Severity of Hirsutism and Its Correlation With Hyperandrogenism: A Cross-Sectional Study in Erbil City
Dindar S Qurtas, Jwan H Ezzat

TL;DR
This study in Erbil City found that most hirsute women had mild hirsutism and no significant testosterone differences, but higher 17-hydroxyprogesterone levels were observed.
Contribution
The study provides local data on hirsutism severity and its hormonal correlations in a specific population.
Findings
98% of hirsute cases had mild or moderate hirsutism, with only 2% having severe hirsutism.
No significant differences in serum testosterone levels were found between hirsute and non-hirsute groups.
Higher mean serum 17-hydroxyprogesterone levels were observed in hirsute females.
Abstract
Background: Hirsutism is defined as excessive terminal hair growth in females in androgen-dependent areas. Hyperandrogenism is a hormonal disease that clinically often presents as hirsutismus. Hirsutism is associated with high levels of androgens according to a few studies. This study is conducted to analyze this correlation in female individuals in Erbil City, Kurdistan Region, Iraq. Methods: This case-control study included 100 hirsute females and their 100 non-hirsute counterparts. A thorough history was obtained for symptoms and conditions associated with hyperandrogenism. The severity of hirsutism was assessed with the modified Ferriman-Gallwey (mFG) score. Laboratory tests were performed to include thyroid function and androgen hormone levels. Results: Most hirsute cases (98%) had mild and moderate hirsutism, and only 2% had severe hirsutism. Thyroid function tests were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
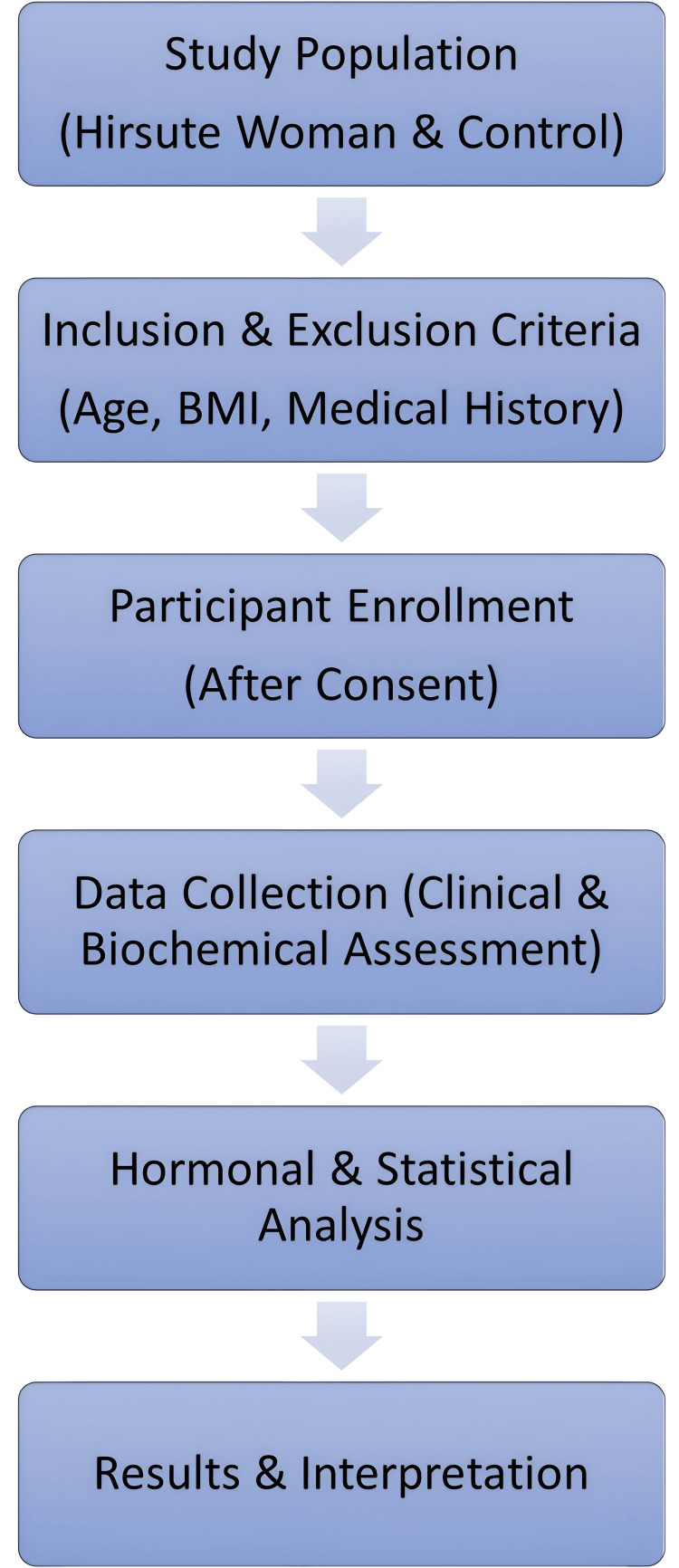 Figure 1
Figure 1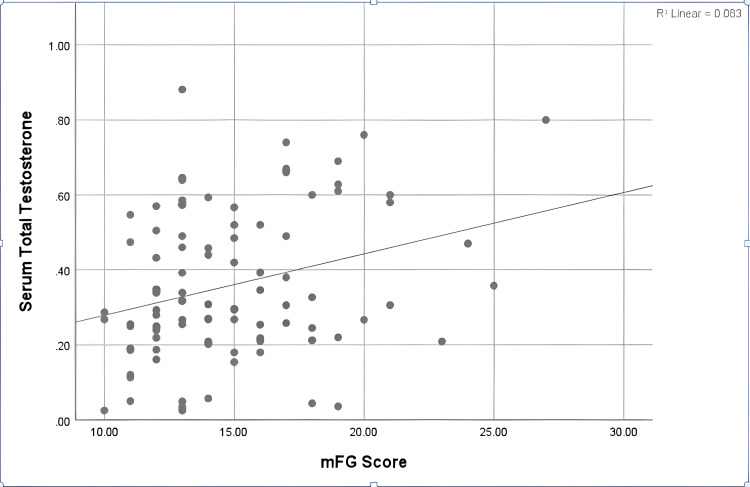 Figure 2
Figure 2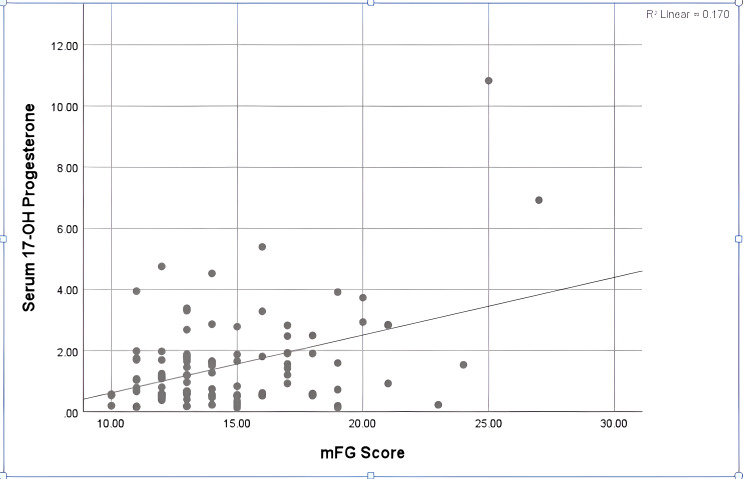 Figure 3
Figure 3| Characteristic | Index | Hirsute cases (n=100) | Controls (n=100) | p-Value* |
| Age (years) | 28.8±7.54 | 27.2±4.9 | 0.25 | |
| Marital Status | Single | 55 | 100 | <0.001 |
| Married | 45 | 0 | ||
| Occupation | Student | 17 | 41 | 0.003 |
| Housewife | 61 | 54 | ||
