi‐Poisson regression model with outcome variable ‘number of recalled words at follow‐up’ and covariates ‘number of recalled words at baseline’, ‘outpatient vs. inpatient surgery’ (including an interaction term between the two aforementioned covariates), and the nine covariates listed above to the analysis data. Quasi‐likelihood ratio tests were used to compute p‐values for the effect of ‘outpatient vs. inpatient surgery’. Again, missing values were imputed using multiple imputation with 12 runs, and the model was fitted 12 times. Estimated means of the number of recalled words at follow‐up were computed from these models by averaging predictions in the subgroups defined by ‘number of recalled words at baseline’ and ‘outpatient vs. inpatient surgery’.
Time to death was analysed using Kaplan–Meier estimates (grouped by ‘outpatient vs. inpatient surgery’) with a log‐rank test. In addition, Cox regression models with covariate ‘outpatient vs. inpatient surgery’ and the nine possible confounders listed in Section 1 were fitted. The Cox model was also fitted 12 times using the imputed data sets. A 95% percent confidence interval for the pooled hazard ratio of ‘outpatient vs. inpatient surgery’ was computed using Rubin's rules.
For descriptive analysis, all missing values in the analysed variables were tabulated. Patients with a missing value in the outcome variables at baseline or follow‐up were excluded from the respective statistical analyses. Functional and cognitive status of patients who died during follow‐up were set to ‘totally dependent’ and ‘zero recalled words’ respectively.
RESULTS
3
Baseline and perioperative characteristics
3.1
Descriptive summaries of the variables at baseline and perioperative period are presented in Tables 1 and 2, respectively. There were no missing values in the binary variable with categories pre‐planned ‘outpatient vs. inpatient surgery’. Out of the 9497 patients, 7562 were planned as inpatients and 1935 as outpatients. There were no major differences between inpatients and outpatients with regard to age, sex, height, and weight. Overall, outpatients had less comorbidities and took fewer medications (Supplemental Table 1. Comorbidities and medication). This is also reflected within their ASA score. Outpatients were more often classified as ASA 1 and 2 compared with inpatients (56.7% vs. 34.0%). Fewer outpatients had a limited TUG test (55.5% vs. 71.2%) and reported ≥1 fall within the last 6 months (18% vs. 34.8%). In comparison to inpatients, outpatients' functional status was more often independent (74.0% vs. 58.4%), and they scored 4–5 points out of 5 possible points in the Mini‐Cog test more frequently (42.9% vs. 37.4%). They recalled three words at baseline more often (42.8% vs. 35.8%). The mean number of correctly recalled words was 2.0 (±1.1) in comparison to 1.8 (±1.1) in inpatients. Outpatients' referring facility was mostly from home (91.2% vs. 85.4%) and less often from a nursing home (3.8% vs. 7.9%) or other hospital (0.4% vs. 2.3%).
The type of intervention and the anaesthesia technique differed between the outpatient and inpatient populations. The most common types of interventions in outpatients were ENT (50.1% vs. 8.3%) and non‐surgical interventions (16.9% vs. 9.2%). Overall, in comparison to inpatients, outpatients more often had minor (46.3% vs. 13.9%) or intermediate procedures (51.2% vs. 34.7%), and the procedure was more often elective (97.7% vs. 69.9%). Outpatients underwent the respective interventions more often in sedation (52.8% vs. 9.7%). Accordingly, their median anaesthesia duration was shorter (33.0 min (23.0–55.0) vs. 105 min (65–160)).
Out of 1935 patients who were originally planned for an outpatient procedure, 101 patients (5.2%) eventually received inpatient care. The mean and median [min to max] length of stay for outpatients versus inpatients was 0.2 (±1.6) and 0 [0 to 31] versus 7.3 (±7.5) and 5 [0 to 31] days, respectively. There were 11 planned outpatients (0.6%) who were admitted to an ICU versus 1646 (21.8%) planned inpatients.
