Perioperative Hyperhidrosis: Case Reports of Two Patients and Literature Review
Yassine Ben Saad, Muhammad Jaffar Khan, Arunabha Karmakar, Muhammad Firas Alhammad, Muhammad Yousaf, Wajeeha Arshad, Moncef Ben Ghoulem Ben Saad

TL;DR
This paper discusses two cases of excessive sweating after surgery and suggests a standardized approach for managing this condition.
Contribution
The paper introduces a clinical algorithm for the first time to standardize the management of perioperative hyperhidrosis.
Findings
Two patients experienced excessive sweating after general anesthesia.
A clinical algorithm is proposed to guide the management of perioperative hyperhidrosis.
Abstract
Perioperative hyperhidrosis (POH) can present as excessive sweating within hours after anesthetic induction and may persist up to 24 hours postoperatively following general anesthesia. While commonly a benign finding, excessive or persistent POH can be disconcerting for the patient and can occasionally signify an underlying infection, electrolyte disturbances, or autonomic dysregulation. A systematic approach to managing POH has not been published. We report the cases of two patients with excessive sweating under general anesthesia, highlighting their clinical presentation and management. We also propose a clinical algorithm to standardize the management of POH.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
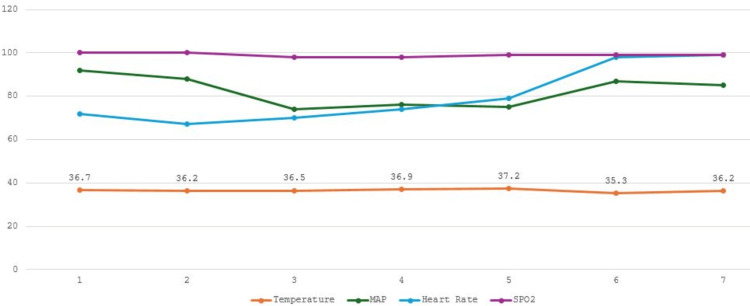 Figure 1
Figure 1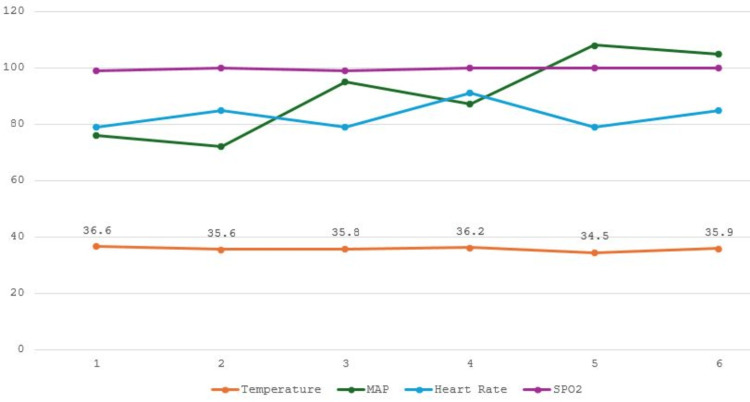 Figure 2
Figure 2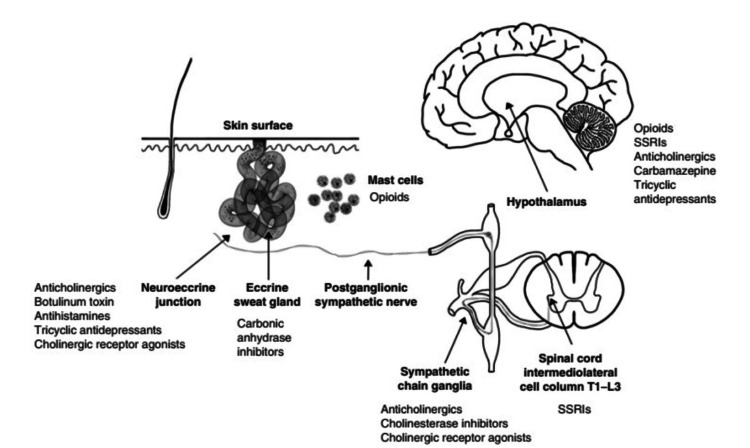 Figure 3
Figure 3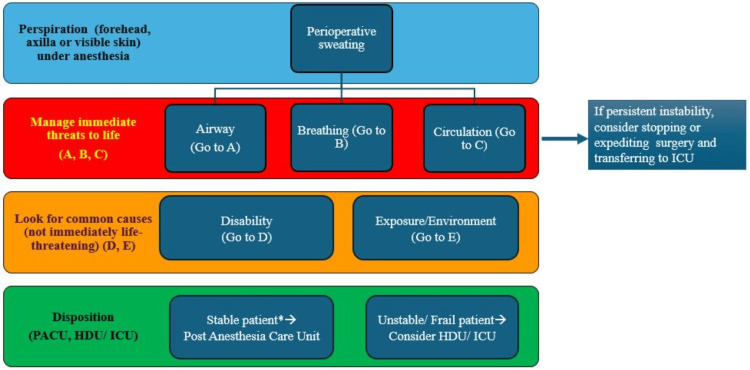 Figure 4
Figure 4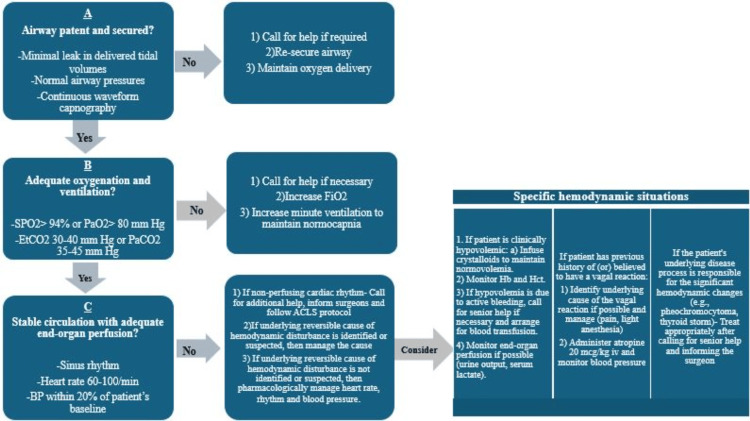 Figure 5
Figure 5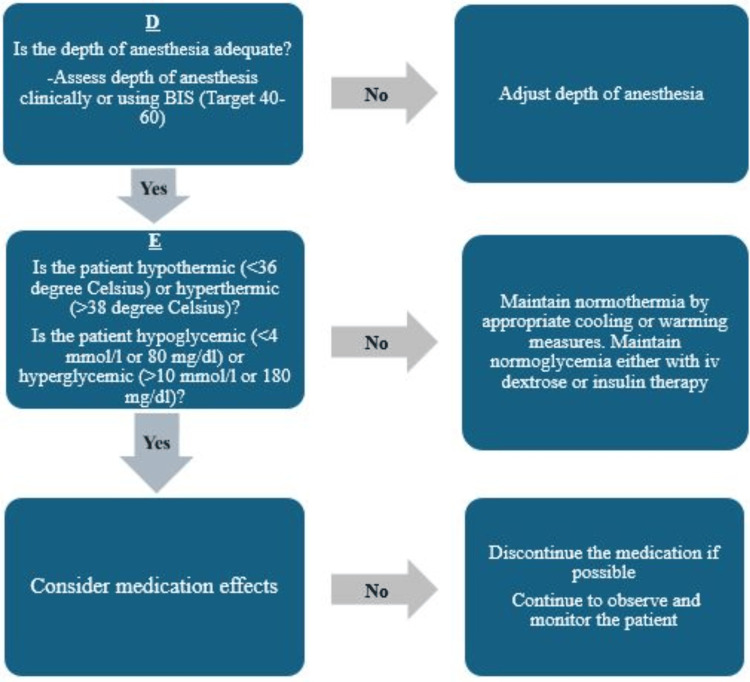 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSympathectomy and Hyperhidrosis Treatments · Thermal Regulation in Medicine · Restraint-Related Deaths
Introduction
