Changes in Mental and Physical Health Outcomes Following One Day a Week Cardiopulmonary Rehabilitation in Regional New South Wales
Nnamdi Mgbemena, Jane Thompson, Uchechukwu Levi Osuagwu

TL;DR
A weekly cardiopulmonary rehabilitation program in regional NSW improved both mental and physical health outcomes for patients with heart or lung diseases.
Contribution
Demonstrates effectiveness of a low-frequency rehabilitation program in a resource-limited regional setting.
Findings
Participants showed significant improvements in depression scores, physical endurance, and waist circumference after the program.
The proportion of participants with major depression decreased by 50% post-rehabilitation.
Both cardiac and pulmonary rehabilitation participants experienced significant mental health improvements.
Abstract
Cardiopulmonary rehabilitation participation rates in regional Australia remain poor, with outcomes further worsened by the limited number of cardiopulmonary rehabilitation professionals in these settings. This study investigated the role of cardiopulmonary rehabilitation in improving physical and mental health outcomes of participants with heart or lung diseases in a regional NSW centre. A retrospective study of adults who attended a 1‐h session per week cardiac or pulmonary rehabilitation programme at Bathurst Hospital between January 2021 and December 2023. Pre‐ and post‐rehabilitation assessments were conducted, which included heart rate, blood pressure, oxygen saturation, waist circumference, rating of perceived exertion, 5‐sit‐to‐stand test (5‐STS), 6‐min walk test (6MWT), and the patient health questionnaire‐9 for assessment of depression (PHQ‐9 score ≥ 10 = major depression).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
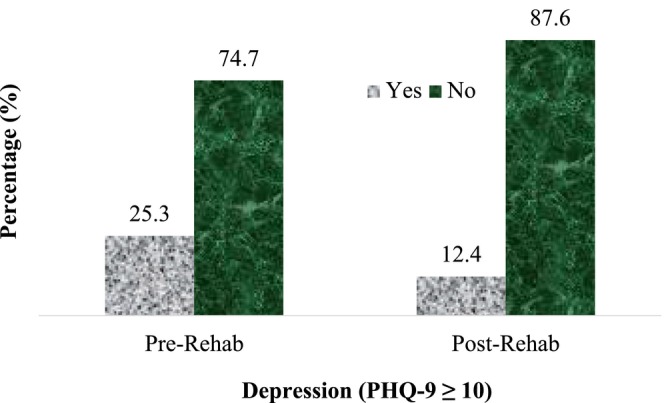 FIGURE 1
FIGURE 1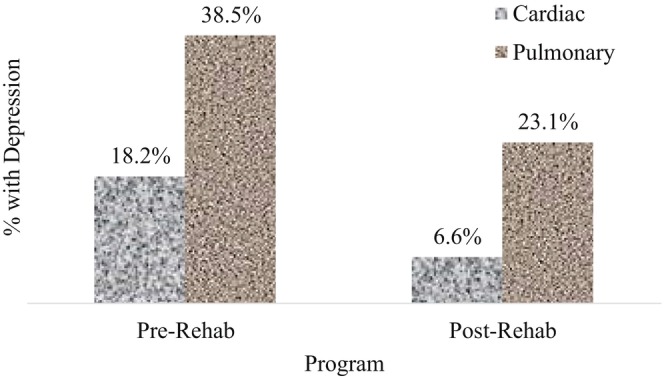 FIGURE 2
FIGURE 2| Variables | Frequency, |
|---|---|
| Demography | |
| Sex, males | 107 (57.5%) |
| Age (years) | 69.34 (12.58) |
| Weight (kg) | 87.87 (21.88) |
| Height (m) | 1.69 (0.11) |
| Body mass index (kg/m2) | 30.7 (8.32) |
| Year of enrolment | |
| 2021/2022/2023 | 44 (23.7%)/57 (30.7%)/85 (45.7%) |
| Type of program, | |
| Cardiac/pulmonary | 121 (65%)/65 (35%) |
| Baseline measures | |
| Heart rate (beats/min) | 75.1 (13.5) |
| Waist circumference (cm) | 104.7 (16.1) |
| 5 Sit‐to‐Stand (seconds) | 15.8 (7.4) |
| Six‐minute walk test (m) | 328.6 (92.1) |
| Systolic blood pressure (mmHg) | 133 (18) |
| Diastolic blood pressure (mmHg) | 77 (10) |
| SPO2 (%) | 96.2 (2.1) |
| Handgrip strength ( | |
| Right | 29.9 (11.6) |
| Left | 28.9 (11.3) |
| Borg Scale | 0.31 (0.04) |
| Cardiac rehabilitation referring conditions, | |