| Public Employee | 11 | 0 | ||
| Self-employed | 11 | 5 | ||
| Age of Menarche (years) | 12.44±0.87 | 12.32±0.76 | 0.43 | |
| Regularity of Period | Regular | 75 | 92 | 0.013 |
| Irregular | 25 | 8 | ||
| Premenstrual Syndrome | 29 | 31 | 0.8 | |
| Menstrual Character | Normal | 74 | 90 | 0.14 |
| Oligomenorrhea | 24 | 10 | ||
| Polymenorrhea | 1 | 0 | ||
| Menorrhagia | 1 | 0 | ||
| Parity | Nulliparous | 56 | 98 | <0.001 |
| Multiparous | 44 | 2 | ||
| History of Induction of Ovulation | 10 | 2 | 0.076 | |
| Presence of Acne | 83 | 40 | 0.004 | |
| Presence of Hair Fall | 55 | 10 | 0.001 | |
| Presence of Acanthosis Nigricans | 13 | 2 | 0.059 | |
| Family History of Hirsutism | 62 | 10 | 0.001 | |
| Family History of PCOS | 30 | 4 | 0.001 | |
| Drug History | Anti-HTN | 1 | 0 | 0.46 |
| Tonics | 3 | 0 | ||
| Herbals | 3 | 0 | ||
| Weight (kg) | 70.76±9.65 | 63.24±7.39 | 0.001 | |
| Height (cm) | 159.7±4.58 | 159.14±2.78 | 0.42 | |
| BMI (kg/m2) | 27.73±3.92 | 24.94±2.56 | 0.001 | |
| BMI Categories | Normal | 27 | 65 | 0.003 |
| Overweight | 49 | 26 | ||
| Obese | 21 | 9 | ||
| Morbid Obese | 3 | 0 | ||
| Modified Ferriman-Gallwey Score | 14.82±3.43 | 5.8±1.06 | <0.001 | |
| Hirsutism Severity | Normal (0-7) | 0 | 100 | <0.001 |
| Mild (8-16) | 72 | 0 | ||
| Moderate (17-24) | 26 | 0 | ||
| Severe (≥25) | 2 | 0 |
| Site | Cases (Mean±SD) (n=100) | Controls (Mean±SD) (n=100) | p-Value* |
| Upper Lip | 2.66±0.68 | 2.41±0.62 | 0.12 |
| Chin | 2.32±0.76 | 0.36±0.59 | <0.001 |
| Chest | 1.52±0.59 | 0.02±0.14 | <0.001 |
| Upper Abdomen | 1.42±0.61 | 0.26±0.44 | <0.001 |
| Lower Abdomen | 1.81±0.89 | 1.12±0.36 | <0.001 |
| Upper Arm | 1.35±0.61 | 0.13±0.31 | <0.001 |
| Thighs | 1.48±0.58 | 0.92±0.35 | <0.001 |
| Upper Back | 1.01±0.11 | 0.02±0.14 | <0.001 |
| Lower Back | 1.25±0.46 | 0.64±0.48 | <0.001 |
| Total (mFG Score) | 14.82±3.43 | 5.8±1.06 | <0.001 |
| Laboratory Test (Unit) | Reference Range | Cases (n=100) | Controls (n=100) | p-Value* |
| Serum TSH (µIU/mL) | 0.27-4.2 | 2.52±1.4 | 2.63±0.97 | 0.64 |
| Serum Free T3 (pmol/L) | 3.1-6.8 | 5.37±0.82 | 5.06±0.93 | 0.32 |
