Preliminary study on the feasibility of united compressed sensing with radial acquisition as a routine method for liver dynamic contrast-enhanced examination in elderly patients with malignancy
Heping Deng, Xiaolei Dong, Yu Zhang, Peng Zhou, Yakun He, Liu Yang

TL;DR
This study compares two MRI techniques for liver scans in elderly cancer patients, finding that one method improves image quality and patient comfort.
Contribution
The study demonstrates that united compressed sensing with radial acquisition (uCSR) is a feasible and comfortable alternative for liver imaging in elderly cancer patients.
Findings
uCSR provides better image quality and reduces motion artifacts compared to 3D-VIBE.
uCSR allows scanning under free breathing, improving patient comfort and reducing scan failure rates.
While 3D-VIBE has higher SNR in some phases, uCSR is suitable for routine liver contrast-enhanced imaging.
Abstract
To explore the value of the united imaging compressed sensing with radial acquisition (uCSR) in liver dynamic contrast-enhanced examinations for elderly patients with malignancy. Hundred patients aged 65 years or over were randomly divided into two groups: 50 patients underwent liver dynamic contrast-enhanced scanning using the uCSR sequence during free breathing, and 50 patients underwent scanning using the three-dimensional volume interpolated breath-hold examination (3D-VIBE) sequence while holding breath. Two radiologists independently and subjectively evaluated the overall image quality and image artifacts with a five-point scale. Concurrently, two technologists measured the signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of the arterial, portal venous and delay phase images in both groups. uCSR has superior overall image-quality and image-artifact scores (z =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
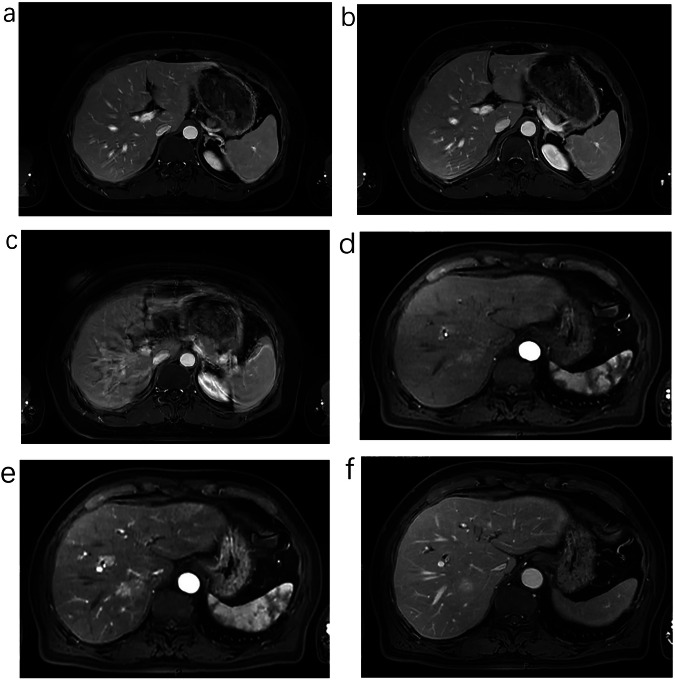 Figure 1
Figure 1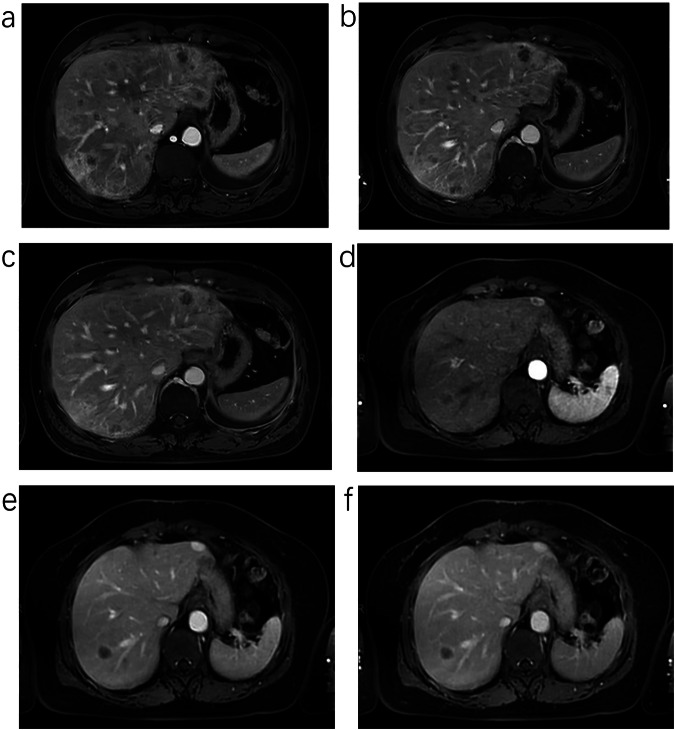 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced MRI Techniques and Applications · MRI in cancer diagnosis · Medical Imaging Techniques and Applications
Introduction
Population aging in China is accelerating, and the proportion of individuals aged ≥ 65 years is increasing [1]. Thus, the proportion of elderly patients who undergo liver magnetic resonance imaging (MRI) examinations is increasing. Because the liver is a dual blood supply organ, a three-phase scan (i.e., arterial, portal vein, and delayed phases) is particularly important. Routine liver dynamic contrast-enhanced scanning uses a sequence called three-dimensional