| Coronary artery disease/isolated CABG | 30 (24.7%)/28 (23.1%) |
| Poor exercise tolerance/other cardiac surgeries | 16 (13.2%)/9 (7.4%) |
| NSTEMI+coronary angiography/isolated AVR | 7 (5.7%)/6 (4.9%) |
| Isolated MVR/cardiomyopathy | 6 (4.9%)/5 (4.9%) |
| Chronic heart failure/CABG+valvular replacement | 4 (3.3%)/3 (2.4%) |
| Not given/angina | 3 (2.4%)/2 (1.6%) |
| Atrial fibrillation/infective carditis | 2 (1.6%)/1 (0.8%) |
| Pulmonary rehabilitation referring conditions, | |
| COPD/long COVID symptoms/poor exercise tolerance | 26 (40.0%)/19 (29.3%)/8 (12.3%) |
| Shortness of breath/lobectomy/IPF | 4 (6.2%)/3 (4.6%)/2 (3.1%) |
| ILD/pneumonia/not given | 1 (1.5%)/1 (1.5%)/1 (1.5%) |
| All participants ( | Mean difference (95% CI) |
| Change (%) |
|---|---|---|---|
| Heart rate (beats/min) | 1.48 (−0.16, 3.12) | 0.076 | −1.99 |
| Waist circumference (cm) | 0.79 (0.27, 1.31) |
| −0.75 |
| 5 Sit‐to‐stand (seconds) | 3.21 (2.33, 4.10) |
| −20.83 |
| Six‐minute walk test (m) | −49.27 (−57.53, −41.01) |
| 14.9 |
| Systolic blood pressure (mmHg) | 2.23 (−0.20, 4.82) | 0.071 | −1.73 |
| Diastolic blood pressure (mmHg) | 1.14 (−0.21, 2.49) | 0.098 | −1.49 |
| SPO2 | −0.12 (−0.47, 0.24) | 0.510 | 0.12 |
| 2021 Enrolment | 44 (23.7%) | ||
| 2022 Enrolment | 57 (30.7%) | ||
| 2023 Enrolment | 85 (45.7%) | ||
| Cardiac rehabilitation participants ( | |||
| Heart rate (beats/min) | 1.88 (−0.06, 0.38) | 0.058 | −2.60 |
| Waist circumference (cm) | 0.66 (0.02, 1.31) |
| −0.63 |
| 5 Sit‐to‐Stand (seconds) | 3.42 (2.29, 4.55) |
| −22.09 |
| Six‐minute walk test (m) | −52. 41 (−62.53, −42.30) |
| 15.47 |
| Systolic blood pressure (mmHg) | 2.07 (0.10, 5.14) | 0.183 | −1.58 |
| Diastolic blood pressure (mmHg) | 0.88 (−0.83, 2.60) | 0.309 | −1.16 |
| SPO2 | 0.05 (−0.28, 0.38) | 0.766 | −0.05 |
| 2021 Enrolment | 25 (20.7%) | ||
| 2022 Enrolment | 38 (31.4%) | ||
| 2023 Enrolment | 58 (47.9%) | ||
| Pulmonary rehabilitation participants ( | |||
| Heart rate (beats/min) | 0.75 (−2.31, 3.82) | 0.625 | −0.95 |
| Waist circumference (cm) | 1.02 (0.14, 1.91) |
| −0.96 |
| 5 Sit‐to‐stand (seconds) | 2.83 (1.39, 4.28) |
| −17.32 |
| Six‐minute walk test (m) | −43.42 (−57.98, −28.85) |
| 14.01 |
| Systolic blood pressure (mmHg) | 2.75 (−1.71, 7.21) | 0.222 | −2.00 |
| Diastolic blood pressure (mmHg) | 1.62 (−0.64, 3.87) | 0.157 | −2.09 |
| SPO2 | −0.43 (−1.25, 0.38) | 0.295 | 0.45 |
| 2021 Enrolment | 19 (29.2%) | ||
| 2022 Enrolment | 19 (29.2%) | ||
| 2023 Enrolment | 27 (41.6%) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Health and Mental Health · Chronic Obstructive Pulmonary Disease (COPD) Research · Frailty in Older Adults
Summary
-
What is already known on this subject?
