Internal Hernia Through a Mesoappendix Defect: A Case Report and Review of the Literature
Rafique Umer Harvitkar, Sugunesh Nanjan, Ioannis Hannadjas, Mariyam Shaheed, Alfredo Tonsi

TL;DR
A rare case of internal hernia through a mesoappendix defect causing small bowel obstruction is reported and reviewed.
Contribution
This case adds to the limited literature on mesoappendix defect-related internal hernias and their clinical presentation.
Findings
A 76-year-old woman presented with acute lower abdominal pain due to a mesoappendix defect causing small bowel obstruction.
Laparoscopy revealed a viable herniated ileum through the mesoappendix defect, successfully treated with reduction and appendicectomy.
The case emphasizes the importance of considering internal hernias in the differential diagnosis of SBO.
Abstract
Internal hernias are an uncommon cause of small bowel obstruction (SBO). If not identified and treated promptly, they can lead to severe complications. Among these, herniation through a mesoappendix defect is exceedingly rare. To our knowledge, SBO due to a mesoappendiceal defect has only been described in a limited number of cases. In this case, a 76-year-old woman presented to the emergency department with a two-day history of acute lower abdominal pain, accompanied by nausea, vomiting, and abdominal distension. Diagnostic imaging revealed a partial small bowel obstruction with two transition points. During diagnostic laparoscopy, a loop of proximal ileum was found herniating through a mesoappendix defect, resulting in a closed-loop obstruction. The herniated bowel was viable and was successfully reduced, followed by an appendicectomy. The postoperative recovery was uneventful. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
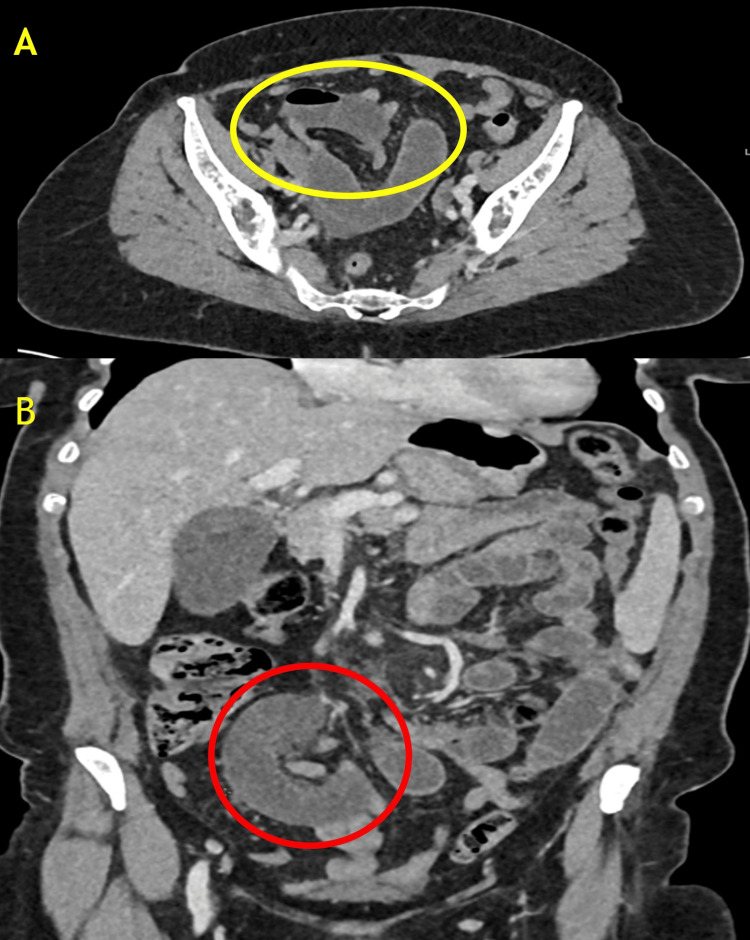 Figure 1
Figure 1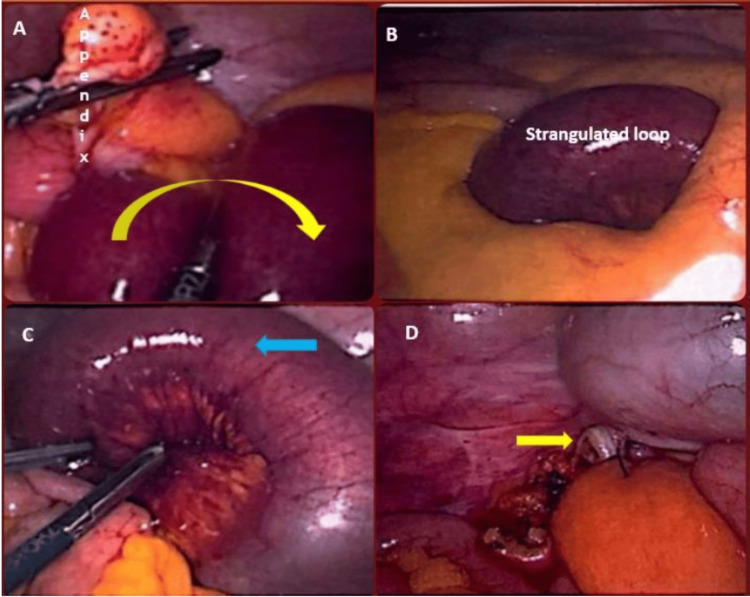 Figure 2
Figure 2| S. no. | Year of publication | Age | Sex | Author(s) | Patient manifestation | Contents | Treatment given |
| 1 | 1963 | 80 | M | Rooney et al. [ | Small bowel obstruction | Terminal Ileum | Reduction and closure |
| 2 | 2016 | 5 | M | Barman et al. [ | Small bowel obstruction | Meckel's diverticulum | Small bowel resection |
| 3 | 2020 | 55 | M | Vinay et al. [ | Small bowel obstruction | Terminal Ileum | Reduction and appendectomy |