| Serum Free T4 (pmol/L) | 12-22 | 14.41±2.0 | 15.16±2.08 | 0.25 |
| Serum Total Testosterone (ng/mL) | 0.06-0.82 | 0.38±0.25 | 0.32±0.26 | 0.13 |
| Serum Free Testosterone (pg/mL) | 0.4-7.1 | 4.18±2.26 | 2.41±1.21 | 0.07 |
| Serum 17-OH Progesterone (ng/mL) | 0.2-1.3 | 1.53±1.57 | 0.76±0.46 | 0.03 |
| Variable | Hirsutism Severity (n=100) | p-Value* | |||
| Mild (n=72) | Moderate (n=26) | Severe (n=2) | |||
| Period Regularity | Regular | 60 | 15 | 0 | 0.001 |
| Irregular | 12 | 11 | 2 | ||
| Menstrual Character | Normal | 61 | 13 | 0 | 0.001 |
| Oligomenorrhea | 11 | 11 | 2 | ||
| Polymenorrhea | 0 | 1 | 0 | ||
| Menorrhagia | 0 | 1 | 0 | ||
| Perimenstrual Syndrome (kg/m2) | 17 | 10 | 2 | 0.02 | |
| BMI | Normal | 18 | 8 | 1 | 0.04 |
| Overweight | 41 | 8 | 0 | ||
| Obese | 13 | 7 | 1 | ||
| Morbid Obese | 0 | 3 | 0 | ||
| Hirsutism Severity | mFG Score | Total Testosterone (ng/mL) | Free Testosterone (pg/mL) | p-Value* | ||||||
| Normal (0.06-0.82) | High (≥0.82) | Normal (0.4-7.1) | High (≥7.1) | |||||||
| Frequency | Mean Value | Frequency | Mean Value | Frequency | Mean Value | Frequency | Mean Value | |||
| Controls | ≤7 | 99 | 0.32 | 1 | 0.8 | 98 | 2.78 | 2 | 7.5 | 0.006 |
| Mild | 8-16 | 71 | 0.33 | 1 | 0.85 | 71 | 1.98 | 1 | 7.8 | |
| Moderate | 17-24 | 26 | 0.43 | 0 | NA | 26 | 2.2 | 0 | NA | |
| Severe | ≥25 | 1 | 0.36 | 1 | 0.8 | 2 | 4.1 | 0 | NA | |
| Hirsutism Severity | mFG Score | Serum 17-OH Progesterone (ng/mL) | p-Value* | |||||
| Normal (0.2-1.3) | Mildly Elevated (1.4-10) | High (>10) | ||||||
| Frequency | Mean Value | Frequency | Mean Value | Frequency | Mean Value | |||
| Controls | ≤7 | 96 | 0.7 | 4 | 2.2 | 0 | NA | 0.03 |
| Mild | 8-16 | 62 | 0.8 | 10 | 3.9 | 0 | NA | |
| Moderate | 17-24 | 18 | 1.2 | 8 | 3.2 | 0 | NA | |
| Severe | ≥25 | 0 | NA | 1 | 7.1 | 1 | 11.2 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Sexual Differentiation and Disorders · Hair Growth and Disorders
Introduction
Hirsutism is defined as excessive terminal hair growth in women within androgen-dependent areas. It is a reflection of either an increase in circulating androgens or a heightened end-organ response to them. Increased production of androgens could be from the ovaries or adrenal glands, or occasionally from androgen-secreting tumors [1].
