Refractory Hypokalemia of Pregnancy: A Rare Case of Non-Aldosterone Mediated Hypokalemia
Deekshita Valiveti, Olivia Lahey, Karim Nooruddin, Brandi Addison

TL;DR
A rare case of hypokalemia during pregnancy is described, linked to a genetic condition called Geller syndrome.
Contribution
This report highlights a rare genetic cause of refractory hypokalemia during pregnancy.
Findings
Geller syndrome is a genetic mutation causing non-aldosterone mediated hypokalemia and hypertension during pregnancy.
Hypertension and hypokalemia resolve after delivery of the fetus.
Genetic testing is essential for diagnosing Geller syndrome.
Abstract
There is a wide differential for a patient presenting with hypokalemia and hypertension in pregnancy. Of these, Geller syndrome is a rare variant of mineralocorticoid receptor that leads to concomitant hypokalemia and gestational hypertension. Progesterone has been shown to have a high affinity for the mineralocorticoid receptor and thus antagonizes aldosterone functioning. However, in Geller syndrome, there is a mutation of the mineralocorticoid receptor with a resultant gain of function. Activation of the mutated receptor is characterized by hypertension and hypokalemia, which is exacerbated by the effect of progesterone and thereby presenting during pregnancy. Genetic testing can confirm the diagnosis of Geller syndrome. The management is supportive therapy and requires close monitoring of the patient and her fetus. Delivery of the fetus results in the resolution of both hypertension…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
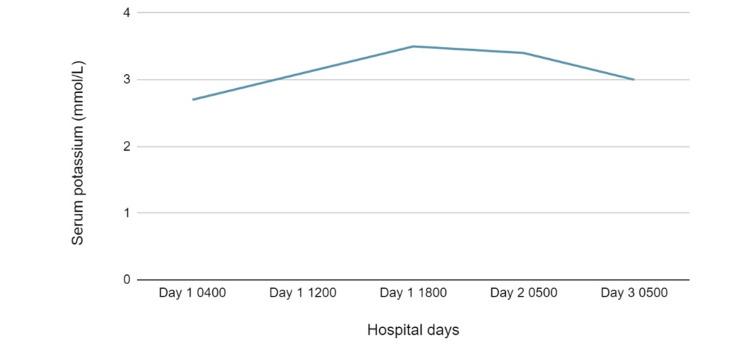 Figure 1
Figure 1| Test | Result | Reference value | ||
| Urine creatinine | 31.59 mg/dL | No established reference range | ||
| Urine chloride | 119 mmol/L | |||
| Urine potassium | 22 mmol/L | |||
| Urine sodium | 102 mmol/L | |||
| 24-hour urine protein | 320 mg/24 hours | 0-165 mg/24 hours | ||
| Renin | 2.707 ng/mL/hour | 0.167-5.380 ng/mL/hour | ||
| Aldosterone | <1.0 ng/dL | 0.0-30.0 ng/dL | ||
| Repeat renin | 0.757 ng/mL/hour | 0.167-5.380 ng/mL/hour | ||
| Repeat aldosterone | <1.0 ng/dL | 0.0-30.0 ng/dL | ||
| Sodium | 139 mmol/L | 133-145 mmol/L | ||
| Potassium | 2.7 mmol/L | 3.6-5.2 mmol/L | ||
| Chloride | 106 mmol/L | 100-108 mmol/L | ||
| Carbon dioxide | 25 mmol/L | 22-32 mmol/L | ||
| Glucose | 73 mg/dL | 65-99 mg/dL | ||
| Blood urea nitrogen | 4 mg/dL | 6-20 mg/dL | ||
| Creatinine | 0.64 mg/dL | 0.60-1.00 mg/dL | ||
| Glomerular filtration rate | 126 mL/min | 71-165 mL/min | ||
| Total protein | 5.6 g/dL | 6.4-8.2 g/dL | ||
| Albumin | 2.1 g/dL | 3.4-5.0 g/dL | ||
| Globulin | 3.5 g/dL | 1.5-3.8 g/dL | ||
| Calcium | 7.8 mg/dL | 8.7-10.5 mg/dL | ||
| Total bilirubin | 0.1 mg/dL | 0.0-1.0 mg/dL | ||
| Aspartate aminotransferase (AST) | 28 units/L | 15-37 units/L | ||
| Alanine aminotransferase (ALT) | 12 units/L | 30-65 units/L | ||
| Alkaline phosphatase (ALP) | 140 units/L | 50-136 units/L | ||
| Magnesium | 1.9 mg/dL | 1.8-2.4 mg/dL | ||
| Hospital day and time | Potassium administered |
| Day 1 0600 | Oral KCl 30 mEq |
| Day 1 0700 | Intravenous D5W + KCl @ 100 cc/hour |
| Day 1 1200 | Intravenous D5-LR + KCl @ 125 cc/hour |
| Day 1 1200 | Oral KCl 30 mEq |
| Day 1 1700 | Oral 30 mEq |
| Day 1 2100 | Intravenous D5-LR + KCl @ 125 cc/hour |
| Day 2 0800 | Oral KCl 30 mEq |
| Day 2 1200 | Oral KCl 30 mEq |
| Day 2 1800 | Oral KCl 30 mEq |
| Day 3 0800 | Oral KCl 30 mEq |
| Day 3 1300 | Oral KCl 40 mEq |
| Day 3 1700 | Oral KCl 40 mEq |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Electrolyte and hormonal disorders · Thyroid Disorders and Treatments
Introduction
Hypokalemia has a variety of etiologies including loss through the gastrointestinal system, renal excretion, intracellular shift, and rarely decreased intake. Hypokalemia in pregnancy can be seen in Geller syndrome, a rare variant of mineralocorticoid receptor that leads to concomitant hypokalemia and gestational hypertension [1].