-
○Attending cardiac or pulmonary rehabilitation has been shown to reduce mortality rates and hospital readmissions; however, there is limited information on the impact of these programmes in rural and remote Australia.
-
○There are still poor cardiac and pulmonary rehabilitation participation rates in Australia, which necessitate the need for greater awareness of the benefits of these programmes, especially in rural and remote Australia.
-
What this study adds?
-
○This study contributes to the growing body of evidence supporting the benefits of cardiac and pulmonary rehabilitation programmes in improving health outcomes for individuals living with cardiovascular and respiratory conditions.
-
○Attending even one session per week of cardiac or pulmonary rehabilitation can yield positive outcomes for participants, particularly in settings where resources are scarce.
-
○Investing in and prioritising the dissemination of rehabilitation services in low resource areas in Australia becomes essential step toward fostering equitable access to quality healthcare for all.
Introduction
1
Cardiopulmonary rehabilitation is a multi‐component intervention offered to patients with heart or lung disease, which helps to improve their functional capacity and quality of life and reduce symptoms of dyspnoea and fatigue [1, 2]. In clinical practice, cardiopulmonary rehabilitation is designed as two independent programmes that are personalised to the participant's needs, where cardiac rehabilitation (CR) is run for 6–10 weeks, while pulmonary rehabilitation (PR) runs for 8 weeks [3, 4].
Introduced in the late 1960s, CR has greatly evolved over the last two to three decades. The programme has developed a large evidence base, the majority suggesting that comprehensive CR should also be targeted at participants with acute coronary syndrome (ACS), percutaneous coronary intervention, or who have undergone cardiac surgeries (coronary artery bypass graft and valvular replacement or repair) [5]. In Australia, existing data showed that 92,400 adults were admitted to the hospital on account of ACS between 2020 and 2021, with an estimated annual mortality rate of 12% [6, 7]. A recent study conducted in New South Wales, Australia, highlighted an increased incidence of emergency presentations and hospital readmissions for ACS among those living in the Hunter New England region compared to the metropolitan areas, reflecting the existing reality of poorer and inadequate specialised health care services in rural settings [8]. Despite the robust evidence of CR in reducing mortality rates and hospital readmissions, there is still a poor CR estimated participation rate of 30% in Australia [9]. Studies have attributed this low uptake in Australia to poor referral rates, poor access to services and adherence, and suboptimal sustainability [10].
Similarly, PR, which involves structured, multidisciplinary education, supervised exercises and psychosocial support, was originally targeted at patients diagnosed with chronic obstructive pulmonary disease (COPD), with recent clinical recommendations to offer this programme to patients with bronchiectasis, interstitial lung disease and pulmonary hypertension [2]. In Australia, approximately 53,000 adults aged 45 and above were hospitalised on a account of COPD between 2021 and 2022, with a mortality rate of 29.6 per 100,000 people in 2022 [11]. The prevalence of COPD is higher in rural and remote areas (3.9%) compared to urban settings (2.2%), with socio‐economic factors being a significant determinant of this disparity. Consequently, rural areas report elevated rates of both hospital admissions and mortality due to COPD compared to metropolitan areas [11]. Despite the demonstrated evidence of the positive effects of PR, poor participation (< 1.2%) remains a common finding in developed countries (Australia, New Zealand, Canada, Ireland, Sweden, the United Kingdom and the United States) [12]. In Australia, a prospective study reported that one‐third of patients with acute exacerbated COPD were referred to PR [13], while less than one‐fifth of the patients with stable COPD attended and completed at least half of the PR programme [14]. Also, prior studies among medical practitioners identified barriers to referral and adherence to PR, including poor knowledge of PR for the COPD population, unclear understanding of the referral process, access or travel difficulties and not being sure of the need to do more to achieve a behaviour change [15, 16].