Hyperhidrosis is characterized by excessive sweating, with a global incidence ranging from 2.5% to 18% [1]. However, perioperative sweating remains poorly studied, and its exact incidence is yet to be determined. Perioperative hyperhidrosis (POH), though not extensively documented, has been observed in various surgical contexts. A study focusing on patients undergoing elective cardiac surgery reported that 46% of participants experienced postoperative sweating, with 22% experiencing mild sweating and 24% experiencing moderate and profuse sweating [2]. POH can be mild or excessive, localized or generalized, self-limited or persistent, benign or concerning, or physiological or pathological/iatrogenic. However, the exact occurrence of POH depends on the patient population, type of surgery, and anesthetic technique. Notably, the World Health Organization - International Classification of Disease registry does not include POH as a distinct clinical entity, which may limit its reporting [3]. Perioperative sweating has been reported in multiple case studies, occurring both intraoperatively and postoperatively, with potential contributing factors such as physiological stress, metabolic imbalances, autonomic dysfunction, and the effects of anesthetic drugs, with symptoms persisting for up to 24 hours postoperatively [3-6]. Intraoperative sweating has been reported in patients who experience significant temperature dysregulation during surgery or a high-stress response during anesthesia. While most cases of POH are benign and self-limiting, they are sufficiently prevalent and alarming to warrant patient assessment before clearance for or discharge from surgery.
We report the cases of two patients with POH that developed during emergence from general anesthesia and tracheal extubation, persisted in the postanesthesia care unit (PACU), and was associated with hypothermia. We describe our clinical observations, correlate the findings with the literature, and provide insights into the mechanisms and potential causes of sweating in the perioperative period.
Case presentation
Patient 1