volume interpolated breath-hold examination (3D-VIBE) [2]. This technique adopts the linear K-space filling method, which requires a high level of patient cooperation because scanning is performed during breath-holding. Each breath-holding period lasted approximately 15–20 s, and the number of breath-holding cycles ranged between 4 to 7 times. However, elderly patients, particularly those with malignancy, cannot perform breath-holding for 3D-VIBE. Thus, motion artifacts appear. Consequently, respiratory motion artifacts may appear in the images and render these images inadequate for clinical diagnosis [3]. Current imaging techniques can ensure dynamic contrast-enhanced liver scanning in a free-breathing state, including extra-dimensional golden-angle radial sparse parallel (XD-GRASP) with additional dimensions [4], Cartesian sampling, extra-dimensional VIBE (XD-VIBE) technology [5] and United Imaging compressed sensing with radial acquisition (uCSR). The uCSR technique combines compressed sensing technology, active aortic signal monitoring, automatic respiratory signal extraction, and 3D radial acquisition with star-shaped K-space filling technology. This technique allows dynamic contrast-enhanced scanning during free breathing. To improve the comfort of elderly patients during examinations, and avoid examination failure due to the inability of elderly individuals to cooperate with breath-holding, this study compared the uCSR with that of the conventional breath-holding 3D-VIBE and evaluated whether the uCSR technique could replace the conventional breath-holding 3D-VIBE and serve as a routine liver dynamic contrast-enhanced scanning method for elderly patients with malignancy.
Materials and methods
General information
A prospective study was conducted between March 2023 and July 2024 and involved elderly patients aged ≥ 65 years who underwent liver MRI examinations. The inclusion criteria were as follows: (1) age of ≥ 65 years; (2) presence of malignancy (e.g., hepatocellular carcinoma, cholangiocarcinoma, ovarian cancer, cervical cancer, lung cancer, and other malignancies); (3) absence of contraindications or history of allergies to MRI contrast agents; (4) absence of renal function abnormalities; and (5) complete imaging data without metallic artifacts in the examination areas. The study included 100 cases: 59 males and 41 females. The patients’ age was 68.00 years (66.00–71.00). The participants provided informed consent, and the study was approved by the hospital’s Medical Ethics Committee (approval number: SCCHEC-02-2021-009).