Outcomes
3.2
Functional status
3.2.1
Out of the 9497 patients in the POSE dataset, 8965 patients were included for the functional status analysis (Supplemental Table 2). Cross tabulations of functional status (baseline vs. follow‐up, all patients + grouped by outpatients vs. inpatients) are presented in Supplemental Table 3. p‐values of McNemar's test were<0.001 throughout, indicating significant changes. The estimated probabilities of functional status categories at follow‐up obtained from ordinal logistic regression are presented in Figure 1. In comparison to inpatients, outpatients had a higher estimated probability to stay independent (0.91 vs. 0.64).
Functional status. Figure showing the estimated probabilities of the categories of functional status at follow‐up (obtained from ordinal logistic regression).
The multivariable ordinal logistic regression models yielded similar results (Supplemental Table 4). The estimated probability for independent outpatients to maintain an independent functional status was 0.91 versus 0.63 for inpatients. Additionally, when removing the covariate ‘outpatient vs. inpatient surgery’ from the model, p‐values remained <0.001 in all 12 imputations, indicating a strong effect of this variable on functional status at follow‐up.
Cognitive outcome
3.2.2
Out of the 9497 patients, 8015 were included in the cognitive outcome analysis (Supplemental Table 2). Cross tabulations of cognitive status (baseline vs. follow‐up, all patients + grouped by outpatient vs. inpatient surgery) are presented in Supplemental Table 5. p‐values of McNemar's test were<0.001 throughout, indicating significant changes. The estimated number of recalled words at follow‐up was 2.15 for outpatients versus 1.78 for inpatients. The estimated means of the number of recalled words at follow‐up (obtained from quasi‐Poisson regression) are presented in Figure 2.
Number of recalled words. Figure showing the estimated means of the number of recalled words at follow‐up (quasi‐Poisson regression).
The estimated means of the number of recalled words at follow‐up obtained from multivariable quasi‐Poisson regression are presented in Supplemental Table 6. Removing the covariate ‘outpatient vs. inpatient surgery’ from the model resulted in p‐values that were<0.001 in all 12 imputations, indicating a strong effect of this variable on functional status at follow‐up.
Mortality
3.2.3
We observed 382 deaths in the inpatient group and 6 deaths in the outpatient group. The estimated 30‐day survival probabilities with 95% CI were 0.997 [0.994–0.999] in the group with planned outpatient surgery and 0.948 [0.942–0.953] in the group with planned inpatient surgery. Regarding time to death, the log‐rank test resulted in a p‐value <.001, indicating a strong effect of planned outpatient versus planned inpatient status on survival. In Cox regression, the planned outpatient versus inpatient status was strongly associated with survival, reducing the hazard of death by more than 80% after adjusting for possible confounding (pooled hazard ratio = 0.161 [0.071–0.366]).
Additional outcomes are presented in Supplemental Table 7.
DISCUSSION
4
To the best of our knowledge, this study is the first large‐scale analysis of older outpatients' characteristics and outcomes in Europe. Older outpatients presented with fewer comorbidities and fewer medications than older inpatients and underwent more often minor procedures. Our results indicate that functional and cognitive status at baseline were higher in outpatients than in inpatients, and the risk of postoperative deterioration was lower. Overall, outpatient interventions were associated with low mortality.
Weighing benefits against risks of interventions is difficult, particularly in the older patient population, but is likely to become a more frequent challenge in the near future. Besides survival, patient‐centred outcomes have come to the fore. Seriously ill older patients may not choose treatment for survival if that would go along with severe functional or cognitive impairment.19 Zhang et al. found that more than 20% of older inpatients who underwent a non‐orthopaedic surgical procedure experienced a functional decline.20 In comparison, the estimated probability for an independent older patient to maintain independent functional status was 0.91 in our outpatient population. The risk of becoming totally dependent was 0.01. In general, independent or partially dependent outpatients had higher probabilities to maintain or to improve their functional status in comparison to inpatients. For older patients who were already totally dependent at baseline, the differences were not as evident.