Considering that heart disease and COPD remain the first and third leading causes of death globally, respectively, and the expected poorer participation rates in cardiopulmonary rehabilitation in regional and rural areas [17, 18, 19], there is still a need to reiterate the importance of these programmes in improving the physical and mental health outcomes of people living in regional and rural Australia. Therefore, this study was designed to demonstrate the role of cardiopulmonary rehabilitation in improving physical and mental health outcomes in patients with heart or lung diseases. It is expected that a significant improvement in health outcomes in these individuals would encourage participation in cardiopulmonary rehabilitation in adults living in these areas, where there remains a dearth of information on the impact of these programmes.
Methods
2
Study Design and Setting
2.1
This was a retrospective study of participants who attended the Cardiopulmonary rehabilitation centre at Bathurst Hospital, New South Wales, between January 2021 and December 2023. Participants were either referred to the CR or PR programme by health professionals or were self‐referred. Pre‐rehabilitation assessments were conducted by a nurse or physiotherapist at week 0, while post‐rehabilitation assessments were performed by the same health professional on the final day of week 6 for the CR programme and week 8 for the PR programme, based on the programme's current staffing availability.
Ethical Consideration
2.2
The study followed the tenets of the Declaration of Helsinki for human subjects (as revised in Brazil 2013). Prior to data collection, ethics approval for the study was obtained from the Western New South Wales Local Health District; Greater Western Human Research Ethics Committee, University Research Ethics Committee (2021/ETH00556). All participants provided written informed consent before data collection for the use of their data for research purposes.
Inclusion and Exclusion Criteria
2.3
Participants were included in this study if they were adults (aged 18 years and above), completed their rehabilitation programme in Bathurst Hopsital Centre within the study duration and had pre‐ and post‐rehabilitation data for the measured outcomes recorded in their hospital records. Those with incomplete demographic and/or clinical data for the studied variables were excluded.
Data Collection
2.4
Participants' socio‐demographic data including age, sex, height, weight and referring condition/reason were retrieved from their electronic medical records by the nursing team. Physical measures (heart rate, blood pressure, oxygen saturation levels, waist circumference, handgrip strength [HGS], rating of perceived exertion, 5‐sit‐to‐stand test [5‐STS], 6‐min walk test [6MWT]) and mental health measures (patient health questionnaire‐9, PHQ‐9) were obtained before and after they completed the rehabilitation programme. These assessments were done under the essential and desirable cardiac rehabilitation best practice statements on the content to be delivered in phase II CR programme [20]. Participants' blood pressure, heart rate and oxygen saturation testing were done in this order, followed by 6MWT, HGS testing in standing, 5‐STS, waist circumference and filling out the PHQ‐9. Participants' baseline perceived exertion was assessed using the modified Borg scale with the participants in a seated position. These assessments were conducted by a trained health professional following standardised recommendations [21, 22, 23].
The Main Outcome
2.5
The main outcome variable was the level of depression which was measured using the PHQ‐9, a nine‐item instrument based on Diagnostic and Statistical Manual criteria for major depressive disorders, and has been validated in the cardiac population [24]. Each item is rated on a 0–3 (0 = ‘not at all’ to 3 = ‘nearly every day’) scale, which relates to the frequency of the symptoms. This questionnaire is scored out of 27, with the depressive symptom severity categorised as minimal (0–4), mild [5, 6, 7, 8, 9], moderate [10, 11, 12, 13, 14], moderately severe [15, 16, 17, 18, 19] and severe [20, 21, 22, 23, 24, 25, 26, 27]. The scores were recategorised as ‘no depression’ for scores ≤ 9 and ‘depression’ for scores ≥ 10 based on its reported sensitivity and specificity of 88% in diagnosing major depressive disorder [25].
Description of the Cardiopulmonary Rehabilitation Programmes
2.6
On the first day of enrolment, all participants discussed with staff to set their goals for the programme and underwent individualised initial clinical, physical and psychosocial assessments by the cardiopulmonary rehabilitation team. The team comprised two part‐time nurses (registered and enrolled) with a combined equivalent of 42 h per week and a physiotherapist who works 2 h per week. The cardiac and pulmonary rehabilitation programmes at the Bathurst Health Service are designed as a 6‐ and 8‐week programme, respectively, where each participant attends one class (approximately 1 h) per week. Compared to the traditional structured programmes of 6–8 weeks in other regions, this short duration ‘half‐program’ was designed to accommodate the lack of qualified staff and other health professionals including exercise physiologists, dietitians and psychologists in this regional area.