A 33-year-old male with ASA physical status 2, obesity (weight 105 kg, BMI 31.18 kg/m^2^), and a history of type 2 diabetes mellitus was scheduled for elective incisional hernia repair. He had a previous history of sleeve gastrectomy, which was complicated by thrombosis of the superior mesenteric vein and portal vein, leading to bowel ischemia and necessitating laparotomy. He was receiving 20 mg of rivaroxaban daily for anticoagulation, which was held 48 hours before his scheduled surgery, and metformin for blood glucose control.
On the day of surgery, the patient was stable preoperatively. Anesthesia was induced intravenously with 200 mg (2 mg/kg) propofol, 200 mcg (2 mcg/kg) fentanyl, and 50 mg (0.5 mg/kg) rocuronium. Anesthesia was maintained with inhaled sevoflurane and intravenous (IV) remifentanil infusion. Active warming device was applied to achieve normothermia. Other intraoperative medications included IV ketorolac (30 mg), dexamethasone (8 mg), acetaminophen (1 gm), and morphine (10 mg). He was infused with 2000 mL of crystalloids (Ringer’s lactate) and 250 mL of colloids (purified protein fraction 5%). The patient was vitally stable intraoperatively and normothermic (Figure 1).
Perioperative vitals of the first patient.The x-axis is marked with seven points representing various time periods during the surgery when the patient's vitals were recorded: 1, preoperative (baseline line) vitals; 2, 5 minutes post-induction of general anesthesia; 3, first hour post-induction; 4, second hour post-induction; 5, vitals at emergence; 6, vitals at PACU admission; and 7, one hour after PACU admission.MAP, mean arterial pressure; PACU, postanesthesia care unit; SPO2, oxygen saturation
Emergence from anesthesia and tracheal extubation were uneventful but were associated with profuse sweating. Post-emergence, the patient was alert, hemodynamically stable, and reported no pain but continued to sweat profusely and became hypothermic without shivering. In the PACU, his body temperature was recorded as 35.3°C. The serum glucose level was normal.
He was treated with active air warming and draped with a sheet. Sweating continued for one and a half hours and then subsided gradually. As the patient was vitally stable and reported no pain, he was transferred to the ward for continuing care.