Similarly, we observed that outpatients had higher cognitive scores at baseline and at follow‐up. Thus, our results are in line with the scarce available evidence on cognitive outcomes after outpatient surgery.5, 6 It has repeatedly been shown that age is associated with adverse outcomes after surgery and that, in particular, older patients with preoperative cognitive impairment are vulnerable.21, 22 In our outpatient population, 50% of outpatients with 0 recalled words at baseline improved the number of recalled words at follow‐up. However, there may be considerable variations in the degree of cognitive impairment within a category, in particular within the ‘0 recalled words category’. It is crucial to underline that both functional and cognitive outcome measures in our analysis are based on very simple and short assessments that were part of the POSE study and not on recommended elaborate questionnaires such as the WHO Disability Assessment Schedule questionnaire (WHODAS).23, 24 It is unknown to what degree the classification of the functional status according to the ACS‐NSQIP used in our study correlates with the WHODAS or if recalling of words truly presents a rough surrogate for assessing changes in pre‐ and postoperative cognitive function.
Nevertheless, we detected differences between the two patient populations, confirming what has been suspected from daily clinical routine: Older patients who are being offered outpatient surgery are usually fitter, undergo less severe interventions, and have better outcomes. It is hence not surprising that the severity of surgery, urgency of surgery, and surgical category strongly correlated with or even determined the pre‐planned in‐ and outpatient status. Consequently, it is not possible to conclusively determine the extent to which the outpatient status or the type of intervention contributed to the positive outcome. What we can observe is that anaesthesiologists' clinical decisions appear to have identified a group of patients with similar characteristics, for whom outpatient surgery was an appropriate choice. Notably, 101 pre‐planned outpatients (5.2%) had a hospital stay longer than 1 day versus 44 pre‐planned inpatients (0.6%) who were discharged on the day of the procedure. Pre‐planned outpatients who had an unplanned hospital stay had a mean and median length of hospital stay of 3.32 ± 6.24 and 1 (1‐2) days, respectively. In comparison to pre‐planned outpatients who stayed outpatients, they underwent more often major surgeries and received more often a general anaesthesia than a sedation (Supplemental Table 8). Their baseline cognitive and functional status were lower, but their sample size was too small to derive meaningful predictors for outcomes or a successful outpatient status. Developing scores and guidelines that facilitate the identification of patients suitable for outpatient surgery is essential to enhance patient safety and efficiency.25, 26 Larger study populations and multicentre ranomised controlled trials are needed to build and validate such scores for older patients. Further research should also focus on the development of postoperative outpatient support systems, such as telemedical support. Embracing patient empowerment concepts, the decision of whether an older patient is suited for outpatient surgery should always be made together with the patient, considering their domestic environment and availability of family member support. The shared decision model has been proposed to incorporate an individualized approach to perioperative care.27, 28
Our study comes along with several limitations. First and foremost, this is a secondary analysis of the POSE study and not a study designed for investigating functional and cognitive outcomes among outpatients and inpatients.12 Questions relating to the cognitive and functional status were restricted to a minimum to enable voluntary participation of 177 study centres across Europe. Our multivariable analysis accounted for important variables associated with functional and cognitive outcomes, but we acknowledge the risk of unmeasured confounding, for example, we could not adjust for years of education or social determinants. Even though we adjusted for the kind of anaesthesia, the effects of different anaesthesia regimes on cognitive decline in older patients require further investigation.29 Also, we did not adjust for random centre effects or differences among the national health care systems. In general, limitations of the POSE data collection apply to our analysis as well.12 It is important to consider that participating POSE centres were mainly tertiary or academic secondary hospitals.12 It remains unclear whether older outpatients in Europe are generally more likely to undergo outpatient surgery in such a setting or if a considerable proportion also undergo interventions with anaesthesia care in primary care facilities. Older patients receiving outpatient care in primary care facilities may have even fewer comorbidities and favourable outcomes. Overall loss‐to‐follow‐up rates in the main POSE study can be considered low.12, 30 Nevertheless, it could be argued that patients who died during the follow‐up period should not have been classified in the lowest category of the respective outcomes. However, excluding these patients from the present analysis entirely may have led to even more biased estimations.
Overall, this secondary analysis demonstrates that older patients in Europe underwent outpatient surgery with a low risk of mortality. In comparison to inpatients, they presented with fewer comorbidities and higher functional and cognitive baseline status. They underwent more often minor procedures with minimal anaesthesia techniques and had better postoperative functional and cognitive scores. Further studies designed to assess functional and cognitive outcomes after outpatient surgery are needed to develop scores that facilitate the identification of older patients suited for outpatient surgery.