Both programmes (cardiac and pulmonary rehabilitation) involve aerobic exercise training, strengthening exercise and education on strategies to control cardiovascular disease risk factors. Although there are variations in pace for the CR and PR programmes, their exercise routine is basically the same as per the recommendations of Heart Foundation Australia and Lung Foundation Australia [3, 4]. The aim of using the same exercises is to strengthen similar antigravity muscles and improve functional capacity, which is relevant for persons attending either CR or PR programme [26].
The aerobic exercises involve a 15‐min walking programme where participants get into a moderate—somewhat hard intensity (using the modified Borg scale) walk and another 15 min of either cycling, walking, or rowing at a moderate—somewhat hard intensity (using the modified Borg scale).
The muscular strengthening exercises are incorporated between two aerobic exercises and consist of a 15‐min routine targeting the upper limbs, lower limbs and core muscles. For the upper limbs, exercises include biceps curls using a 1 kg dumbbell in each hand (2 sets of 15 repetitions), progressing every 2 weeks by increasing the weight by 0.5 kg per hand and forward punches (based on participants' shoulder mobility) for 2 sets of 15 repetitions, progressing every 2 weeks by adding an extra set of 15 repetitions. For the lower limbs, exercises include sit‐to‐stand movements (without weights) for 2 sets of 15 repetitions, seated knee extensions (without weights) for 2 sets of 15 repetitions, seated heel raises for 2 sets of 15 repetitions and step‐ups and step‐downs using an aerobic stepper for 2 sets of 15 repetitions per limb. Each lower limb exercise progresses every 2 weeks by adding a 0.5 kg weight to each hand (for sit‐to‐stand and step‐ups) or each ankle (for knee extensions and heel raises).
Core strengthening includes high knee stepping in standing for 15 repetitions per limb, progressing every 2 weeks by adding an extra set of 15 repetitions. Balance exercises, performed within parallel bars for support, include tandem stance (each limb positioned in front for 30 s, 2 sets) and single leg stance (each limb raised for 30 s, 2 sets). These exercises progress every 2 weeks by adding an extra set of 30 s per limb. For the home programme, participants received an exercise sheet with two strengthening exercises for the upper and lower limbs and one balance exercise. These were adapted from their current routine in the programme to suit their home environment. These exercises are written with clear instructions following the Heart Foundation and Lung Foundation, Australia [2, 27].
Data Analysis
2.7
The data of all consenting participants who enrolled in the CR programme from January 2021 to December 2023 were included in this study. The normality of the data was tested using the Kolmogorov–Smirnov test and Lilliefors correction, with more than half of the variables identified not to be normally distributed. However, the application of the central limit theorem allowed the use of parametric statistical analysis for the data [28]. All results were presented as mean (standard deviation) or frequency (percentages). All analyses were two‐tailed, and p < 0.05 was considered statistically significant. Differences between pre‐ and post‐measurements of the mental (PHQ‐9) and physical (heart rate, blood pressure, oxygen saturation levels, waist circumference, HGS, rating of perceived exertion, 5‐STS and 6MWT) outcome variables of the participants were assessed using the paired t‐tests. Differences in depression scores between pre‐ and post‐measurements and rehabilitation programme types were determined using the Chi square test. One‐way analysis of variance (ANOVA) was used to determine the effect of the enrolment year on the main outcome variable. All analyses were conducted using the Statistical Package for the Social Sciences, version 29.0 (IBM Corp., Armonk, N.Y., USA).
Results
3
Demographic and Clinical Characteristics
3.1
Data from 205 adults who attended these programmes over the study period were available, but only the data for the 186 participants (90.7%) who completed the pre‐ and post‐rehabilitation assessments for the outcome measures were included in the analysis. Nineteen participants were excluded because they did not have complete demographic and/or clinical information. Of those included in the analysis, a summary statistic of their demographic and clinical characteristics is shown in Table 1. The characteristics of the participants included in this study were comparable with those of the excluded participants (p > 0.05) except for the 6MWT mean score.