Since being first described by Geller et al. in 2000 [1], there have been roughly 10 reported cases [2-10]. Genetic testing confirms the diagnosis of Geller syndrome. The management is supportive therapy and requires close monitoring of the patient and her fetus. Delivery of the fetus results in the resolution of both hypertension and hypokalemia [1].
This case report of a 25-year-old pregnant woman with refractory hypokalemia emphasizes the importance of swift and accurate diagnosis and treatment.
Case presentation
A 25-year-old female patient, G4 P0120 (23rd-week perinatal death), presented at 29 weeks gestation for consultation regarding severe hypokalemia with paresthesias, pedal edema, lethargy, and generalized weakness.
The patient recalled that she has had issues with low potassium during the current and prior pregnancies. In previous pregnancies, she required oral potassium (which she was unable to tolerate) and thus necessitated frequent infusions of potassium in the emergency room. Once the patient was postpartum, she was able to maintain her serum potassium levels with dietary management. During the current pregnancy, her prenatal course was rather uncomplicated with the exception of nausea and vomiting (one to two episodes daily). She also endorsed palpitations. The patient denied any worsening gastrointestinal symptoms such as increased vomiting or diarrhea that could explain the persistent hypokalemia. She also denied any recent febrile illness. Also during the current pregnancy, she presented to the emergency department on seven separate occasions for elevated blood pressure and was noted to have low potassium levels requiring intravenous (IV) supplementation. Aside from hypokalemia, her remaining outpatient laboratory testing and sonograms were unremarkable. Her home medications included: albuterol, fluticasone propionate/salmeterol, gabapentin, and prenatal vitamins. She specifically denied taking over-the-counter medications, IV or recreational drug use, and tobacco or alcohol use.
Vital signs on admission showed blood pressure 112/56 mmHg, heart rate 87 beats/minute, respiratory 17 breaths/minute, oxygen saturation (SpO2) 95% on room air, temperature 97.9 F. Physical examination was notable for trace pedal edema and gravid uterus consistent with 29 weeks gestation. On laboratory evaluation, she was found to have significant hypokalemia of 2.7 mEq/L and was admitted to the inpatient antepartum unit for further workup and treatment. Labs on admission can be found in Table 1.
After being started on vigorous IV potassium supplementation, her symptoms largely resolved and intermittent palpitations dissipated. A review of her records revealed that her fractional excretion of urinary potassium was 12.6% in the presence of hypokalemia and replacement of potassium at 90 mEq/day. This indicates potassium wasting by the kidneys. Her magnesium level was 1.5 mg/dL which was repleted daily. The patient was not known to have any history of renal dysfunction. Nephrology was thus consulted and believed that there could be an association with pregnancy-induced hypokalemia.
Further workup revealed normal thyroid-stimulating hormone (TSH) and cortisol levels, with a renin level of 0.757 ng/mL/hour (normal range: 0.167-5.380 ng/mL/hour) and suppressed aldosterone level (below 1 ng/dL) (Table 2). Given the fractional excretion of potassium at 12.6% and simultaneous suppression of aldosterone, this incongruence implies renal potassium wasting [2-5,11].
Geller syndrome is a rare disease that manifests during pregnancy and causes clinical findings of severe hypokalemia and gestational hypertension. Normalization of blood pressure and potassium following delivery strongly suggests Geller syndrome. The diagnosis is further supported by low serum aldosterone and plasma renin in addition to hypokalemia despite an elevated urinary potassium-creatinine ratio. The presence of hypertension in addition to hypokalemia, despite renal-potassium wasting, implies a hyperaldosteronism-like state. However, suppressed serum aldosterone indicates the diagnosis of an activating mineralocorticoid receptor mutation [4]. Diagnosis is suggested by clinical findings and can be confirmed with genetic testing [1].
