New Biomarkers for Patients With Fungal Keratitis From Blood Routine Examination: Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio
Aizhen Wang, Menghe Jin, Zhanpeng Yang, Shuaibing Zhou, Juan Yue, Susu Liu, Yanting Xie, Hongmin Zhang

TL;DR
This study shows that blood tests measuring NLR and PLR can help detect and monitor fungal eye infections, especially in areas with limited medical resources.
Contribution
The study introduces NLR and PLR as novel, accessible biomarkers for diagnosing and predicting outcomes in fungal keratitis.
Findings
NLR and PLR were significantly higher in fungal keratitis patients compared to controls.
NLR strongly correlated with inflammation severity, more so than PLR.
Higher NLR and PLR values were linked to worse treatment outcomes in FK patients.
Abstract
Purpose: To assess the potential of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as novel diagnostic and prognostic biomarkers in fungal keratitis (FK). Methods: This study was carried out retrospectively in 77 FK patients and 77 matched cataract controls from Henan Eye Hospital. Peripheral venous blood samples were collected via venipuncture and analyzed using complete blood count for routine clinical evaluation. FK patients were classified into three subgroups: Fusarium, Aspergillus, and Candida groups. Inflammation severity was quantified using standardized clinical scoring. The treatment modalities were used to divide the FK patients into enucleation and nonenucleation groups. Results: NLR and PLR were significantly elevated in FK versus controls (p < 0.001). NLR correlated strongly with inflammation scores (r = 0.535, p < 0.0001), exceeding PLR's…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
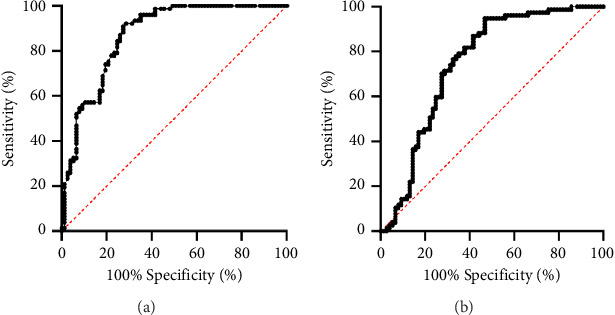 Figure 1
Figure 1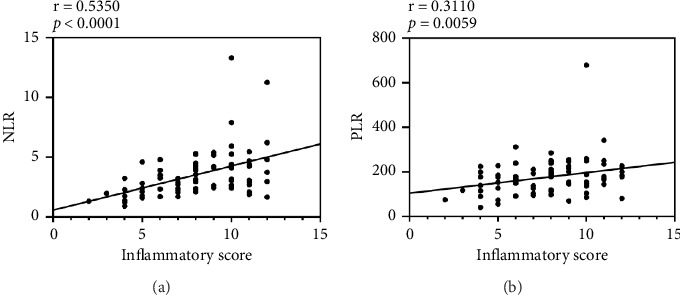 Figure 2
Figure 2- —Natural Science Foundation of Henan Province
- —Henan Eye Hospital Key Program of Basic Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Surface and Contact Lens · Corneal surgery and disorders
1. Introduction
Fungal keratitis (FK) remains a leading cause of corneal blindness in agricultural regions, with Fusarium, Aspergillus, and Candida species accounting for over 80% of culture-proven cases globally [1, 2]. Despite advancements in diagnostic tools such as direct microscopy, corneal scraping, culture, confocal microscopy, and PCR, significant limitations persist in resource-limited rural settings in terms of availability, timeliness, sensitivity, and specificity [3]. As a result, improper diagnosis or delayed treatment is common, which can lead to irreversible complications such as endophthalmitis and even enucleation if not addressed promptly. The diagnostic dilemma is similarly exacerbated by FK's deceptive clinical trajectory (slow onset and subtle symptoms). Without early detection and suitable treatment approaches, the condition becomes debilitating and refractory in its later stages [4]. This diagnostic bottleneck creates urgent demand for rapid, affordable biomarkers that complement existing methods.
Recent studies have explored the use of blood-derived inflammatory biomarkers, particularly the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), which have shown promise as indicators of various inflammatory and systemic conditions [5–10]. Emerging evidence positions NLR and PLR as potential diagnostic adjuncts across ocular disorders. Moreover, NLR and PLR levels have also been linked to heightened inflammatory activity, disease severity, and poor prognosis [11–16]. However, the role of NLR and PLR in FK remains underexplored.
This study aims to investigate the potential association between FK and NLR/PLR. By evaluating their levels in FK patients, we seek to understand whether these biomarkers could serve as early indicators for diagnosing FK and predicting its progression, offering a simple, cost-effective tool for stratified FK management in resource-limited settings. Ultimately, this could improve the prognosis and treatment outcomes for FK patients by enabling timely intervention.