Instrumentation and methods
Scanning was performed using a United Imaging 3.0-T MRI scanner (UMR 780; United Imaging, Shanghai, China) equipped with an 18-channel phased-array body coil and a 32-channel spine coil. The patients were placed in the supine position with their heads first and their hands placed down on both sides of the body. A 6-h fast and water restriction period was required before the examination, and an indwelling needle was inserted into the elbow vein for contrast agent injection. Patients who underwent breath-holding liver dynamic contrast-enhanced examinations using the 3D-VIBE sequence were included in the 3D-VIBE group, whereas those who underwent free-breathing liver dynamic contrast-enhanced examinations using the uCSR technique were included in the uCSR group. Patients who failed to perform adequate breath-holding during T_1_-weighted imaging were automatically included in the uCSR group. Each group comprised 50 patients who were randomly allocated using the RANDBETWEEN (small value, large value) function of Excel, and the same scanning sequences were used for both groups, including consistent T_2_-weighted imaging (T_2_WI) in the coronal and transverse planes and 3D-VIBE imaging in the transverse plane. The 3D-VIBE group underwent three-phase scanning (i.e., arterial, portal venous, and delay phases), and the 3D-VIBE sequence was used during breath-holding. The uCSR group underwent uCSR sequence scanning during free breathing, and images for the arterial, portal venous, and delay phases were reconstructed. The scanning parameters of the T2-weighted imaging (T_2_WI), 3D-VIBE and uCSR sequence are shown in Table 1. The uCSR settings were as follows: pre-contrast phase 1 (temporal resolution for reconstruction, 45 s), arterial phase 2 (temporal resolution for reconstruction, 15 s), portal venous phase 1 (temporal resolution for reconstruction, 30 s), delay phase 1 (temporal resolution for reconstruction, 40 s), arterial input function, and region of interest (ROI) in manual mode (ROI diameter 10 mm). The 3D-VIBE sequence was performed with contrast injection triggered after 17 s for the arterial phase scan, 50 s for the portal phase scan, and 180 s for the delay phase scan. Then, 10 s after the start of the uCSR sequence, a high-pressure injector was used for the venous injection of the contrast agent (Gadopentetate Dimeglumine) at a speed of 2.0 mL/s. The contrast agent dose was calculated according to the patient’s weight (0.2 mL/kg). After the contrast agent was injected, 15 mL of saline was injected at the same rate as a saline flush.Table 1. The scanning parameters of T_2_WI, 3D-VIBE and uCSR,The scanning parametersT_2_WI3D-VIBEuCSRFOV400 × 300 mm400 × 280 mm400 × 280 mmTR3001 ms3.42 ms3.08 msTE82.68 ms1.56 ms1.4 msSlice thickness5 mm5 mm5 mmSlice gap1 mmNoneNoneOversampling20%0%0%Matrix256 × 230320 × 288256 × 256Phase encodingA > PA > PA > PFlip angle90°10°10°Number of averages111Concatenations211Method for fat suppressionChemical saturationChemical saturationChemical saturationCompressed sensing acceleration factor/2.62Number of spokes//3420Phase cycling//Mode adaptiveScan time36 s16 s310 sFOV field of view, TR repetition time, TE echo time.
Image quality evaluation
Qualitative analysis
All qualitative analyses were scored separately using a 5-point Likert scale. Two radiologists (radiologists 1 and 2, with 8 and 10 years of liver diagnosis experience, respectively) blindly evaluated the images using a subjective scoring system. The evaluation included two aspects: 1. Overall image quality of the 3D-VIBE and uCSR groups The scoring criteria were as follows: 5 = excellent, image quality with no artifacts, accurate phase timing, and suitable for diagnostic purposes; 4 = good, image quality with minimal artifacts, accurate phase timing and suitable for diagnostic purposes; 3 = moderate, image quality with some artifacts, partial phase timing inaccuracies, and mostly suitable for diagnostic purposes; 2 = poor, image quality with phase timing inaccuracies and some lesions not clearly visible, affecting diagnostic accuracy; 1 = very poor, image quality unsuitable for disease diagnosis. 2. Image artifacts (not limited to respiratory motion artifacts) in the 3D-VIBE and uCSR groups. The scoring criteria were as follows: 5 = excellent, no artifacts present; 4 = good, slight respiratory motion artifacts or slight radial artifacts; 3 = moderate, some respiratory motion artifacts or radial artifacts, generally suitable for diagnostic purposes; 2 = poor, significant artifacts affecting diagnosis; 1 = very poor, severe artifacts, unable to provide diagnostic recommendations.