Hirsutism is diagnosed clinically by using a special visual scale called the modified Ferriman-Gallwey (mFG) score, where a total of ≥8 points is indicative of hirsutism. The mFG score assesses the density of terminal hair at nine distinct body regions, including the upper lip, chin, upper back, lower back, upper abdomen, arms, and thighs [2].
Hyperandrogenism may manifest clinically or biochemically. Clinical hyperandrogenism is defined as the presence of symptoms such as hirsutism, acne, and androgenic alopecia. Biochemical hyperandrogenism is defined as an elevated serum level of androgens, including total testosterone (TT), free testosterone (FT), androstenedione, dehydroepiandrosterone (DHEA), and the DHEA metabolite dehydroepiandrosterone sulfate (DHEAS) [3].
Although a proportion of hirsute women have elevated levels of circulating androgen, others do not. It has been established that there is a weak correlation between the degree of androgen excess and the manifested severity of hirsutism. Furthermore, it is still unclear which androgenic factor has the strongest influence on the mFG score [4]. Peripheral androgen metabolism also appears to influence the exhibition of hyperandrogenism [5].
Although hyperandrogenism has been a subject of much research, little has been studied about it regarding the Middle Eastern population, especially the population of Erbil, Kurdistan. Hirsutism is a multifactorial condition with genetic, environmental, and lifestyle factors influencing its presentation and severity, yet epidemiological information on the prevalence of hirsutism in this region is limited. There is a lack of some of this information that is necessary for achieving more accurate diagnosis and treatment specifically in this population [6]
The aim of this study is to evaluate the correlation of hirsutism severity with androgen hormone levels and clinical features of hyperandrogenism in hirsute women compared to healthy controls in Erbil, Kurdistan.