2. Material and Method
2.1. Study Design and Patients
The research was designed as a retrospective observational study, with inherent limitations including selection bias and confounding factors from single-center sampling. The study was approved by the Institutional Review Board (IRB) of Henan Eye Hospital (approval number HNEEC-202419) and adhered to the ethical guidelines of the Declaration of Helsinki. Informed consent was obtained from all included participants.
This study analyzed the medical records of 255 FK patients admitted to Henan Eye Hospital from January 1, 2019, to December 31, 2023. Initially, patients diagnosed with FK based on WHO diagnostic criteria were included, while a control group was selected from patients receiving preoperative screening in the cataract department. General demographic data, such as age, sex, and body mass index (BMI), were collected.
Exclusion criteria included age under 18 years, presence of autoimmune or inflammatory systemic or ocular diseases (except for FK), ocular surgery or trauma within the past 12 months, permanent traumatic eye injury, use of medications that affect blood counts (except for antifungal drugs used in FK treatment), history of malignancy or hematological disorders, pregnancy, and habitual smoking. In addition, patients with incomplete medical records or who did not consent to participate were excluded.
Following the eligibility review, 77 FK patients were included in the study. The control group comprised 77 age- and gender-matched cataract patients without other comorbidities.
2.2. Clinical Evaluation
From the medical records, various data were collected, including anterior segment photos, fungal culture results, slit-lamp inspection images, and details of the treatment procedures. Following fungal culture-based identification, in which corneal scrapings were inoculated onto Sabouraud dextrose agar (SDA) using a C-shaped streaking method, FK patients were classified into three etiological subgroups: Fusarium, Aspergillus, and Candida [17]. Inflammation levels in the patients were visually scored using anterior segment photos and slit-lamp inspection images (the two methods complemented each other; in case of any conflict, the slit-lamp results took precedence). The inflammation scoring system, which evaluated area of opacity, opacity density, and surface regularity, was specifically performed by one experienced clinician to ensure consistent and accurate evaluations across multiple time points [18]. Each criterion was graded on a scale from 0 to 4, with higher scores indicating greater severity. In cases where empyema and/or hypopyon were present in the anterior chamber, an additional point was added to the score for that eye. A completely clear, nonscarring cornea received a score of 0 in each category. The final inflammation score for each eye was the sum of the scores across all three categories. More detailed scoring criteria are shown in Table 1. The treatment modalities were used to divide the FK patients into enucleation and nonenucleation groups. Such therapies as pharmacotherapy, penetrating keratoplasty (PK), and anterior lamellar keratoplasty (DALK) were included in the group of nonenucleation.
2.3. Blood Sampling
For all participants, 3–5 mL venous blood samples were collected from the antecubital vein in the early morning and mixed with an anticoagulant (EDTA). Complete blood count (CBC) measurements were performed within 2 h using an automated blood cell analyzer (XN9100; Sysmex, Kobe, Japan). The parameters of neutrophil, platelet, and lymphocyte were recorded. The NLR and PLR were calculated by determining the ratio of neutrophils to lymphocytes and platelets to lymphocytes, respectively. The selection of thresholds was determined by maximizing the Youden Index, prioritizing the balance between sensitivity and specificity to ensure optimal diagnostic performance.
2.4. Statistical Analysis
The normality of each continuous variable was tested using the Kolmogorov–Smirnov normality test. Continuous variables with a normal distribution were expressed as means ± standard deviations, while continuous variables without a normal distribution were expressed as medians and interquartile ranges. An independent t-test, Mann–Whitney U test, or chi-square test were used to compare continuous and categorical variables between two groups. For multiple groups, the Kruskal–Wallis test was applied to compare parameters across all groups. Spearman correlation was used to analyze the correlations between inflammatory degree and NLR or PLR. The area under the receiver operating characteristic (ROC) curve (AUC), specificity, sensitivity, and cutoff values were used to determine the accuracy of the NLR and PLR for distinguishing between FK and NFK. Statistical significance was set at p < 0.05. The statistical analysis was conducted using the Statistical Package for Social Science 27.0 software (SPSS, Chicago, IL, USA).
3. Results
3.1. Patient Characteristics
The mean age was 59.43 ± 8.73 years old (range: 35–76) in the FK group and 59.51 ± 8.54 years old (range: 37–75) in the control group (p=0.956). The mean BMI was 23.99 ± 3.13 in the FK group and 24.97 ± 3.66 in the control group. Males comprised 44% of both the FK and control groups (p=1). There were no significant differences between the groups in terms of age, BMI, and gender distribution (p=0.956, p=1, and p=0.076, respectively).