Quantitative analyses
Two experienced MRI technicians (technicians 1 and 2, with 7 and 10 years of experience, respectively) blindly measured the signal intensities of the liver parenchyma (SI_liver_) and erector spinae muscle (SI_muscle_) and the background signal standard deviation (SD_background_) on the same anatomical level in the three-phase images of both groups. The measurement levels for the signal intensity of the liver parenchyma and erector spinae were conducted at the level of the porta hepatis. The liver measurement area was confined to the right posterior hepatic parenchyma, whereas the erector spinae measurement area was restricted to the right erector spinae muscle tissue. The ROIs for each measurement had a diameter of < 0.5 cm. Three measurements were obtained and averaged, and the signal-to-noise ratio (SNR = SI_liver_ / SD_background_) and contrast-to-noise ratio (CNR = (SI_liver_ − SI_muscle_) / SD_background_) were calculated.
Statistical analysis
Statistical analyses were performed using SPSSPRO (version 1.1.22) [6]. The Shapiro–Wilk test was used to evaluate the normality of the continuous variable distribution. Categorical or enumeration parameters are described as numbers (percentages), whereas continuous variables are expressed as the means ± standard deviations or the (medians (interquartile, ranges (IQRs)), as appropriate. The Mann–Whitney test was used for data that did not conform to the normal distribution, and the independent samples t-tests were used for data that conformed to the normal distribution. The intraclass correlation coefficient (ICC) was used to assess the inter- and intra-observer consistency of the data collected by the two radiologists and two technicians (< 0.2, poor consistency; 0.2–0.4, fair consistency; 0.4–0.6, moderate consistency; 0.6–0.8, good consistency; 0.8–1.0, excellent consistency). p-values < 0.05 were used to indicate statistical significance.
Results
Basic characteristics of the patients
Fifty-seven patients were initially included in the 3D-VIBE group; however, seven patients were excluded because of their inability to hold their breath. Approximately 87.7% of the patients in the 3D-VIBE group could perform breath-holding. The uCSR group comprised 50 patients, all of whom met the requirements and did not require breath-holding. The 3D-VIBE group had an average age of 68.00 years (66.00, 70.25), whereas the uCSR group had an average age of 67.00 years (66.00, 72.00). No statistically significant difference in age was found between the groups (z = −0.215, p = 0.830). The 3D-VIBE group comprised 19 females and 31 males, whereas the uCSR group comprised 22 females and 28 males (Table 2); however, no statistically significant difference in sex distribution was found between the groups (χ^2^ = 0.372, p = 0.542).Table 2. The demographics of patientsDemographicsThe 3D-VIBE groupThe uCSR groupAge (years)68.00 (66.00, 70.25)67.00 (66.00, 72.00)Sex (females/males)19/3122/28Types of malignancyOvarian cancer31Cervical cancer24Hepatocellular carcinoma74Lung cancer810Rectal cancer63Breast carcinoma22Prostate cancer52Nasopharyngeal carcinoma34Glioma01Gallbladder carcinoma11Lymphoma10Colon cancer23Cholangiocarcinoma13Malignant melanoma10Renal cancer13Pancreatic cancer12Laryngeal cancer10Bladder cancer11Tongue cancer01Thyroid cancer01Carcinoma of penis11Gastric cancer42Laryngeal cancer01
Qualitative analysis
Overall image quality score
The mean score for the 3D-VIBE group was 4.00 (4.00, 4.00), and the mean score for the uCSR group was 4.00 (4.00, 5.00). The results exhibited a statistically significant difference in the scores between the groups (z = 2.342, p = 0.019). This statistical result indicated that the overall image quality score was better in the uCSR group than in the 3D-VIBE group as shown in Fig. 1 and Table 3.Fig. 1a–c Female, 65 years old, cervical cancer, liver dynamic contrast-enhanced scanning utilizes 3D-VIBE, Arterial Phase (a) is incorrect and slight breathing artifact, Portal Venous Phase (b) slight breathing artifact, and Delay Phase (c) significant respiratory artifact; overall image quality Score is 3. d–f Male, 68 years old, cholangiocarcinoma, liver dynamic contrast-enhanced scanning utilizes uCSR, Arterial Phase (d), Portal Venous Phase (e) and Delay Phase (f) have excellent image quality and accurate phase; the score is 5Table 3Qualitative analysisGroupMedian (interquartile range)Frequencyz**p-value12345Overall image quality score (3D-VIBE)4.00 (4.00, 4.00)02829112.3420.019Overall image quality score (uCSR)4.00 (4.00, 5.00)0023018Image artifact score (3D-VIBE)4.00 (4.00, 4.25)011027122.1050.035Image artifact score (uCSR)4.00 (4.00, 5.00)00231173D-VIBE the three-dimensional volume interpolated breath-hold examination, uCSR the united imaging compressed sensing with radial acquisition