More than half of the participants were males (57.5%), with a higher mean BMI (30.7 ± 8.3 kg/m^2^) and the average age was 69 years. The average waist circumference was 104.7 (±16.1) cm. Sixty‐five per cent were attending the cardiac rehabilitation program. The primary diagnoses for participation for those in the CR programme were coronary artery disease and isolated CABG surgery and for those in the PR program, COPD and long COVID symptoms were their primary diagnoses (Table 1).
Mental and Physical Health Outcomes
3.2
Figure 1 presents the prevalence of depression in this study population and showed that 25.3% had major depressive disorder (PHQ‐9 ≥ 10) at the time of enrolment, which reduced by 50% at the completion of the programme (p < 0.05).
Comparison of pre‐ and post‐rehabilitation data according to the presence of depression.
Figure 2 shows that participants who attended PR had a higher prevalence of major depressive disorder than CR participants at enrolment. However, in both groups, significant reductions (p < 0.05) in major depressive disorder were observed post‐rehabilitation, with 11.6% and 15.4% reductions in the CR and PR participants, respectively (Figure 2).
Comparison of the presence of depression across pre‐ and post‐rehabilitation data according to the type of programme attended.
Table 2 presents the mean differences (post minus pre) in measured variables for programme participants, while the absolute values (mean and standard deviation) are provided in Table S1. The enrolment years (2021, 2022 and 2023) had no significant influence on the measured variables (One‐way ANOVA, p > 0.05). Regarding the physical measures in all participants, and within the PR and CR groups, waist circumference, 5 Sit‐to‐Stand and 6MWT showed statistically significant changes post‐intervention. The time to complete the 5‐STS was reduced by 22% and 17% for participants in the CR and PR programmes, respectively, compared to pre‐rehabilitation values.
Discussion
4
The findings of this study showed the significant impact of a short rehabilitation programme in regional NSW. Participants attending cardiac or pulmonary rehabilitation programmes significantly improved their mental and physical health, especially depressive symptoms, time to complete 5‐STS, 6MWT distance and waist circumference. In contrast, blood pressure, heart rate and blood oxygen saturation levels were similar between pre‐ and post‐rehabilitation assessments. Despite the progressive increase in the number of enrolments since 2021 following the COVID‐19 pandemic, the year of enrolment was not identified as a significant contributor to these pre‐ and post‐rehabilitation changes identified in the improved variables. Overall, the current study showed that in regional and rural settings, where there is a limited number of health professionals to conduct standard, twice to thrice per week CR rehabilitation programmes, attending a 1‐day CR programme weekly is still adequate to elicit improvements in the level of depression and physical function of an individual.
Given the increasing prevalence of depression among patients living with cardiac and respiratory diseases, attending rehabilitation programmes has been shown to have beneficial effects on a patient's mental well‐being [29, 30]. The findings of a decrease in the proportion experiencing major depression post‐rehabilitation are congruent with previous studies conducted among individuals who attended CR or PR programmes [30, 31, 32, 33] elsewhere. This improvement could be partly attributed to the social interaction of participating in cardiopulmonary rehabilitation, where participants interact, support each other and recount their personal experiences, potentially serving as a means to alleviate apprehension among participants [34]. Further, this improvement could be due to the reported anti‐depressant effects of exercises in reshaping the brain structure, promoting behavioural adaptation changes, and maintaining the integrity of the hippocampus and white matter of the brain [35]. These neurophysiological changes enhance the nervous system processing and delay cognitive deterioration in depressed patients [36].
This study found an improvement in the time to complete the 5‐STS test, which was similar to previous studies [37, 38] that reported stronger lower limb muscles, improved balance and low falls risk among participants who attended cardiorespiratory rehabilitation [39, 40]. This is explained by the impact of cardiac and respiratory diseases in causing reduced involvement in physical activity, with concomitant alterations in skeletal muscle metabolism, systemic inflammation and decreased muscle capillary density, which leads to generalised muscle atrophy [41]. Further, these processes are accelerated by the possible sarcopenic profile of these patients, as previous studies have reported positive associations between sarcopenia and cardiac or pulmonary diseases [42, 43]. This explains why one of the core components of cardiac and pulmonary rehabilitation programmes is graded strengthening exercises of the limbs. Improvement in lower limb muscle strength whilst maintaining optimal balance requires the coordination of several lower limb and trunk muscle groups and thus is an essential component of independence [37].