3.2. Parameters of the Blood Test
Regarding hematological parameters, neutrophil counts, platelet counts, NLR, and PLR (for all p < 0.001) were significantly higher in FK patients compared with control groups. The statistically lower value was observed only in the case of lymphocyte counts (p=0.001) between the study and control groups. Comparable of the control and patient groups are summarized in Table 2. The ROC analysis of the evaluated factors is graphically presented in Figure 1. According to the figure, the NLR AUC value that was used to discriminate subjects in the FK and control groups was 0.871. When the best cutoff value was identified as 2.35, sensitivity and specificity values were found to be 71.4% and 92.0%, respectively. The PLR AUC value that was used to discriminate subjects in the FK and control group was 0.749. When the best cutoff value was identified as 176, sensitivity and specificity values were found to be 53.2% and 94.7%, respectively.
Analysis using Kruskal–Wallis H revealed that the median value of NLR was 3.14 in the Fusarium group, 2.89 in the Aspergillus group, and 2.30 in the Candida group. The median value of PLR was 124.23 in the Fusarium group, 177.69 in the Aspergillus group, and 140.88 in the Candida group. There were no statistically significant differences in NLR (p=0.534) and PLR (p=0.476) noticed among the subgroups (Table 3).
To investigate the correlation of clinical scoring on CBC-derived inflammatory markers in FK patients, a correlation between inflammation scores and hematological parameters was performed. Spearman correlation analysis in Figure 2 suggested there was a positive relationship between inflammatory scores and NLR (r = 0.535, p < 0.0001) and PLR (r = 0.311, p=0.0059).
In two different treatment groups, the median value of NLR value was 3.07 in the enucleation group and 1.98 in the nonenucleation group. The median value of PLR was 179.14 in the enucleation group and 139.07 in the nonenucleation group. The intergroup differences in the median value of NLR and PLR turned out to be statistically significant between the groups (p=0.012 and p=0.021, respectively). Also, higher NLR and PLR values were observed in the enucleation group (Table 4).
4. Discussion
FK represents a severe corneal suppurative inflammation governed by dynamic interactions between fungal virulence and host inflammatory responses. While fungal invasion initiates tissue damage, accumulating evidence suggests that excessive neutrophil activation constitutes a critical driver of terminal-stage corneal opacification and vision loss. Neutrophils, activated by pathogen recognition receptors, release proinflammatory cytokines, neutrophil extracellular traps (NETs), and tissue-damaging molecules such as reactive oxygen species (ROS), which exacerbate inflammation and aid in fungal clearance. However, excessive neutrophil activation can lead to uncontrolled inflammation, further contributing to corneal scarring and depriving patients of the opportunity for corneal transplantation surgery [19–22]. Platelets, traditionally known for their role in hemostasis, are increasingly recognized for their involvement in immunity and inflammation. They possess a dual nature in immune responses, capable of both enhancing inflammatory responses and modulating their strength and temporal dynamics [23]. Moreover, the decrease in lymphocytes, indicative of depressed cell-mediated immunity, has been extensively addressed [24]. Elevated NLR/PLR typically indicates excessive activation of neutrophils and platelets and a relative reduction in lymphocytes, reflecting an exacerbation of the inflammatory response and a disruption of immune balance.
Our study identified NLR (> 2.35) and PLR (> 176) as diagnostic markers for FK, with both parameters significantly elevated compared with controls (p < 0.001). While NLR/PLR have demonstrated utility in systemic infections [9, 25], this study provides the first validation in corneal infections, addressing a critical gap in ocular immunology. The NLR threshold, while lower than those in systemic chronic conditions (e.g., COPD NLR > 3.4–16.8; hypertrophic cardiomyopathy NLR > 3.43), aligns with acute ocular pathologies such as retinal artery occlusion (NLR > 1.62) and high myopia (NLR > 2.68) [12, 14, 26, 27]. The blood-eye barrier likely attenuates peripheral immune cell infiltration, reducing systemic biomarker sensitivity compared with nonocular infections. In contrast to chronic systemic inflammation, acute corneal infections may induce different hematopoietic dynamics. Notably, the observed NLR dichotomy—higher than noninflammatory ocular conditions but lower than uveitis (NLR > 5.608)—may result from the former is an intraocular inflammation, whereas FK affects the cornea, leading to differential impacts on the blood-ocular barrier [13]. However, the PLR threshold was found to be elevated relative to other ocular diseases in the current study, though the precise mechanistic drivers of this divergence remain to be fully elucidated. Moreover, even for the same disease, NLR/PLR thresholds vary substantially across different studies [16]. Although a precise cutoff value has not been found yet, its role as a flag of immune system homeostasis was well established.