Patient 2
A 55-year-old male with an ASA physical status of 2 was scheduled for laparoscopic cholecystectomy. He had hypertension, which was well controlled with amlodipine, and type 2 diabetes mellitus, which was well controlled with metformin.
On the day of surgery, anesthesia was induced intravenously with propofol 150 mg (2 mg/kg), fentanyl (2 mcg/kg), and rocuronium (0.6 mg/kg) and maintained with sevoflurane inhalation. Additionally, the patient received IV dexamethasone 8 mg, ketorolac 30 mg, acetaminophen 1 gm, and morphine 10 mg for analgesia. He received one liter of Ringer’s lactate. His body temperature was maintained with active warming. Toward the end of the procedure, sweating was observed on his face and arms, despite a normal body temperature of 36.2°C. Active warming was discontinued, and the patient was transferred to the PACU after emergence and extubation. The perioperative vital signs are shown in Figure 2.
Perioperative vitals for the second case. The x-axis is marked with six points representing various time periods during the surgery when the patient’s vitals were recorded: 1, preoperative (baseline line) vitals; 2, 5 minutes post-induction of general anesthesia; 3, first hour post-induction; 4, vitals at emergence; 5, vitals at the admission to PACU; and 6, one hour after admission to the PACU.MAP, mean arterial pressure; PACU, postanesthesia care unit; SPO2, oxygen saturation
The patient’s body temperature in the PACU was 34.5°C, with continued sweating. The random blood sugar concentration was 10.4 mmol/L. Active air warming was utilized to normalize his temperature. The sweating continued for one hour and then subsided.
Discussion
Our patients had persistent POH with postoperative hypothermia after otherwise uneventful general anesthesia. Both had recovered with expectant management. When excessive sweating occurs during emergence, it is essential to assess the patient's overall clinical status, hemodynamics, pain levels, medication effects, and body temperature. Potential interventions include pharmacological measures such as anticholinergic agents to reduce sweat gland activity or active warming techniques to counteract hypothermia [6]. However, in both our cases, they were managed conservatively, and the patients’ condition improved spontaneously.
Common causes of POH include covering patients with surgical drapes, surgical stimulation, autonomic dysregulation, medication-related effects, hypoglycemic episodes, or other underlying causes [7,8].
Human eccrine and apocrine sweat glands are involved in sweating. Eccrine glands are present throughout the body's skin surface and are the predominantly active sweat glands. In contrast, apocrine glands become active after puberty when stimulated by hormonal changes. Both glands have sympathetic innervation mediated adrenergically and are involved primarily in emotional sweating triggered by stress, fear, and pain [9,10].
The hypothalamic thermal center is responsible for regulating body temperature and receives stimuli from temperature-sensing nerves or directly senses the temperature of the blood. Additionally, localized sweating centers have been identified in the thoracic and lumbar regions [9]. Sweating due to increased body temperature is known as thermal sweating, which serves the primary purpose of heat dissipation through evaporation. It is reflexive and can precede a rise in body temperature when exposed to external heat. Thermal sweating tends to be generalized throughout the body. Physiologically, if one area of the body is warm, sweating can occur across the entire body.
Sweating can also be triggered by autonomic activity through sympathetic (mediated by adrenaline and noradrenaline) or parasympathetic activation (mediated by acetylcholine). While the primary innervation of sweat glands is cholinergic, adrenaline and noradrenaline also play a role [9,11]. An individual's specific autonomic response, whether sympathetic or parasympathetic, cannot be accurately predicted in advance. Typically, an increase in heart rate and blood pressure signifies a sympathetic response, whereas a decrease in blood pressure and pulse rate, accompanied by cold sweat, indicates a parasympathetic response. Under general anesthesia, both sympathetic and parasympathetic-mediated sweating can occur [11,12]. Sympathetic discharge can result from anxiety, pain, or hypercarbia in the presence of inadequate anesthesia. Sweating may also be accompanied by bradycardia, nausea, and hypotension as part of a generalized vagal reaction or as a thermoregulatory response to hyperthermia. During surgical stimulation, in the lighter plane of anesthesia, an enhanced sympathetic response can cause an increase in blood pressure and pulse rate, with or without sweating, but sweating is mostly induced by sympathetic system stimulation. Both hypoxia and hypercarbia can lead to increased blood pressure and sweating [13]. Hemorrhage and pain may elicit a parasympathetic response, resulting in cold sweat [11,13].
