Acute Generalized Exanthematous Pustulosis Following the Administration of Cephalexin: A Case Report and Review of the Literature
Yoshihito Mima, Tsutomu Ohtsuka

TL;DR
This paper reports a rare case of a severe skin reaction (AGEP) caused by the antibiotic cephalexin and discusses possible links to viral infections.
Contribution
The paper presents a new case of cephalexin-induced AGEP and is the first to use the EuroSCAR score for its diagnosis.
Findings
AGEP occurred two days after cephalexin administration and was confirmed by subcorneal pustules and a EuroSCAR score of 9.
The patient had pre-existing cold symptoms, suggesting a possible role of viral infections in triggering AGEP.
Only six cases of cephalexin-induced AGEP have been reported, with this being the first to use the EuroSCAR score for diagnosis.
Abstract
Acute generalized exanthematous pustulosis (AGEP) is a severe cutaneous reaction characterized by the sudden onset of numerous sterile, non-follicular pustules on an erythematous and edematous background, usually associated with fever. AGEP is commonly triggered by medications, including antibiotics, anticancer agents, and hydroxychloroquine, but infections and vaccinations, such as parvovirus B19 and COVID-19 vaccines, have also been implicated. We report a case of AGEP which developed two days after the administration of cephalexin. The pathological findings of subcorneal pustules and European Severe Cutaneous Adverse Reactions (EuroSCAR) score of 9 confirmed the diagnosis of AGEP. To date, only six cases of cephalexin-induced AGEP have been reported. Among these, five cases involved patients without underlying conditions, while one case occurred in a patient with pustular psoriasis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1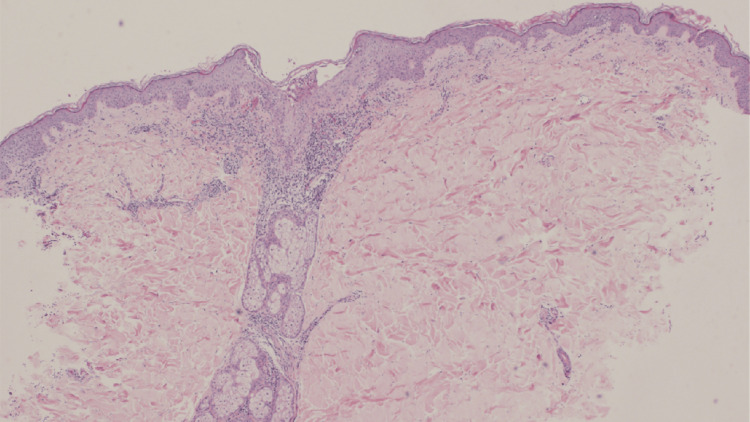 Figure 2
Figure 2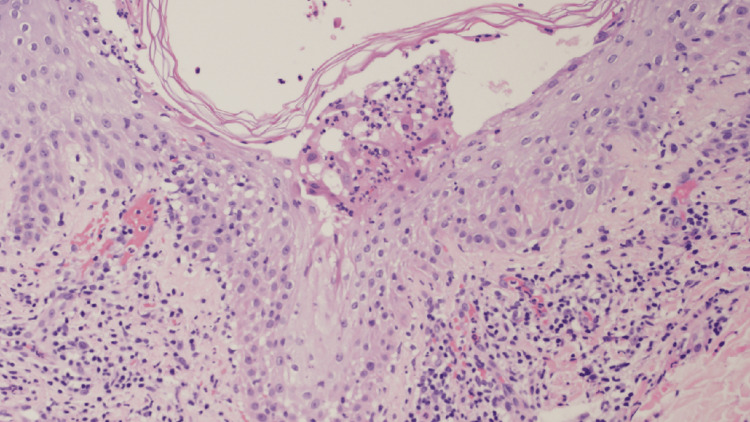 Figure 3
Figure 3| Criteria | Description | Score |
| Morphology | ||
| Pustules | Typical | 2 |
| Erythema | Typical | 2 |
| Distribution | Typical | 2 |
| Postpustular desquamation | No | 0 |
| Course | ||
| Mucosal involvement | Yes | 0 |
| Acute onset (<24 hours) | Yes | 0 |
| Resolution of pustules and erythema (<15 days) | Yes | 0 |
| Fever (>38℃) | No | 0 |
| Blood neutrophil count (>7000 μ/L) | Yes | 1 |
| Histopathology | ||
| Skin biopsy | Subcorneal pustule with mild edema | 2 |
| Total score | - | 9 |
| Case | Age | Sex | Past medical history | Diagnosis of AGEP | Symptoms | Onset time | Additional allergy test | Treatment for AGEP |
| DaCunha et al. [ | 35 | Woman | None | Clinical course and histopathological findings | Fever, sweating, and fatigue | Three days after intake | None | Oral corticosteroid |
| Holscher et al. [ | 58 | Male | None | Clinical course | Fever, vomiting, diarrhea, and respiratory failure | Five days after intake | None | Oral corticosteroid and topical corticosteroids |
| Abbas et al. [ | 54 | Female | Pustular psoriasis | Clinical course and histopathological findings | Fever, blisters, and epidermal detachment | Two days after intake | None | Oral cyclosporine and topical corticosteroids |
| Arroyo et al. [ | 47 | Female | Unknown | Clinical course and histopathological findings | Unknown | Unknown | None | Topical corticosteroids |
| Choon et al. [ | Unknown | Unknown | Unknown | Unknown | Unknown | One day after intake | Unknown | Unknown |