Image artifact score
The mean score for the 3D-VIBE group was 4.00 (4.00, 4.25), whereas that for the uCSR group was 4.00 (4.00, 5.00). The results exhibited a statistically significant difference in the scores between the two groups (z = 2.105, p = 0.035). This statistical result indicated that the uCSR group had better control over image artifacts than the 3D-VIBE group as shown in Fig. 2 and Table 3.Fig. 2a–c Male, 66 years old, adenocarcinoma of the lung, liver dynamic contrast-enhanced scanning utilizes 3D-VIBE; client held his breath well; however, the boundary of blood vessels is blurred in the image, and some of them appear as bilateral shadows in Arterial Phase (a), Portal Venous Phase (b) and Delay Phase (c), the image artifact score is 3. d–f Female, 68 years old, hepatic metastases and hemangioma, liver dynamic contrast-enhanced scanning utilizes uCSR; there are no respiratory motion artifacts and other atypical motion artifacts in Arterial Phase (d), Portal Venous Phase (e) and Delay Phase (f), there are slight radial artifacts in Arterial Phase (d), the image artifact score is 4
Quantitative analyses
Arterial phase: The mean SNR and CNR values for the 3D-VIBE group were 388.40 (320.85, 424.08) and 150.10 (110.60, 192.20), respectively, whereas those for the uCSR group were 280.65 (234.64, 345.25) and 136.00 (113.60, 185.33), respectively. A statistically significant difference in SNR was found between the groups (z = 4.988, p = 0.000); however, no significant difference in CNR was observed (z = 0.676, p = 0.499). The results revealed that 3D-VIBE images had a higher SNR than uCSR images, and the CNR did not significantly differ between the groups (Table 4).Table 4. Quantitative analysesGroupMeanz/t**p-valueThe SNR of arterial phase (3D-VIBE)388.40 (320.85, 424.08)4.9880.000The SNR of arterial phase (uCSR)280.65 (234.65, 345.25)The CNR of arterial phase (3D-VIBE)150.10 (110.60, 192.20)0.6760.499The CNR of arterial phase (uCSR)136.00 (113.60, 185.33)The SNR of portal venous phase (3D-VIBE)514.55 (426.78, 623.10)5.6740.000The SNR of portal venous phase (uCSR)368.80 (318.58, 415.95)The CNR of portal venous phase (3D-VIBE)259.10 ± 84.2693.6380.000The CNR of portal venous phase (uCSR)205.89 ± 59.959The SNR of delay phase (3D-VIBE)305.85 ± 57.2485.4710.000The SNR of delay phase (uCSR)240.54 ± 62.033The CNR of delay phase (3D-VIBE)94.95 (70.90, 130.70)1.2580.208The CNR of delay phase (uCSR)84.85 (73.13, 104.88)3D-VIBE three-dimensional volume interpolated breath-hold examination, uCSR united imaging compressed sensing with radial acquisition, SNR signal-to-noise ratio, CNR contrast-to-noise ratio
Portal venous phase: The mean SNR and CNR values for the 3D-VIBE group were 514.55 (426.78, 623.10) and 259.10 ± 84.269, respectively, whereas those for the uCSR group were 368.80 (318.58, 415.95) and 205.89 ± 59.959, respectively. A statistically significant difference in SNR was observed between the groups (z = 5.674, p = 0.000); however, no significant difference in CNR was observed (t = 3.638, p = 0.000). The results observed that 3D-VIBE images had higher SNR and CNR values than uCSR images (Table 4).
Delay phase: The mean SNR and CNR values for the 3D-VIBE group were 305.85 ± 57.248 and 94.95 (70.90, 130.70), respectively, whereas those for the uCSR group were 240.54 ± 62.033 and 84.85 (73.13, 104.88), respectively. A statistically significant difference in SNR was found between the two groups (t = 5.471, p = 0.000); however, no significant difference in CNR was observed (z = 1.258, p = 0.208). The results revealed that 3D-VIBE images had a slightly higher SNR than uCSR images, and the CNR did not significantly differ between the groups (Table 4).