| 4 | 2021 | 33 | F | Jones et al. [ | Appendicitis | Ovary (right) | Reduction and appendectomy |
| 5 | 2024 | 50 | M | Gashey et al. [ | Small bowel obstruction | Terminal Ileum | Reduction and appendectomy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Hernia repair and management · Intestinal Malrotation and Obstruction Disorders
Introduction
Internal hernias are a rare cause of small bowel obstruction (SBO), with an incidence of less than 1.5% in the general population. If untreated, they may result in a mortality rate of up to 48%. They account for approximately 0.6% to 6% of all SBO cases [1-4]. An internal hernia occurs when a viscus protrudes through a peritoneal or mesenteric aperture within the peritoneal cavity. These apertures can be congenital or acquired, with the latter often arising from surgical procedures, trauma, or inflammatory processes.
The mesoappendix, a peritoneal fold attaching the appendix to the ileum and caecum, is an uncommon site for internal herniation. Defects in the mesoappendix are rare and may be congenital or acquired [2]. When present, they can allow loops of the small intestine to herniate through, potentially causing bowel obstruction. To the best of our knowledge, only a few cases of SBO due to a mesoappendiceal defect have been reported. Given its rarity, this condition presents a diagnostic challenge and is often overlooked in the initial assessment of SBO.
Here, we report the case of a 76-year-old woman who presented with acute SBO secondary to an internal hernia through a mesoappendiceal defect. This case underscores the importance of considering internal hernias in patients presenting with bowel obstruction, even in those with a history of prior abdominal surgery.
Case presentation
A 76-year-old woman presented to the emergency department with a two-day history of acute onset lower abdominal pain. The pain was constant, severe, and predominantly located in the lower abdomen. She also reported associated symptoms of nausea, vomiting, and progressive abdominal distension. No previous episodes of similar symptoms were noted. Her medical history was significant for a laparoscopic hysterectomy performed several years prior. She had no history of bowel surgery, abdominal trauma, or known hernias. She was not on any regular medications and had no known allergies.