| Our case | 47 | Male | None | Clinical course and histopathological findings | Fever and fatigue | Two days after intake | None | Topical clobetasol propionate and oral olopatadine |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Heparin-Induced Thrombocytopenia and Thrombosis · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Acute generalized exanthematous pustulosis (AGEP) is a condition characterized by the acute onset of diffuse edematous erythema, particularly in intertriginous areas and the face, with numerous non-follicular, sterile pustules developing on the erythematous skin. Patients may experience associated burning sensations or pruritus, and approximately 20% of cases present with mucosal involvement, primarily affecting the oral cavity. Mucosal lesions are typically mild and limited to a single site. The majority of AGEP cases present with fever exceeding 38°C and leukocytosis, often accompanied by mild eosinophilia [1]. AGEP is commonly triggered by medications, including antibiotics, anticancer agents, and hydroxychloroquine, typically occurring within a week following exposure to the causative drug [2]. In addition, infections or virus vaccinations, such as parvovirus B19 and COVID-19 vaccination, have also been considered to trigger the development of AGEP [3,4]. Clinically, the pustules of AGEP resolve spontaneously within 4-10 days, often leaving behind desquamation and postinflammatory hyperpigmentation. The prognosis is generally favorable, but in elderly or immunocompromised patients, high fever or secondary bacterial infections can pose life-threatening risks [1].
Several conditions require differential diagnosis from AGEP, including drug reaction with eosinophilia and systemic symptoms (drug-induced hypersensitivity syndrome), toxic epidermal necrolysis, subcorneal pustular dermatosis, generalized pustular psoriasis, bacterial folliculitis, acne, dermatophytosis, varicella, Kaposi varicelliform eruption, Sweet’s syndrome, impetigo, autoimmune blistering diseases, and Behçet’s disease [1]. Histopathologically, AGEP is characterized by spongiform subcorneal or intraepidermal pustules, prominent dermal papillary edema, and perivascular neutrophilic infiltration, with occasional eosinophil degranulation [5,6]. In some cases, perivascular neutrophilic infiltration and keratinocyte necrosis suggestive of vasculitis may be observed. However, epidermal hyperplasia, a hallmark of psoriasis, is typically absent [5,6].
The diagnosis of AGEP is based on clinical presentation and histopathological findings, with the European Severe Cutaneous Adverse Reactions (EuroSCAR) scoring system serving as a useful diagnostic tool [7]. EuroSCAR score contains the category such as morphology (pustules, erythema, distribution, desquamation postpustulation), course (mucosal involvement, acute onset, resolution, fever, white blood cell count), and histopathology (skin biopsy). A EuroSCAR score of 8 or higher is considered positive and confirms the diagnosis of AGEP [7]. Additional tests such as patch testing, drug-induced lymphocyte stimulation tests (DLSTs), and intradermal testing may be considered as needed [2]. The pathogenesis of AGEP involves multiple immune pathways. Activated CD4+ and CD8+ T-cells respond to specific drug-related triggers, inducing keratinocyte apoptosis and tissue destruction via perforin/granzyme B and Fas ligand pathways, leading to vesicle formation. Additionally, interleukin (IL)-8 or IL-36 secretion promotes neutrophil recruitment, contributing to pustule formation and peripheral neutrophilia [8]. The first-line treatment for AGEP is topical corticosteroid therapy and immediate discontinuation of the causative drug. In severe cases, oral prednisolone is recommended, while supportive therapy with antipyretics and antihistamines can be beneficial. If systemic corticosteroid therapy is ineffective, cyclosporine may be considered as an alternative treatment [2].
Cephalexin is a first-generation cephalosporin beta-lactam antibiotic that exhibits bactericidal activity by inhibiting penicillin-binding proteins [9]. It has strong activity against gram-positive bacteria but limited efficacy against gram-negative bacteria [10]. Adverse effects include dyspepsia, gastritis, diarrhea, abdominal pain, and urticaria, and it is commonly used for the treatment of otitis media and pharyngitis [10,11].