Sweating can also be caused by multiple drugs that the patient may be taking or has received intraoperatively. Special attention is warranted for patients taking antidepressants, as sweating can be indicative of serotonin syndrome, which is typically accompanied by high blood pressure and tachycardia. Patients who are taking selective serotonin reuptake inhibitors (SSRIs) along with pain medications such as tramadol, meperidine, and fentanyl, and anti-nausea medications such as ondansetron or migraine medications may be at risk of developing serotonin syndrome. Other drugs that contribute to perioperative sweating are nonsteroidal anti-inflammatory drugs (NSAIDs), beta-agonists, proton pump inhibitors, steroids, oral hypoglycemic drugs, and triptans [8,13,14].
Opioid-induced sweating has been well documented [4,15]. Specifically, two cases have been reported in which patients who underwent spinal anesthesia with intrathecal morphine injections experienced excessive sweating and hypothermia [5,16]. The regulation of body temperature involves multiple opioid receptors in the hypothalamus, and the distribution of spinal opioids may interfere with the temperature set point [4]. Furthermore, opioids such as morphine can stimulate mast cells, a type of immune cell, leading to the release of histamine, which can cause skin warmth and sweating [15]. Excessive sweating has also been associated with the use of oral methadone and transdermal fentanyl, possibly again attributed to opioid-induced mast cell release of histamine [8,17]. Similarly, patients may experience sweating after receiving remifentanil, a potent opioid analgesic [6].
Hypoglycemia can also cause sweating, and blood sugar must be monitored in diabetic patients who are under anesthesia. Other potential causes of sweating include vitamin D deficiency or hyperthyroidism. In addition to medication-related and preexisting disease causes, excessive warming and draping during procedures can result in sweating [18].
Cold-induced sweating syndrome is a genetic disorder inherited in an autosomal recessive manner. It is characterized by dysmorphic features and sweats on the face, arms, and posterior chest when exposed to temperatures below 18-22°C [19]. Nervousness can also trigger sweating in individuals with this condition.
Notable rare or serious clinical pathologies causing POH have also been described. Shapiro syndrome is a rare condition characterized by recurrent hypothermia, sweating, and chills due to agenesis of the corpus callosum [20]. Pheochromocytoma is a tumor of the adrenal glands characterized by excessive cortisol release that presents with hypertension and a triad of diaphoresis, headaches, and palpitations [21]. In patients with pheochromocytoma, the release of adrenaline can lead to significant sweating. Similarly, familial dysautonomia (FD) is a rare genetic disorder marked by autonomic dysfunction, recurrent pulmonary infections, esophageal dysmotility, spinal abnormalities, and episodic dysautonomic crises. These crises present with symptoms such as rash, vomiting, sweating, and hypertension. Patients with FD are prone to frequent anesthetic complications [22].
Various strategies can be employed to mitigate sweating based on the cause. These include measures to prevent hyperthermia, maintain the depth of anesthesia, regulate blood sugar, ensure oxygenation and ventilation, address any underlying metabolic conditions, and mitigate sympathetic stimuli. Vasopressors may be administered to maintain blood pressure, and supplemental fluid may be required for normovolemia and to maintain adequate cardiac output (Figure 3).
Schematic representation showing the major sites of action of classes of drugs that commonly influence sweating.The sweating pathway begins in the hypothalamus and extends to the intermediolateral column, from which arise preganglionic sympathetic fibers that leave the spinal cord and synapse within the sympathetic chain ganglia. Postganglionic sympathetic nerves emerge from these ganglia and travel alongside arteries to reach their subdermal targets, the eccrine sweat glands. Drugs can interact with each level of this pathway.Reproduced with permission from [4].SSRI, selective serotonin reuptake inhibitor
As POH may be a red flag for an underlying physio-pathological condition, a stepwise approach helps rule out significant pathologies, deliver appropriate care, and mitigate intraoperative mortality. The algorithm in Figures 4-6 is a suggested approach proposed by the authors on the basis of their experience.