The prognostic utility of NLR/PLR was reinforced by their significant correlations with both inflammatory severity and surgical outcomes. Mirroring findings in open globe injuries [15] and dry eye disease [28], our data demonstrate these biomarkers' potential for predicting FK progression, with elevated levels indicating higher enucleation risk. Consistent with the previous results, NLR apparently outperformed PLR in diagnostic accuracy and prognostic value, possibly reflecting neutrophils' central role in fungal defense versus platelets' secondary mediator functions. Importantly, both markers showed limited discriminatory capacity for specific fungal species. This observation may indicate either conserved inflammatory responses across pathogens or insufficient statistical power in subgroup analyses due to sample size constraints.
In primary hospitals or resource-limited areas, routine blood tests are easily accessible. While conventional methods like corneal scraping cultures are time-consuming and delay diagnosis, NLR and PLR may provide a rapid alternative as early warning indicators in the absence of efficient etiological tools. Dynamic monitoring of NLR and PLR may help gain valuable insights into the disease's inflammatory status, enabling prompt intervention. In addition, these markers can be used to identify patients who are at high risk for poor outcomes, such as severe tissue damage or the need for surgical interventions like enucleation. Their ability to guide personalized treatment strategies could significantly improve patient prognosis and reduce the long-term impact of FK. The “systemic-to-local” research approach offers new perspectives for the diagnosis and treatment of infectious eye diseases.
Our study also had several limitations. Its retrospective, single-center design and the small number of patients included risked selection bias. Second, single-timepoint measurements preclude tracking dynamic biomarker changes. Third, a huge difference in the disease course may have also affected these risk factors. Lastly, elderly skewed cohort may not generalize to younger populations. Therefore, more stable results would be expected to be gained adequately by clinical trials with larger sample sizes, in which data can be analyzed prospectively.
In conclusion, NLR and PLR might be valuable supplementary indicators for not only early detection but also for monitoring disease progression and tailoring therapeutic approaches in clinical practice. Further research is required to validate these findings and establish their clinical applicability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoffman J. J. Burton M. J. Leck A. Mycotic Keratitis-A Global Threat From the Filamentous Fungi Journal of Fungi 202174 p. 27310.3390/jof 704027333916767 PMC 8066744 · doi ↗ · pubmed ↗
- 2Donovan C. Arenas E. Ayyala R. S. Margo C. E. Espana E. M. Fungal Keratitis: Mechanisms of Infection and Management Strategies Survey of Ophthalmology 202267375876910.1016/j.survophthal.2021.08.00234425126 PMC 9206537 · doi ↗ · pubmed ↗
- 3Brown L. Leck A. K. Gichangi M. Burton M. J. Denning D. W. The Global Incidence and Diagnosis of Fungal Keratitis The Lancet Infectious Diseases 2021213 e 49e 5710.1016/s 1473-3099(20)30448-533645500 · doi ↗ · pubmed ↗
- 4Toumasis P. Tsantes A. G. Tsiogka A. Samonis G. Vrioni G. From Clinical Suspicion to Diagnosis: A Review of Diagnostic Approaches and Challenges in Fungal Keratitis Journal of Clinical Medicine 2024131 p. 28610.3390/jcm 13010286 PMC 1077956038202293 · doi ↗ · pubmed ↗
- 5Heshmat-Ghahdarijani K. Sarmadi V. Heidari A. Falahati Marvasti A. Neshat S. Raeisi S. The Neutrophil-To-Lymphocyte Ratio as a New Prognostic Factor in Cancers: A Narrative Review Frontiers in Oncology 202313 p. 122807610.3389/fonc.2023.1228076 PMC 1058354837860198 · doi ↗ · pubmed ↗
- 6Gasparyan A. Y. Ayvazyan L. Mukanova U. Yessirkepov M. Kitas G. D. The Platelet-To-Lymphocyte Ratio as an Inflammatory Marker in Rheumatic Diseases Ann Lab Med 201939434535710.3343/alm.2019.39.4.3452-s 2.0-8506228654130809980 PMC 6400713 · doi ↗ · pubmed ↗
- 7Ou Y. Liang S. Gao Q. Prognostic Value of Inflammatory Markers NLR, PLR, LMR, d NLR, ANC in Melanoma Patients Treated With Immune Checkpoint Inhibitors: A Meta-Analysis and Systematic Review Frontiers in Immunology 202415 p. 148274610.3389/fimmu.2024.148274639493767 PMC 11527641 · doi ↗ · pubmed ↗
- 8Zinellu A. Zinellu E. Mangoni A. A. Clinical Significance of the Neutrophil-To-Lymphocyte Ratio and Platelet-To-Lymphocyte Ratio in Acute Exacerbations of COPD: Present and Future European Respiratory Review 202231166 p. 22009510.1183/16000617.0095-2022 PMC 972488036323421 · doi ↗ · pubmed ↗