Herein, we report a case of cephalexin-induced AGEP occurring in the context of viral symptoms, while also reviewing previously reported cases.
Case presentation
A 47-year-old male with no significant medical history and no regular medication or supplement use underwent the excision of an epidermal cyst on his back at the Department of Plastic Surgery. Postoperatively, he was prescribed oral cephalexin and topical gentamicin sulfate for the prevention of postoperative infection. Although he had experienced mild upper respiratory symptoms, including cough and nasal discharge, a few days before the procedure, he had no fatigue or fever at that time. On postoperative day 2, while his respiratory symptoms were improving, he developed fatigue, low-grade fever (37.4°C), and a skin eruption, prompting a visit to our Dermatology Department. Physical examination revealed numerous non-follicular pustules with halos on an erythematous base, distributed across the trunk and extremities (Figure 1).
Clinical photograph: Numerous small pustules with erythematous halos were widely distributed across the trunk and extremities, independent of hair follicles.
Despite persistent fatigue, his respiratory symptoms had resolved, and no gastrointestinal symptoms were present. Laboratory examinations revealed elevated white blood cells (11,200/μL; reference range, 4,000-10,000/μL) and C-reactive protein levels (1.39 mg/dL; reference range, 0.00-0.30 mg/dL), while all other biochemical and hematological parameters were within normal ranges. Moreover, viral antibody titers were not tested due to the patient's preference. Histopathological examination of the pustular lesions revealed subcorneal pustules filled with numerous neutrophils. Furthermore, there was marked lymphocytic infiltration into the epidermis at the basal layer, along with liquefactive degeneration. Mild edema in the papillary dermis was observed. Additionally, there was a prominent infiltration of lymphocytes, neutrophils, and eosinophils around the dermal blood vessels (Figures 2-3).
Histopathological examination: Subcorneal pustules were observed, and there was marked infiltration of inflammatory cells in the dermis. Mild edema in the papillary dermis was observed (HE staining; x40).HE: Hematoxylin and eosin
Histopathological examination: A large number of neutrophils were observed within the subcorneal pustules. There was marked lymphocytic infiltration into the epidermis at the basal layer, along with liquefactive degeneration. Additionally, there was prominent infiltration of lymphocytes, neutrophils, and eosinophils around the dermal blood vessels (HE staining; x200).HE: Hematoxylin and eosin
Bacterial cultures of the pustules were negative. The patient’s EuroSCAR score was 9 (Table 1), confirming the diagnosis of AGEP.
Based on the clinical course, cephalexin was identified as the likely causative agent. The patient was treated with topical clobetasol propionate and oral olopatadine, leading to complete resolution of the skin eruption within two weeks. Although patch testing and DLST of the causative drug were recommended to confirm an allergy to cephalexin, the patient declined further testing. No recurrence of skin lesions was observed during a one-month follow-up period, after which both topical and oral treatments were discontinued and follow-up care was completed.
Discussion
To the best of our knowledge, only six cases of AGEP due to the administration of cephalexin have been documented (Table 2) [12-16].
Among these, five cases involved patients with no underlying conditions who developed AGEP rapidly after taking cephalexin for a skin infection. The remaining case involved a patient undergoing treatment for pustular psoriasis who developed AGEP after cephalexin was prescribed for a concurrent skin infection. Both pustular psoriasis and AGEP are characterized by sterile pustules, and their pathogenesis is linked to T helper 17 (Th17) cell activation [17] and the involvement of cytokines such as IL-8 and IL-36 [18]. In their report, Abbas et al. suggested that patients with pustular psoriasis may have an increased susceptibility to the development of AGEP. All six cases were diagnosed with AGEP based on clinical course and histopathological findings; however, our case is the only one in which the EuroSCAR score has been used for definitive diagnosis. The latency period between cephalexin administration and AGEP onset ranged from one to five days, which is consistent with the typical incubation period of AGEP development [1,2]. Notably, none of the six cases underwent drug lymphocyte hypersensitivity testing or patch testing. These allergy tests have a risk of false-positive or false-negative results [1,2], and in cases where the causative drug can be clearly identified based on clinical course, such tests may not be deemed necessary. Regarding treatment, three of the six reported cases received systemic corticosteroids or cyclosporine, while two cases were successfully managed with topical corticosteroids or oral histamines. Although antibiotics are among the most frequently implicated drugs in the trigger of AGEP [1,2], our review found only six documented cases specifically associated with cephalexin [12-16]. However, it is essential to consider the possibility of unpublished cases or instances where multiple drugs were administered, making it difficult to pinpoint the exact causative agent.