Our patient's findings of recurrent pregnancy with severe hypokalemia, gestational hypertension, suppressed renin and aldosterone, and elevated urine potassium-creatinine ratio support the diagnosis of Geller syndrome. Following aggressive intravenous potassium supplementation (Figure 1), the patient clinically improved and she was discharged home with oral potassium chloride 40 mEq three times daily and magnesium oxide 400 mg twice daily. Note that there was a discussion on whether or not to initiate amiloride; however, the patient was planning to travel cross-country to return home and, as close follow-up was undetermined, she was strongly advised to discuss initiation of amiloride with her maternal-fetal medicine physician once she returned home.
Serum potassium trend during hospitalization
Discussion
The differential diagnosis of a patient presenting with hypokalemia is broad, including genetic conditions such as congenital adrenal hyperplasia (CAH), acquired conditions such as mineralocorticoid excess, decreased potassium intake, or increased potassium losses. Liddle syndrome was also a consideration in this patient; however, we would have expected to see early-onset hypertension and hypokalemia. Moreover, refractory hypokalemia can be seen in Gitelman and Bartter syndrome; however, normal or low blood pressure with elevated renin and aldosterone levels is expected in patients who are diagnosed with these syndromes [6,12,13]. Although our patient exhibited a lack of hypertension on this admission, she did note mild gestational hypertension in previous pregnancies.
More recently, other etiologies for hypokalemia have been studied. Notably, Geller et al., in 2000, identified pregnant individuals presenting with gestational hypertension and hypokalemia [1]. The proposed mechanism is caused by an agonist effect of the excessive production of progesterone and its action on a mutated mineralocorticoid receptor, leading to severe hypokalemia and gestational hypertension [1,6]. As seen in our patient, renin and aldosterone levels are usually suppressed in this syndrome[2-5,11]. Genetic testing remains the gold standard for confirmation of the diagnosis [2]. However, due to limitations, this was not performed in our patient for confirmation of the presumed Geller syndrome diagnosis.
Treatment is generally supportive and focuses on managing complications of gestational hypertension and hypokalemia which usually resolve after delivery [14]. The current literature suggests that some patients have responded well to amiloride, while spironolactone has been noted to worsen blood pressure by activating the mutated mineralocorticoid receptor, therefore contraindicated in Geller syndrome and also in pregnancy [15].
Conclusions
Given the novelty and rarity of the condition, both the early recognition and awareness of Geller syndrome are crucial to avoid complications for the patient and fetus from hypokalemia and hypertension. Clinicians should be vigilant when evaluating recurrent hypokalemia of pregnancy. Early identification and management can mitigate hospitalizations for severe hypokalemia and the development of periodic paralysis. Clinicians should also focus on patient education regarding high chances of recurrence during future pregnancies. Finally, consistent follow-up for monitoring serum potassium levels in addition to blood pressure is necessary for the treatment of Geller syndrome and other syndromes of apparent mineralocorticoid excess. Although benefit from amiloride has been suggested, future studies can focus on its role in treatment and explore potential teratogenic effects.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Activating mineralocorticoid receptor mutation in hypertension exacerbated by pregnancy Science Geller DS Farhi A Pinkerton N 11912328920001088422610.1126/science.289.5476.119 · doi ↗ · pubmed ↗
- 2Geller syndrome: a rare cause of persistent hypokalemia during pregnancy Cureus Hindosh N Hindosh R Dada B Bal S 0142022 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 9308893/10.7759/cureus.26272 PMC 930889335898361 · doi ↗ · pubmed ↗
- 3American Society of Nephrology: Geller syndrome: two cases of hypertension and hypokalemia in pregnancy Am Soc Nephrol 4 2024 Mulkanoor Mulkanoor Vinay Vinay Maynard Maynard Sharon E 6252017 https://www.asn-online.org/education/kidneyweek/2017/program-abstract.aspx?control Id=2788811
- 4Pregnancy complicated by hypertension and hypokalemia Am J Kidney Dis Garg AK Parajuli P Mamillapalli CK 0276202010.1053/j.ajkd.2020.04.01232972567 · doi ↗ · pubmed ↗
- 5A Case Report of Recurrent Hypokalemia During Pregnancies Associated With Nonaldosterone-Mediated Renal Potassium Loss Can J Kidney Health Dis Pintavorn P Munie S 20543581211017424820213410445510.1177/20543581211017424 PMC 8165817 · doi ↗ · pubmed ↗
- 6American Society of Nephrology:Hypokalemic periodic paralysis and hypertension in pregnancy: a diagnostic challenge Am Soc Nephrol 4 2024 Yalamarti T Ntoso KA Patrascu C Zonoozi S Barry T 3782019 https://www.asn-online.org/education/kidneyweek/2019/program-abstract.aspx?control Id=3230404
- 7#4180 hypertension, hypokalemia and pregnancy: a case of geller syndrome Nephrol Dialysis Transplant Sarwal A Abraham J 012023
- 8WCN 23-1210 first reported case of Geller syndrome outside North America Kidney Int Rep Bin Rhasbudin Shah SS Crawford V Williams L Gupta A 082022