AUTHOR CONTRIBUTIONS
Linda Grüßer: Methodology, investigation, data curation, validation, visualization, and wrote the original draft. Mark Coburn: Conceptualization, methodology, validation, supervision, project administration, writing—review and editing. Matthias Schmid: Methodology, software, formal analysis, visualization, writing—review and editing. Rolf Rossaint: Conceptualization, project administration, writing—review and editing. Sebastian Ziemann: Data curation, writing—review and editing. Ana Kowark: Conceptualization, methodology, data curation, validation, supervision, writing—review, and editing. POSE Study group: Data acquisition.
FUNDING INFORMATION
The main study was supported by the European Society of Anaesthesiology and Intensive Care (ESAIC) as an ESAIC Research Group. MS received funding from the ESAIC POSE Research Group for this secondary analysis. The remaining authors report no funding for this secondary analysis.
CONFLICT OF INTEREST STATEMENT
Outside the submitted work, LG reported payment for a lecture, Baxter Germany GmbH; MC reported payments for lectures, Baxter Germany GmbH, Drägerwerk AG & Co. KGaA, Ambu GmbH; RR reported being a cofounder of Docs in Clouds GmbH; AK reported being a member of the advisory board of PAION.
Supporting information
Supplemental Table 1. Comorbidities and medication.
Supplemental Table 2. Study population.
Supplemental Table 3. Cross tabulations of functional status at baseline and follow‐up. (a) All patients, (b) outpatients, (c) inpatients.
Supplemental Table 4. Multivariable ordinal logistic regression—functional status.
Supplemental Table 5. Cross tabulations of cognitive status at baseline and follow‐up. (a) All patients, (b) outpatients, (c) inpatients.
Supplemental Table 6. Multivariable quasi‐Poisson regression—cognitive status.
Supplemental Table 7. Additional outcomes of outpatients and inpatients.
Supplemental Table 8. Baseline characteristics, perioperative characteristics and outcomes of planned outpatients with no and with unplanned stay.
Data S1: POSE‐study group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Population Division of the United Nations Department of Economic and Social Affairs . World Population Prospects 2019: Highlights. 2019.
- 2Eurostat . Ageing Europe. Looking at the lives of older people in the EU. 2019 https://ec.europa.eu/eurostat/documents/3217494/10166544/KS‐02‐19%E 2%80%91681‐EN‐N.pdf/c 701972 f‐6b 4e‐b 432‐57d 2‐91898 ca 94893 (Accessed: 02 Mar 2025).
- 3White PF , White LM , Monk T , et al. Perioperative care for the older outpatient undergoing ambulatory surgery. Anesth Analg. 2012;114:1190‐1215.22467899 10.1213/ANE.0b 013e 31824 f 19b 8 · doi ↗ · pubmed ↗
- 4Aurini L , White PF . Anesthesia for the elderly outpatient. Curr Opin Anaesthesiol. 2014;27:563‐575.25318569 10.1097/ACO.0000000000000135 · doi ↗ · pubmed ↗
- 5Rasmussen LS , Steinmetz J . Ambulatory anaesthesia and cognitive dysfunction. Curr Opin Anaesthesiol. 2015;28:631‐635.26308519 10.1097/ACO.0000000000000247 · doi ↗ · pubmed ↗
- 6Canet J , Raeder J , Rasmussen LS , et al. Cognitive dysfunction after minor surgery in the elderly. Acta Anaesthesiol Scand. 2003;47:1204‐1210.14616316 10.1046/j.1399-6576.2003.00238.x · doi ↗ · pubmed ↗
- 7Gaulton TG , Eckenhoff RG , Neuman MD . Prevalence and multivariable factors associated with preoperative cognitive impairment in outpatient surgery in the United States. Anesth Analg. 2019;129:e 5‐e 7.31210651 10.1213/ANE.0000000000004035 · doi ↗ · pubmed ↗
- 8Culley DJ , Flaherty D , Reddy S , et al. Preoperative cognitive stratification of older elective surgical patients: a cross‐sectional study. Anesth Analg. 2016;123:186‐192.27028776 10.1213/ANE.0000000000001277 PMC 4912429 · doi ↗ · pubmed ↗