Materials and methods
Study design and setting
This case-control study was performed in the Erbil Dermatology Teaching Center, Kurdistan Region, Iraq. The study was designed to evaluate the association between severity of hirsutism and biochemical markers of hyperandrogenism in women with and without hirsutism.
Study population and sampling method
A case-control study was performed on 100 consecutive hirsute women (cases) who were seen at the outpatient dermatology clinic with healthy female controls who did not have hirsutism. Controls were age-matched (±2 years) and BMI-matched (±2 kg/m^2^) to minimize potential confounding effects.
Inclusion and exclusion criteria
Cases were defined as females with mFG score ≥8. Pregnant or lactating women, women with premenarchal, postmenopausal, hormonal therapy, or hysterectomy history or diagnosed as having primary ovarian failure, as well as women who applied laser hair removal recently within the previous six months were excluded from the study. Controls were selected in the same clinic, mFG score <8, and with no androgen-related disorders history.
Data collection and assessments
Hirsutism was assessed using the mFG score in nine androgen-dependent sites (upper lip, chin, chest, upper back, lower back, upper abdomen, lower abdomen, thighs, and upper arms). In each of these areas, a score of 0 (absence of terminal hairs) through 4 (extensive terminal hair growth) was assigned [7]. Hirsutism severity was measured according to Abraham's classification as mild 8-16, moderate 17-24, and severe 24-36 [8].
Demographic and clinical data, including age, marital status, occupation, and family history of hirsutism or polycystic ovarian syndrome, were recorded after obtaining written informed consent. Gynecological and obstetric history (age menarche commenced, menstrual regularity, ovulation induction history, and in vitro fertilization (IVF) history) was documented. Dermatological manifestations, including acne, alopecia, and acanthosis nigricans, were noted. The medication history was documented, including glucocorticoids, supplements, and gym enhancers. We calculated body mass index (BMI) using the equation weight (kg)/height (m^2^).
Hormonal and biochemical assessment
Venous blood samples were obtained during the early follicular phase of the menstrual cycle. We measured serum TT, FT, and 17-OH progesterone using enzyme-linked immunosorbent assay (ELISA) kits. Thyroid-stimulating hormone (TSH), free triiodothyronine (T3), and free thyroxine (T4) levels were measured by a fully automated chemiluminescence immunoassay (Cobas e411 analyzer, Roche Diagnostics, Rotkreuz, Switzerland). All assays were validated and quality controlled internally, and calibrated using international standards.
Statistical analysis
Data were analyzed with SPSS 25.0 (IBM Corp., Armonk, NY). Continuous variables were presented as mean ± standard deviation (SD) and categorical variables were presented as frequency and percentage. Student’s t-tests were performed for the comparison of continuous variables between groups, and chi-squared or Fisher’s exact tests were used for categorical data. For three or more subgroups, a one-way analysis of variance (ANOVA) was used for comparisons. Based on data normality, Pearson’s or Spearman’s correlation coefficients were calculated. Multiple imputation techniques were used to handle missing data where appropriate. A p-value <0.05 was considered statistically significant.
Ethical considerations
Ethics approval was granted from the Kurdistan Higher Council for Medical Specialties (KHCMS) (Letter No. 14/241-2023). Informed written consent was achieved from all responders before explaining the objectives and procedures of the study. Data were treated confidentially, and participants were informed that they could withdraw at any time.
Data visualization and supplementary information
Participants were screened for eligibility based on selection criteria. Informed consent was then obtained to recruit eligible participants, including hirsute women and healthy controls. Data collection involved a clinical assessment using the mFG score, biochemical analysis of androgen levels, and documentation of demographic and medical history. Data analysis was performed using SPSS 25.0 to statistically evaluate the correlation between hirsutism severity, clinical signs, and biochemical markers. The results highlight the associations between hirsutism severity and hyperandrogenism parameters (Figure 1).