On clinical evaluation, the patient appeared in distress due to pain. Her vital signs were as follows: blood pressure of 135/80 mmHg, heart rate of 95 beats per minute, respiratory rate of 18 breaths per minute, and a temperature of 37.2°C. Abdominal examination revealed a distended abdomen with generalized tenderness, more pronounced in the lower quadrants; bowel sounds were absent. There were no palpable masses or signs of peritonitis. Laboratory investigations showed a lactate level of 3 mmol/L, a white blood cell count of 16 × 10⁹/L, a C-reactive protein (CRP) level of 65 mg/L, and serum creatinine indicating stage 1 acute kidney injury (AKI). Given her surgical history, an adhesional SBO was initially suspected.
The patient underwent a contrast-enhanced computed tomography scan of the abdomen and pelvis (CTAP), which revealed a partial SBO with dilated loops measuring up to 26 mm (Figures 1A, 1B). There was evidence of pelvic ascites and mesenteric vascular engorgement. Notably, two transition points were identified: one in the midline pelvis and another to the left of the midline. Importantly, abnormal enhancement of the small bowel was preserved, suggesting of ischemia. Given the imaging findings and the patient’s clinical presentation, a decision was made to proceed with diagnostic laparoscopy.
Contrast-enhanced CT images demonstrating small bowel closed-loop obstruction. (A) Axial section showing clustered, dilated small bowel loops with a characteristic "U-shaped" configuration, suggestive of a closed-loop obstruction (yellow circle). (B) Coronal section highlighting the transition point with mesenteric congestion and a radial distribution of mesenteric vessels converging towards the site of obstruction (red circle), consistent with internal herniation.
The patient was taken to the emergency operating theatre for a diagnostic laparoscopy within a few hours of admission. Intraoperatively, a loop of proximal ileum was found herniating through a defect in the mesoappendix, resulting in a closed-loop obstruction (Figures 2A, 2B). Although the herniated bowel initially appeared compromised in terms of blood supply, its appearance improved immediately upon reduction from the mesoappendix defect (Figure 2C). Therefore, bowel resection was not deemed necessary. Given the presence of a mildly inflamed appendix and to prevent future episodes, an appendicectomy was performed (Figure 2D). No other abnormalities or evidence of obstruction were noted during the procedure.
Intraoperative images: (A) an intraoperative view showing the appendix (labelled) with herniated small bowel loops entrapped along the mesoappendix (yellow curved arrow). (B) Strangulated small bowel loop visible after the initial reduction attempt, with signs of compromised vascularity. (C) Close-up of the reduced small bowel loop showing congestion and early ischemic changes (blue arrow) post-release of the obstruction. (D) Post-hernia reduction, the appendix is removed via laparoscopic appendicectomy (the yellow arrow indicates the appendiceal stump).
The patient tolerated the procedure well. Postoperatively, she was managed with intravenous fluids, analgesia, and prophylactic antibiotics. Her recovery was uneventful, with the return of normal bowel function and resolution of symptoms. She was discharged on the third postoperative day with advice for routine follow-up.
Discussion
Internal hernias are a rare but potentially life-threatening cause of SBO. They result from the protrusion of the small intestine through a normal or abnormal peritoneal or mesenteric defect, leading to varying degrees of obstruction. The incidence of internal hernias is estimated to be less than 1% in the general population, though they account for 0.6% to 6% of all SBO cases. The most common types of internal hernias include paraduodenal (52%), pericaecal (12%), transmesenteric and transmesocolic (7%), foramen of Winslow (7%), intersigmoid (5.5%), and retroanastomotic hernias (4.5%). However, herniation through a mesoappendix defect is extremely rare and scarcely reported in the literature [1-6].