In our case, pre-existing cold symptoms prior to the administration of cephalexin may have contributed to the occurrence of AGEP. Infections, including viral infections, have been implicated in AGEP pathogenesis [2-4]. Calistru et al. reported a case of AGEP triggered by amoxicillin in a patient with concurrent parvovirus B19 infection and suggested that viral infection may have played an important role in AGEP onset alongside drug-induced immune responses [19]. Viral infections are known to activate CD4+ and CD8+ T-cells in the body [20]. When a causative drug is administered during an ongoing viral infection, increased infiltration of inflammatory CD4+ and CD8+ T-cells into the skin may lead to enhanced production of inflammatory cytokines such as IL-8 and IL-36, potentially triggering AGEP [2-4,8,20]. In the present case, cephalexin was administered in the presence of viral symptoms, which may have resulted in excessive activation of CD4+ and CD8+ T-cells due to the viral infection, coupled with an immune response to the drug, ultimately leading to AGEP onset. This suggests that in addition to the drug itself, viral infection may have played a contributory role in the development of AGEP in the present case.
Herein, we detailed a case of cephalexin-induced AGEP occurring in the context of viral symptoms and reviewed six previously reported cases. While the EuroSCAR score is a valuable tool for quantitatively confirming AGEP diagnosis, its clinical application remains limited. Greater awareness and broader adoption of the EuroSCAR scoring system are warranted. Furthermore, while AGEP can be triggered by viral infections or interactions between viral infections and causative drugs, its precise mechanisms remain unclear. Therefore, further studies and case accumulations are needed to elucidate these pathophysiological pathways.
Conclusions
AGEP is a severe drug eruption characterized by the sudden onset of numerous small pustules accompanied by edematous erythema. The mainstay of treatment is discontinuation of the causative drug and topical corticosteroids, with rapid resolution typically observed within two weeks. Herein, we presented a case of cephalexin-induced AGEP and reviewed six previously reported cases associated with cephalexin. Since antibiotics are among the most common causative agents of AGEP, careful monitoring of antibiotic administration history is crucial when AGEP is suspected. A limitation of our study is that viral antibody testing was not performed. However, as AGEP developed following symptoms suggestive of a viral infection, a possible association between viral infection and AGEP onset cannot be ruled out. AGEP may be triggered by viral infection alone or by an interaction between viral infection and the causative drug. Therefore, further case accumulation and research are essential to elucidate its underlying mechanisms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute generalized exanthematous pustulosis: European expert consensus for diagnosis and management J Eur Acad Dermatol Venereol Tetart F Walsh S Milpied B 207320813820243902318710.1111/jdv.20232 · doi ↗ · pubmed ↗
- 2Acute generalized exanthematous pustulosis: clinical features, differential diagnosis, and management Am J Clin Dermatol Parisi R Shah H Navarini AA Muehleisen B Ziv M Shear NH Dodiuk-Gad RP 5575752420233715699210.1007/s 40257-023-00779-3PMC 10166469 · doi ↗ · pubmed ↗
- 3Acute generalized exanthematous pustulosis induced by parvovirus B 19 infection Ann Dermatol Lee D Kang JN Hwang SH Lee YS Kim H Seo JK Sung HS 3994002620142496664410.5021/ad.2014.26.3.399PMC 4069655 · doi ↗ · pubmed ↗
- 4COVID-19 vaccine-induced acute generalized exanthematous pustulosis Korean J Intern Med Kang SY Park SY Kim JH Lee SM Lee SP 153715383620213413037210.3904/kjim.2021.198PMC 8588970 · doi ↗ · pubmed ↗
- 5Pustular drug eruptions: a histopathological spectrum Histopathology Burrows NP Russell Jones RR 569573221993835448810.1111/j.1365-2559.1993.tb 00178.x · doi ↗ · pubmed ↗
- 6Acute generalized exanthematous pustulosis Semin Cutan Med Surg Beylot C Doutre MS Beylot-Barry M 244249151996906959210.1016/s 1085-5629(96)80037-x · doi ↗ · pubmed ↗
- 7Acute generalized exanthematous pustulosis (AGEP) - a clinical reaction pattern J Cutan Pathol Sidoroff A Halevy S Bavinck JN Vaillant L Roujeau JC 1131192820011116876110.1034/j.1600-0560.2001.028003113.x · doi ↗ · pubmed ↗
- 8Increased circulating Th 17 frequencies and serum IL-22 levels in patients with acute generalized exanthematous pustulosis J Eur Acad Dermatol Venereol Kabashima R Sugita K Sawada Y Hino R Nakamura M Tokura Y 4854882520112056928210.1111/j.1468-3083.2010.03771.x · doi ↗ · pubmed ↗