Study flowchart: selection criteria, data collection, and analysis frameworkScreening: Determining if participants fit in or out of involvement by selection criteria.Materials and methods enrollment: Informed consent was obtained to recruit eligible participants (hirsute women and healthy controls).Data collection: Clinical assessment using modified Ferriman-Gallwey (mFG) score, biochemical analysis of androgen levels, and demographic and medical history were documented.Data analysis using SPSS 25.0 for statistical evaluation of the correlation between hirsutism severity, clinical signs, and biochemical markers.Outcome: Associations between hirsutism severity and hyperandrogenism parameters are interpreted.
Results
In this research, the average age of hirsute cases was 28.8±7.54 years compared to 27.2±4.9 years in controls (p=0.25). Furthermore, the two groups had similar ages of menarche (p=0.43). Hirsute ladies were more likely to be overweight (p=0.001), experience more menstrual irregularity (p=0.013), acne (p=0.004), and hair fall (p=0.001), and give a significant family history of polycystic ovary syndrome (PCOS) and hirsutism (p=0.001). The average mFG score in hirsute cases was 14.82±3.43 compared to 5.8±1.06 in controls (p=0.001). Only a few cases reported using medication with no apparent significant effect on mFG score (p=0.46) (Table 1).
Table 1: Clinical characteristics of hirsute cases and controls*p-Value <0.05 is considered to be significant.HTN, hypertension.
The distribution of terminal growth over the nine predefined androgenic areas of the body according to the mFG score is shown in Table 2. Compared to controls, the only site where terminal hair growth density did not differ in hirsute and non-hirsute was the upper lip region (p=0.12) (Table 2).
*Table 2: mFG scores on androgen-sensitive areas of the bodyThere were significant differences in every area but the upper lip.mFG, modified Ferriman-Gallwey.p-Value <0.05 is considered to be significant.
On hormonal evaluation of cases and controls, no significant differences were observed in mean serum levels of thyroid function status between them (p=0.4). On individual analysis of the subjects, only four hirsute cases (4%) had subclinical hypothyroidism. In general, there was a minimal discrepancy between serum TT and FT between the two groups. There was a mild elevation of mean serum levels of 17-OH progesterone more than normal, versus normal value among the control subjects (p=0.03) (Table 3).
Table 3: Hormonal assessment of hirsute cases and controls*p-Value <0.05 is considered to be significant.
According to the mFG score of the hirsute cases, the severity was mild in 72 (72%) cases, moderate in 26 (26%) cases, and severe in two (2%) cases. The degree of severity of hirsutism was significantly different in terms of regularity of periods (p=0.001), menstruation character (p=0.001), premenstrual syndrome (p=0.02), and body weight (p=0.04). However, the association was statistically significant in more than half of them, resented by 60 (60%) cases of hirsute cases having regular menstrual periods; on the other hand, only two cases (2%) had irregular periods in severe hirsutism. Regarding the amount of menstrual bleeding, the majority, 74% (74 cases), had the normal amount of bleeding, and oligomenorrhea was observed in 24% (24 cases) of hirsute cases. Normal BMI was observed in only 27 hirsute cases (27%), and the rest had increased BMI (Table 4).
Table 4: Correlation of severity of hirsutism with menstruation and body mass*p-Value <0.05 is considered to be significant.
Although the measured values of serum TT were within the normal range in the majority of cases (98%), only two cases (2%) had significant elevations in the serum TT, out of which only one case (1%) suffered from severe hirsutism. Only one case of hirsute females had high serum FT (Table 5). Despite these data, there was a trend toward higher mFG scores within the normal range of TT (p=0.006) (Figure 2).
Table 5: Mean serum testosterone levels according to hirsutism severity*p-Value <0.05 is considered to be significant.mFG, modified Ferriman-Gallwey.
Correlation between mFG score and total serum testosterone in hirsute casesSerum total testosterone is measured in ng/mL.mFG, modified Ferriman-Gallwey.
A significant correlation was found between hirsutism severity and serum 17-OH progesterone level (p=0.03). About 19 (19%) hirsute cases had mildly elevated serum 17-OH progesterone levels, while only one case (1%) was found to have severe hirsutism together with high 17-OH progesterone (Table 6). The scatter plot shows the correlation between serum 17-OH progesterone and mFG score. There was a strong correlation (p=0.03) (Figure 3).
Table 6: Comparison of serum 17-OH progesterone levels in cases and controls*p-Value <0.05 is considered to be significant.mFG, modified Ferriman-Gallwey.