Another significant finding of this study was the reduction in waist circumference post‐rehabilitation programme. Rehabilitation programmes often incorporate physical activity components, such as cardiovascular exercise and strength training, which can contribute to overall weight loss and reductions in abdominal fat, including waist circumference. Also, improvements in dietary habits and lifestyle behaviours, commonly addressed in rehabilitation programmes, may contribute to reductions in waist circumference. Participants may adopt healthier eating patterns and decrease their intake of calorie‐dense foods, leading to reductions in abdominal fat. This finding aligns with previous work by Greenwood et al. [44] and Silva et al. [45] demonstrating the effectiveness of rehabilitation programmes in reducing waist circumference. In that study [44], the authors found that exercise‐based rehabilitation programmes were associated with significant reductions in waist circumference among individuals with CKD. Silva et al. [45] reported significant reductions in waist circumference following a multidisciplinary rehabilitation programme for individuals with obesity. Overall, the reduction in waist circumference observed post‐rehabilitation programme likely reflects the multifaceted approach of these interventions, which target both physical activity and dietary behaviours to promote weight loss and improvements in body composition. Further research is warranted to elucidate the specific mechanisms underlying these effects and to optimise the design and implementation of rehabilitation programmes for individuals seeking to reduce abdominal fat and improve overall health.
Limitations and Strengths of the Study
4.1
The study has several limitations to consider. First, there was no control group, which prevents direct comparison between participants attending rehabilitation programmes and those not participating, potentially affecting the attribution of observed improvements solely to the programmes. Second, the small sample size and voluntary enrolment in cardiac or pulmonary rehabilitation programmes may introduce selection bias, with enrolled individuals possibly more motivated to improve their health outcomes, thus possibly overestimating programme effectiveness. Third, the study was conducted in a regional and rural setting, which may limit the generalisability of the findings to other settings with better access to healthcare services and resources. Fourth, the lack of longer‐term follow‐up data prevents insights into the sustainability of observed improvements over time and the potential need for ongoing support or intervention. Lastly, while the study assessed several outcome measures, important variables such as quality of life and medication adherence were not included, potentially limiting the comprehensive understanding of programme impact. Despite these limitations, the study contributes valuable insights into the effectiveness of cardiac and pulmonary rehabilitation programmes in improving mental well‐being and physical function among participants in regional and rural settings. The significant improvements observed in most of the measured outcomes, especially waist circumference, after attending just one session per week for only 6 weeks underscore the importance of such programmes, particularly in rural settings with limited options. Future research with larger sample sizes, control groups, longer follow‐up periods and comprehensive outcome measures is needed to further confirm the benefits of these programmes and address the identified limitations. Additionally, future studies may look at assessing the balance of the participants, particularly since the majority were older individuals; their lived experiences and barriers to attending cardiorespiratory rehabilitation may provide further insights.
Clinical Implications
4.2
From a clinical perspective, attending even one session per week of cardiac or pulmonary rehabilitation can yield positive outcomes for participants, particularly in settings where resources are scarce. Healthcare providers, especially those working in regional and rural areas, should consider incorporating and promoting rehabilitation programmes as part of comprehensive care plans for patients with cardiac and respiratory diseases. Furthermore, the findings underscore the need for funding for ongoing support and intervention beyond the immediate post‐rehabilitation period to sustain the observed improvements in mental well‐being and physical function. Overall, this contributes to the growing body of evidence supporting the benefits of cardiac and pulmonary rehabilitation programmes in improving health outcomes for individuals living with cardiovascular and respiratory conditions. Future research with larger sample sizes and longer follow‐up periods is warranted to better understand the long‐term effects of these programmes. By addressing these gaps in knowledge, healthcare providers can better tailor rehabilitation interventions to meet the needs of patients in regional and rural settings, ultimately improving overall health and well‐being.
