Rare Causes of Abdominal Pain
Wei Zheng, Xiaoyan Yu, Suying Wu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
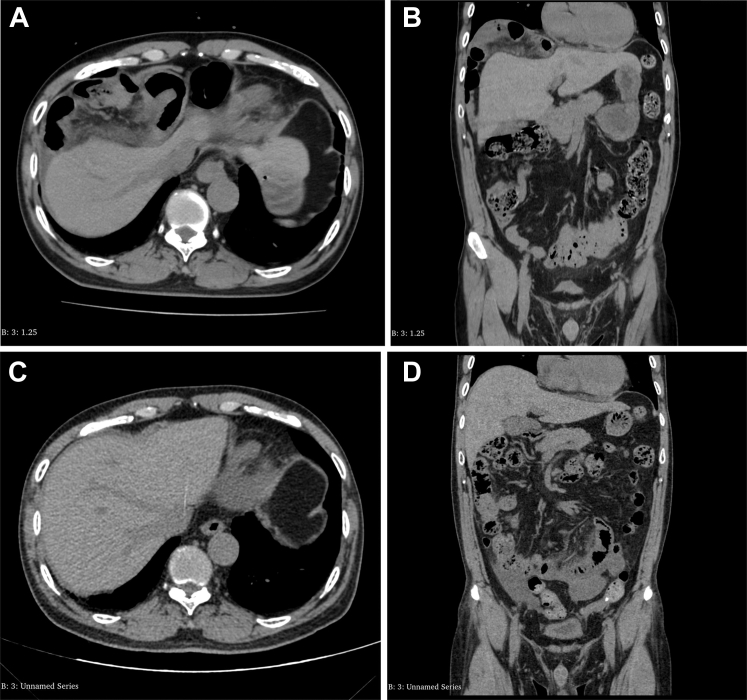 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions
Case Presentation
1
A 61-year-old man presented with a 6-hour history of persistent dull pain in the right upper abdomen, gradually worsening over time, accompanied by nausea and vomiting of gastric contents. The pain did not radiate, was unrelated to position changes, and had no associated fever, chills, abdominal distension, diarrhea, or bowel obstruction. Physical examination revealed mild right upper abdominal tenderness without rebound tenderness, with normal bowel sounds. Laboratory tests were unremarkable, and an abdominal computed tomography scan was performed for further evaluation with results shown in Figure A and B. What is the cause of the abdominal pain and the patient’s diagnosis?FigureA, Axial view of the patient’s abdomen on computed tomography (CT) imaging. B, Coronal view of the patient’s abdomen on CT imaging. C, Axial view of the patient’s abdomen on CT imaging. D, Coronal view of the patient’s abdomen on CT imaging.
Diagnosis: Chilaiditi Syndrome
2
After conservative treatment during hospitalization, the patient’s symptoms improved, and follow-up computed tomography scans are shown in Figure C and D. Chilaiditi sign describes the positioning of the colon between the liver and diaphragm on imaging and is typically asymptomatic. When symptomatic, it is termed Chilaiditi syndrome.1 This syndrome was first reported in 1910 by Greek radiologist Demetrius Chilaiditi.2 The incidence of Chilaiditi syndrome is approximately 0.025% to 0.28%,3 with a higher prevalence in elderly men. The exact etiology of Chilaiditi syndrome remains unclear.4 Research by Inagaki and Ebata1 indicates that the interposed organ is most commonly the colon (93.1%), with the small intestine accounting for approximately (6%) of cases, with small bowel interposition being more likely to cause an acute abdomen. Most cases are asymptomatic. Symptomatic patients may need rest, fluids, decompression, or surgery for obstructions or ischemia.5
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Inagaki S.Ebata K.A roentgenological study of Chilaiditi’s syndrome Article in Japanese Nihon Ika Daigaku Zasshi 5941992302322140090510.1272/jnms 1923.59.302 · doi ↗ · pubmed ↗
- 2Chilaiditi D.Zur frage der hepatoptose und ptose im allgemeinen im anschlussan drei fälle von temporärer, partieller leberver-lagerung Fortschr Geb Röntgenstr Nuklearmed 161910173208
- 3Moaven O.Hodin R.A.Chilaiditi syndrome: a rare entity with important differential diagnoses Gastroenterol Hepatol (N Y)84201227627822723763 PMC 3380266 · pubmed ↗
- 4Nakagawa H.Toda N.Taniguchi M.Ibukuro K.Tagawa K.Prevalence and sonographic detection of Chilaiditi's sign in cirrhotic patients without ascites AJR Am J Roentgenol 18762006 W 589W 5931711451010.2214/AJR.05.0597 · doi ↗ · pubmed ↗
- 5Torgersen J.Suprahepatic interposition of the colon and volvulus of the cecum Am J Roentgenol Radium Ther 665195174775114878056 · pubmed ↗