Correlation between mFG score and serum 17-OH progesterone in hirsute casesSerum 17-OH progesterone is measured in ng/mL.mFG, modified Ferriman-Gallwey.
Discussion
Hirsutism is a genetically influenced condition and is characterized by excessive terminal hair growth in androgen-dependent areas, caused by a combination of genetic, hormonal, and environmental factors [1]. Etiologies include either an increase in circulating androgens or a heightened end-organ response to them. Increased production of androgens could be from the ovaries or adrenal glands, or occasionally from androgen-secreting tumors [2]. Hyperandrogenism manifests clinically as hirsutism, androgenic alopecia, and acne [8]. The prevalence of hirsutism is around 30% in premenopausal Iraqi women [9]. Evaluation of hirsutism can be made using the standard mFG score [6]. A common cutoff value of ≥8 is used if no population-specific studies recommend a different limit [6,7]. Significant variations in age, skin type, and race/ethnicity also play a role in redefining hirsutism in a given population [10,11]. Patients with endocrine organ-based dysfunction-related hirsutism are more likely to manifest an mFG score ≥15, while a normal or slightly elevated circulating levels of androgens may be detected in constitutional (dermatologic) hirsutism [12]. Regarding androgens, the circulating free, rather than TT, seems to exert a significant role in the transformation of vellus to terminal hair during puberty in the androgen-dependent areas of the female body [13]. BMI ≥30 is often seen in association with hirsutism because of increased conversion of androgen precursors to testosterone [14,15]. Measurement of 17-OH progesterone in hirsute women may be valuable in uncovering cases of late-onset congenital adrenal hyperplasia (CAH) [16]. Although uncommon, the incidence of CAH is around 1.9-3% in Mediterranean populations [17]. In this study, we investigated the correlation between the clinical signs and biochemical values of hyperandrogenism in hirsute women and non-hirsute controls in Erbil City, Kurdistan Region, Iraq. A statistically significant correlation was demonstrated between the severity of hirsutism according to mFG score and serum FT rather than TT, serum 17-OH progesterone, and other clinical features of hyperandrogenism. Despite the former mentioned association, while almost all (98%) hirsute cases had no elevation of their hormone levels in androgens, as mentioned in the other studies, values of mFG were more than 7, i.e. hirsutism have 7 times more elevated levels of serum FT [18]. Family history of hirsutism and PCOS among hirsute was observed to be significantly more than the non-hirsute. The majority of hirsute ladies in this study also exhibited other signs of hyperandrogenism like acne in 83% of cases and hair fall in 55% of cases which were much higher than non-hirsute subjects. These data regarding acne-associated hirsutism are slightly higher than those of a report published before [19]. In this study, no correlation between thyroid dysfunction and hirsutism was seen and the same observation was found among non-hirsute cases; however, in some other studies, some percentage (16-17%) of hirsute cases of PCOS had thyroid dysfunction [20,21]. Recent studies demonstrated various findings. In a study conducted on hirsute women in Basrah city, FT, rather than TT or DHEAS, was found to correlate with the severity of hirsutism [22]. In Filipino women, FT was likely to be elevated if the mFG score was >7. In 80 Iraqi women with PCOS, higher levels of testosterone were recorded compared to healthy controls, with the magnitude of elevation of serum testosterone being proportionate to the severity of manifested hirsutism [23]. Conversely, a study in Kalar did not show these findings, and no correlation to any hormonal disturbance could be demonstrated in the study group [24]. In a study evaluating serum FT in hirsute PCOS women in Soran City, the highest levels were recorded in the youngest age group (18-20-year-olds) [25]. In Kirkuk City, a study of 1000 young lean female students with no underlying ovarian dysfunction or menstrual irregularity, i.e., non-PCOS etiology of hirsutism, has shown a significant correlation between hirsutism severity and serum FT, DHEAS, androstenedione, and sex hormone-binding globulin (SHBG). A strong family history was also uncovered in a significant proportion of cases [26]. It is recommended that the approach to the management of hirsutism should be based on a thorough and detailed history and physical examination of the affected women [27,28]. The higher quartiles of mFG scores are generally expected to be related to significant pathology [29,30]. Thus, according to the results of our study, especially in resource-limited health systems, over-investigating the cause of apparently mild-moderate hirsutism with costly hormonal assays may not be necessary, and can be avoided with careful selection of diagnostic testing according to the clinical probability determined by the dermatologist and/or endocrinologist.