Consistency analysis of subjective scores and objective measurements within and between the observer groups
Table 5 shows that the ICC values for all evaluation items within and between the observer groups were > 0.6 (intra-observer ICC: 0.891, 0.876, 0.904, and 0.943; inter-observer ICC: 0.838, 0.732, 0.867, and 0.908). The results revealed good data consistency within and between the observers.Table 5. Intra- and inter-observer variabilityIntra-observerInter-observerICC95% CIICC95% CIOverall image quality score0.8910.790–0.9410.8380.688–0.912Image artifact score0.8760.763–0.9330.7320.493–0.857SNR0.9040.818–0.9490.8670.746–0.928CNR0.9430.905–0.9730.9080.831–0.925ICC intraclass correlation coefficient, CI confidence interval, SNR signal-to-noise ratio, CNR contrast-to-noise ratio
Discussion
In this study, 57 patients were recruited in the 3D-VIBE group; however, seven patients could not hold their breath. Therefore, 12.3% of patients could not use the traditional 3D-VIBE technique because they could not hold their breath. Nevertheless, using the uCSR technique, which does not require breath-holding, all cases were completed successfully. Therefore, the tolerance of patients to the uCSR was significantly higher than that to 3D-VIBE, and uCSR ensured the comfort of patients during examinations. The main reason is that uCSR enables 3D star-like radial acquisition in the K-space, which greatly reduces the influence of respiratory motion on images in contrast to linear Cartesian sampling used in 3D-VIBE [7, 8]. Furthermore, uCSR automatically extracts respiratory signals and generates a respiratory curve. The time during the free-breathing state, when the chest and abdomen are relatively motionless, is longer at the end of expiration than at the end of inspiration. Therefore, we used the bottom of the curve (end of expiration) as a reference and matched the acquired signals throughout the entire respiratory cycle to the respiratory curve. Different weights were applied to the data acquired from different respiratory curves during image reconstruction. The corresponding weight decreased as the data moved away from the bottom of the respiratory curve. This method ensures the use of acquired data while further reducing the impact of respiratory motion on image quality. However, some respiratory models cannot achieve high-quality images, which can be obtained only when breathing is consistent and uniform and the respiratory cycles have the same amplitude [9, 10]. When deep and shallow breaths alternate randomly, the mismatch between the top and bottom of the respiratory curve in the horizontal line results in noticeable radial artifacts in the reconstructed images. Therefore, patients should be instructed to maintain a consistent and stable breathing pattern before the examination.
In our study, two radiologists with expertise in medical image diagnosis subjectively scored the overall image quality and image artifact suppression ability of the two groups from a diagnostic perspective. The overall image quality score was slightly better in the uCSR group than in the 3D-VIBE group. When the seven excluded cases were included in the 3D-VIBE group, the advantage of the uCSR group over the 3D-VIBE group in subjective scoring was more pronounced. The uCSR can better address motion and cardiac pulsation artifacts than 3D-VIBE because radial acquisition has stronger motion robustness than linear Cartesian sampling [11].
In 3D-VIBE, respiratory motion occurring at any time during the entire scanning period will result in arc-shaped artifacts in all reconstructed images in the phase-encoding direction. For example, even if breath-holding is good for most scans, slight abdominal motion in a short period at the end can still cause motion artifacts, which are related to the magnitude of respiratory motion. However, upon detailed observation of the uCSR images in each phase, radiating streak artifacts appear at varying degrees in each phase instead of the typical arc-shaped motion artifacts caused by Cartesian line sampling, leading to a decrease in image quality. These radiating streak artifacts are mainly due to the use of radial K-space acquisition in uCSR [12].
The subjective scoring indicated that the tolerance of radiologists toward motion artifacts in 3D-VIBE was significantly lower than that toward streak artifacts caused by radial K-space acquisition in uCSR. The streak artifacts in uCSR can be improved to some extent by adjusting the sequence parameters, particularly by increasing the number of spokes or reducing the temporal resolution of the reconstructed data. However, when highly accurate arterial phase image timing is required, excessive reduction in temporal resolution may lead to nonstandard arterial phase reconstruction and potential contamination of portal venous phase acquisition data.