The mesoappendix is a peritoneal fold containing the appendicular artery and veins, connecting the appendix to the ileum and caecum. Defects in the mesoappendix can be congenital or acquired. Congenital defects arise due to incomplete embryological development, whereas acquired defects may result from prior inflammation, ischemia, or trauma. These defects may create a potential space through which a segment of the small intestine can herniate, leading to obstruction and, if untreated, strangulation and ischemia [1-3,7-9].
In this case, a loop of proximal ileum was found traversing through a mesoappendix defect, forming a closed-loop obstruction. Closed-loop obstructions are particularly concerning because they increase intraluminal pressure, impair venous drainage, and can rapidly progress to bowel ischemia. The presence of mesenteric engorgement and ascites on imaging further suggested vascular compromise.
Internal hernias often present with non-specific symptoms, making preoperative diagnosis challenging. Patients typically report colicky abdominal pain, nausea, vomiting, and distension, as seen in this case. The absence of previous bowel surgery may lower the suspicion for adhesional obstruction, making imaging crucial [6,10-12]. CT imaging remains the gold standard for diagnosing internal hernias, with sensitivity exceeding 82%. Key radiological findings to look for include dilated small bowel loops with transition points, whirling of mesenteric vessels, presence of ascites or mesenteric vascular engorgement, and abnormal clustering of small bowel loops [2,13].
A review of the literature highlights similar cases of herniation through a mesoappendix defect. In most cases, the herniated content was the terminal ileum, with patients predominantly presenting with small bowel obstruction (Table 1).
The pathophysiology in these cases mirrors our findings, with congenital or acquired defects serving as the herniation site. Management consistently involves surgical intervention, with laparoscopy preferred due to its minimally invasive nature and diagnostic capabilities.
Conclusions
This case underscores the importance of considering internal hernias in the differential diagnosis of SBO, even in patients with prior abdominal surgeries. Internal hernias through a mesoappendix defect represent a rare but serious condition that requires prompt recognition and surgical management. CT and diagnostic laparoscopy are crucial to prevent complications such as bowel ischemia and necrosis, hence improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A rare case of small bowel obstruction due to paraduodenal hernia Am J Case Rep Al Otaibi RS Al Maghrabi HS Bin Dous Y Malaekah H 158115862020193165631010.12659/AJCR.918403 PMC 6839541 · doi ↗ · pubmed ↗
- 2Laparoscopic repair of internal hernias: a case series with review of literature Indian J Surg Harvitkar RU Joshi A 15341539832021
- 3Internal hernias due to defects in the meso-appendix and mesentery of small bowel, and probable Ivemark syndrome: report of two cases Ann Surg Rooney JA Carroll JP Keeley JL 25425815719631397469310.1097/00000658-196302000-00011 PMC 1466436 · doi ↗ · pubmed ↗
- 4Internal hernia: an increasingly common cause of small bowel obstruction Semin Ultrasound CT MR Blachar A Federle MP 1741832320021199623010.1016/s 0887-2171(02)90003-x · doi ↗ · pubmed ↗
- 5Internal herniation of Meckel’s diverticulum through mesoappendix in infant: an extremely rare occurrence Chrismed J Health Res Barman S Hadiuzzaman Md Ray S Sarkar R 899132016
- 6Broad ligament hernia: two contrasting ways to a common goal - two case reports with review of literature Int J Surg Case Rep Rohatgi Y Harvitkar RU Raut V Joshi A 1061988520213430408710.1016/j.ijscr.2021.106198 PMC 8327646 · doi ↗ · pubmed ↗
- 7Mesoappendix hernia: an unusual internal hernia Clin Surg J Vinay HG Reddy R Kumar K 111332020 https://www.researchgate.net/profile/Vinay-H-G/publication/343135597_Mesoappendix_Hernia_An_unusual_Internal_Hernia/links/6035 c 2b 9a 6fdcc 37a 849778 b/Mesoappendix-Hernia-An-unusual-Internal-Hernia.pdf
- 8The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int J Surg Sohrabi C Mathew G Maria N Kerwan A Franchi T Agha RA 1136114010920233701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