An important shortcoming of our study is the low number of severe hirsutism cases, which limits statistical power and generalizability. Further investigation will require a large sample with more severe cases. Moreover, the cross-sectional design of the study does not allow conclusions on a cause-effect basis; longitudinal studies measuring hormonal changes over time could clarify the natural evolution of hirsutism.
Another significant limitation was the lack of DHEAS measurement which would have given additional information about the adrenal contribution to hyperandrogenism. To enhance diagnostic accuracy, future studies should incorporate a broader hormonal panel, potentially including androstenedione and SHBG [26,30]. Moreover, the investigation of potential metabolic confounders, including insulin resistance and obesity-related hyperinsulinemia, may give a better understanding of the pathophysiology of hirsutism.
Recommendations for clinicians in practice
In approaching hirsutism, clinicians should utilize a stepwise diagnostic method, starting with detailed history-taking and physical examination, reserving extensive biochemical testing for patients with specific features on history and physical examination [27,28]. This approach should be tailored to the patient due to the frequency of mild to moderate hirsutism with normal androgen levels based on family history, BMI, and metabolic risk. Where there is severe or progressive hirsutism, specific endocrine evaluation including 17-OH progesterone and DHEAS should be the main focus.
Conclusions
This adds to the body of literature documenting regional patterns of hirsutism/hyperandrogenism, particularly from the Middle Eastern population. Our results underscore FT and 17-OH progesterone being relevant biochemical markers for hirsutism evaluation results in a more clinically relevant, economical, and lower-cost approach. Although the small number of severe cases limits the generalizability of findings, the study highlights the need for context-specific diagnostic strategies and further research to improve clinical guidance. Future studies should seek to validate these findings across larger cohorts, integrate more biochemical markers, and continue to elucidate the genetic and metabolic basis of hirsutism in various populations. By taking into account these aspects, the performance in diagnosing and treating hirsutism could be bettered, and health outcomes improved.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Approach to androgen excess in women: Clinical and biochemical insights Clin Endocrinol (Oxf) Cussen L Mc Donnell T Bennett G Thompson CJ Sherlock M O'Reilly MW 1741869720223534917310.1111/cen.14710 PMC 9541126 · doi ↗ · pubmed ↗
- 2Practise updates: Diagnosis and management of idiopathic hirsutism Indian J Endocrinol Metab Khare VR Sinha B Sengupta N 2392492820243908656410.4103/ijem.ijem_2_24PMC 11288517 · doi ↗ · pubmed ↗
- 3Androgen excess and deficiency: Analytical and diagnostic approaches Clin Chem Heijboer AC Hannema SE 136113736920233779465110.1093/clinchem/hvad 146 · doi ↗ · pubmed ↗
- 4Testosterone or dihydrotestosterone: What should be evaluated in hirsutism?Ir J Med Sci Darjani A Alizadeh N Gharaei Nejad K Eftekhari H Rafiei R Kazemi H Rafiei E 2823282719220233704317110.1007/s 11845-023-03366-x · doi ↗ · pubmed ↗
- 5An update on the assessment and management of hirsutism Obstet Gynaecol Reprod Med Armata I Prakash A 8187342024
- 6Is there a difference in hirsutism score in adolescents with polycystic ovary syndrome on the basis of ethnicity and race?J Pediatr Adolesc Gynecol Badr F Chattha AJ 3483523720243815105810.1016/j.jpag.2023.12.008 · doi ↗ · pubmed ↗
- 7Clinical and biological assessment of hirsutism Hirsutism Mauvais-Jarvis P Kuttenn F Mowszowicz I Berlin, Heidelberg Springer 1981
- 8Practical approach to hyperandrogenism in women Med Clin North Am Sharma A Welt CK 1099111610520213468841710.1016/j.mcna.2021.06.008PMC 8548673 · doi ↗ · pubmed ↗