*Suggested algorithm to approach perioperative sweating (continued).Stability refers to cardiopulmonary stability. Continued sweating in an otherwise stable patient can still be observed in the PACU.HDU, high dependency unit; ICU, intensive care unit; PACU, postanesthesia care unit
Suggested algorithm to approach perioperative sweating (continued).ACLS, advanced cardiac life support; EtCO2, end tidal carbon-dioxide; FiO2, fraction of inspired oxygen concentration; Hb, hemoglobin; Hct, hematocrit; iv, intravenous; kg, kilogram; mcg, microgram; PaCO2, arterial partial pressure of carbon-dioxide; PaO2, arterial partial pressure of oxygen; SPO2, oxygen saturation
Suggested algorithm to approach perioperative sweating.BIS, bispectral index; iv, intravenous
Both patients exhibited stable hemodynamics, maintained adequate oxygen saturation, and had normal end-tidal carbon dioxide levels intraoperatively. During a follow-up assessment three months later, both patients were reported to be in good health, with no complications or concerns related to their perioperative management.
Conclusions
The exact etiology of POH in our patients was not identified. It is plausible that a combination of active warming and medications such as steroids, morphine, and NSAIDs may have contributed. Remarkable features of POH in our patients included its persistence for 60-90 minutes postoperatively, associated hypothermia, and self-resolution.
POH is caused by various factors, such as surgical stimulation, opioid administration, or alterations in the autonomic nervous system associated with aging. It is crucial to promptly evaluate the underlying causes of excessive sweating during anesthesia, as it could indicate a serious underlying medical issue or potentially lead to complications on its own. Timely assessment and identification of the root cause are essential for ensuring appropriate management and intervention to address sweating and mitigate any associated risks or complications. If the patient is otherwise fit, they may recover with expectant management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hyperhidrosis: a targeted literature review of the disease burden J Dermatol Oshima Y Fujimoto T Nomoto M Fukui J Ikoma A 122712365020233751913410.1111/1346-8138.16908 · doi ↗ · pubmed ↗
- 2Awareness and sweating among patients undergoing elective cardiac surgery under hypothermic cardiopulmonary bypass Med Pulse Int J Anesthesiol Mathew A Mathew M Balamurugan B 1116222022 https://medpulse.in/Anesthsiology/html_22_1_3.php
- 3International Statistical Classification of Diseases and Related Health Problems 10th Revision 2 2025 2019 https://icd.who.int/browse 10/2019/en
- 4Persistent hypothermia and excessive sweating following intrathecal morphine administration in a teenage boy: a case report Anesth Pain Med Ferraz S Caria T Da Silva AV Candeias MJ Cenicante T 08201810.5812/aapm.66724 PMC 597036329868463 · doi ↗ · pubmed ↗
- 5Hypothermia and excessive sweating following intrathecal morphine in a parturient undergoing cesarean delivery Reg Anesth Pain Med Sayyid SS Jabbour DG Baraka AS 1401432820031267762510.1053/rapm.2003.50043 · doi ↗ · pubmed ↗
- 6Unusual excessive sweating and hypothermia during hysterectomy under general anesthesia: a case report Anesth Pain Med Kim H Jee D Lee H 321324102015
- 7Definition and treatment of primary hyperhidrosis J Dtsch Dermatol Ges Wörle B Rapprich S Heckmann M 625628520071761061510.1111/j.1610-0387.2007.06409.x · doi ↗ · pubmed ↗
- 8Drug-induced hyperhidrosis and hypohidrosis: incidence, prevention and management Drug Saf Cheshire WP Fealey RD 1091263120081821778810.2165/00002018-200831020-00002 · doi ↗ · pubmed ↗