Conclusion
5
The findings of this study underscore the important role of cardiac and pulmonary rehabilitation programmes, particularly in addressing the healthcare disparities prevalent in rural and regional areas characterised by limited‐service access. Our findings highlight the significant impact of even short‐term participation in these programmes on enhancing both the mental well‐being and physical function of the participants. Notably, the observed improvements in key measures, including the reduction in the proportion of participants experiencing major depression, enhanced mobility as evidenced by decreased time to complete the 5‐STS, increased 6MWT distance and reduction in waist circumference, underscore the importance of implementing and advocating for the expansion of such rehabilitation initiatives in underserved regions. This is particularly crucial as rural and regional communities grapple with persistent healthcare resource shortages; therefore, securing funding for sustainable programmes led by allied health professionals becomes imperative. Programmes such as this do not only address immediate healthcare needs of people in their community but lay the foundation for positive long‐term health and general well‐being outcomes, thereby mitigating the impact of service deficiencies on vulnerable populations. Investing in and prioritising the dissemination of rehabilitation services in these areas becomes essential steps towards fostering equitable access to quality healthcare for all.
Author Contributions
Nnamdi Mgbemena: conceptualization, writing – review and editing, writing – original draft, formal analysis, methodology. Jane Thompson: conceptualization, writing – original draft, writing – review and editing, investigation, resources, methodology. Uchechukwu Levi Osuagwu: conceptualization, methodology, writing – review and editing, writing – original draft, formal analysis.
Disclosure
The authors have nothing to report.
Ethics Statement
The study followed the tenets of the Declaration of Helsinki for human subjects (as revised in Brazil 2013). Prior to data collection, ethics approval for the study was obtained from Western New South Wales Local Health District; Greater Western Human Research Ethics Committee, University Research Ethics Committee (2021/ETH00556).
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Appendix S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. D. Hasnain , D. Patrick , and S. T. Rod , “Cardiac rehabilitation,” BMJ [British Medical Journal] 351 (2015): h 5000.26419744
- 2J. A. Alison , Z. J. Mc Keough , K. Johnston , et al., “Australian and New Zealand Pulmonary Rehabilitation Guidelines,” Respirology 22, no. 4 (2017): 800–819, 10.1111/resp.13025.28339144 · doi ↗ · pubmed ↗
- 3Lung Foundation Australia , “Pulmonary Rehabilitation Toolkit 2023,” accessed March 25, 2024, https://lungfoundation.com.au/health‐professionals/clinical‐information/pulmonary‐rehabilitation/pr‐toolkit/.
- 4Heart Foundation , “Cardiac Rehabilitation. Supporting Your Recovery 2020,” accessed March 25, 2024, https://assets.contentstack.io/v 3/assets/blt 8a 393bb 3b 76c 0ede/blta 676a 981e 19696 d 6/659cb 867bb 2e 10cf 2c 012952/Cardiac‐Rehab_Brochure_2020.pdf.
- 5R. S. Taylor , H. M. Dalal , and S. T. J. Mc Donagh , “The Role of Cardiac Rehabilitation in Improving Cardiovascular Outcomes,” Nature Reviews Cardiology 19, no. 3 (2022): 180–194.34531576 10.1038/s 41569-021-00611-7PMC 8445013 · doi ↗ · pubmed ↗
- 6Australian Institute of Health and Welfare , “Treatment Pathways for People Hospitalised for Acute Coronary Syndrome, Australia,” 2024, accessed March 27, 2024, https://www.aihw.gov.au/reports/heart‐stroke‐vascular‐diseases/treatment‐pathways‐for‐people‐hospitalised‐for‐acu/contents/background.
- 7Heart Foundation , “Acute Coronary Syndromes (ACS) Clinical Guidelines,” 2024 accessed January 21, 2025, https://www.heartfoundation.org.au/for‐professionals/fp‐acs‐guidelines.
- 8S. Sritharan , B. Wilsmore , J. Wiggers , et al., “Rural‐Urban Differences in Outcomes of Acute Cardiac Admissions in a Large Health Service,” JACC: Advances 3, no. 11 (2024): 101328, 10.1016/j.jacadv.2024.101328.39469611 PMC 11513678 · doi ↗ · pubmed ↗