The timing window of the data required for image reconstruction is crucial for achieving satisfactory image quality in each phase, particularly in the arterial phase. Early or late data acquisition can result in premature or delayed arterial phase. In uCSR, the time–signal curve of a vessel is obtained by manually labeling the curve, and variations in the labeled arterial signal are considered during data acquisition. Then, based on the arterial time–signal curve as a reference, the time point at which the curve reaches half of its peak height is considered the start time. The start time determines the starting point of arterial phase reconstruction. By using this method, the reconstruction of each phase ensures the accuracy of the dynamic enhancement, particularly in the arterial phase of the liver. In this study, the abdominal aorta at the level of the porta hepatis was used as the labeled vessel, and the time–signal curve of the abdominal aorta was obtained. The multi-phase images reconstructed based on this curve effectively meet the diagnostic requirements.
Currently, a technique called XD-GRASP is widely used in research on the dynamic contrast-enhanced scans of the liver, uterus, rectum and other organs during free-breathing conditions [5, 13–15] and in adaptive radiation therapy for moving organs [16, 17]. This technique classifies the continuously acquired K-space data into multiple under-sampled datasets with different motion states. It uses motion signals directly extracted from the data for image reconstruction. Another study [6, 9, 18] used a novel Cartesian sampling technique called the XD-VIBE for dynamic contrast-enhanced scans of the liver. In the reconstruction of multi-phase images, the same temporal resolution is used to evenly divide the time points, and data from adjacent time points are reconstructed to produce multi-phase images. In this study, the image qualities of the arterial, portal venous, and delay phase images, including SNR and CNR, were objectively evaluated. No significant difference in CNR was observed between the arterial and delay phases. In terms of other comparison parameters, 3D-VIBE outperformed uCSR. The most important factor affecting the SNR and CNR in the reconstructed images obtained using uCSR is the temporal resolution of each phase. Decreasing the temporal resolution increases the amount of reconstructed data and significantly improves the SNR and CNR of the images. However, the accuracy of the phase-to-phase registration limits the reduction in the temporal resolution of image reconstruction, particularly in the arterial phase. The requirements for temporal resolution are relatively lower in the portal venous and delay phases than in the arterial phase, allowing an increase in the data volume by reducing the temporal resolution and thereby improving the image quality. For example, in this study, the temporal resolution of uCSR sequence parameters during the portal venous and delay phases was significantly lower than that during the arterial phase. In the future, we can also improve the SNR and CNR of the reconstructed image by modifying the parameters.
Currently, few studies have explored the clinical application of the uCSR technology in the free-breathing dynamic contrast-enhanced liver scans in elderly patients with cancer, uCSR and XD-GRASP combine compressed sensing [19] and 3D radial acquisition with star-shaped K-space filling technology [20]. The compressed sensing can improve the time resolution and also obtain satisfactory image quality [21], and the star-shaped K-space filling technology can significantly inhibit respiration-induced motion artifacts. According to subjective evaluations, uCSR performed better than 3D-VIBE. This finding may be attributable to suboptimal respiratory coordination in elderly patients with cancer and varying degrees of respiratory artifacts in the images. Furthermore, the accuracy of the arterial phase timing significantly influenced the subjective evaluation of the diagnosing physicians.
Although the SNR and CNR of uCSR images were lower than those in the 3D-VIBE group, they still maintained a good level, and uCSR had a higher subjective score, which also suggested doctors’ affirmation of the quality of uCSR images. Thus, we conclude that the importance of image artifacts and phase timing accuracy outweighed the importance of SNR and CNR in clinical diagnosis. Therefore, uCSR can be routinely used for dynamic contrast-enhanced liver scans in elderly patients with cancer because it can improve patient comfort and reduce the rate of failure due to inadequate breath-holding capability.
The limitations and shortcomings of this study include the small number of collected cases, which may have affected the statistical results. Future studies should aim to increase the number of cases to address this limitation.
Supplementary information
Supplementary Data 1