A case of hemodiafiltration dialysis preventing progression of acute kidney injury in a patient with hypermyoglobinemia in one kidney: a case report
Toru Minamiyama, Shozo Yoshida, Yosuke Mizuno, Hiroki Kitagaki, Kaori Kimura, Yoshihito Naito, Akihiro Uchida, Ayumi Kuroda, Yuki Kawasaki, Ayane Nishio, Hirotsugu Fukuda, Genki Yoshimura, Ryo Kamidani, Takahito Miyake, Norihide Kanda, Hideshi Okada

TL;DR
This case report shows how early dialysis helped prevent kidney failure in a patient with severe muscle breakdown.
Contribution
Demonstrates the effectiveness of early hemodiafiltration in preventing acute kidney injury due to hypermyoglobinemia.
Findings
Early hemodiafiltration prevented acute kidney injury despite high myoglobin levels.
The patient's kidney function remained stable with normal creatinine levels.
Intermittent hemodiafiltration may be a viable intervention for rhabdomyolysis-induced kidney injury.
Abstract
Rhabdomyolysis is a clinical syndrome resulting from skeletal muscle damage and the release of its breakdown products into the bloodstream. It can range from asymptomatic cases to severe conditions such as acute kidney injury. Although the release of myoglobin (molecular weight 17.2 kDa) into the blood is associated with the progression to acute kidney injury, there is no established method to prevent it. Here, we report a case of hypermyoglobinemia due to rhabdomyolysis caused by reperfusion injury following acute limb ischemia, where early renal replacement therapy was deemed effective. The patient, a 73-year-old Japanese male, had a history of right nephrectomy due to trauma. At 2 years prior, he underwent bypass surgery connecting the subclavian artery to the bilateral femoral arteries to treat lower limb arteriosclerotic occlusive disease. In this case, he presented to another…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
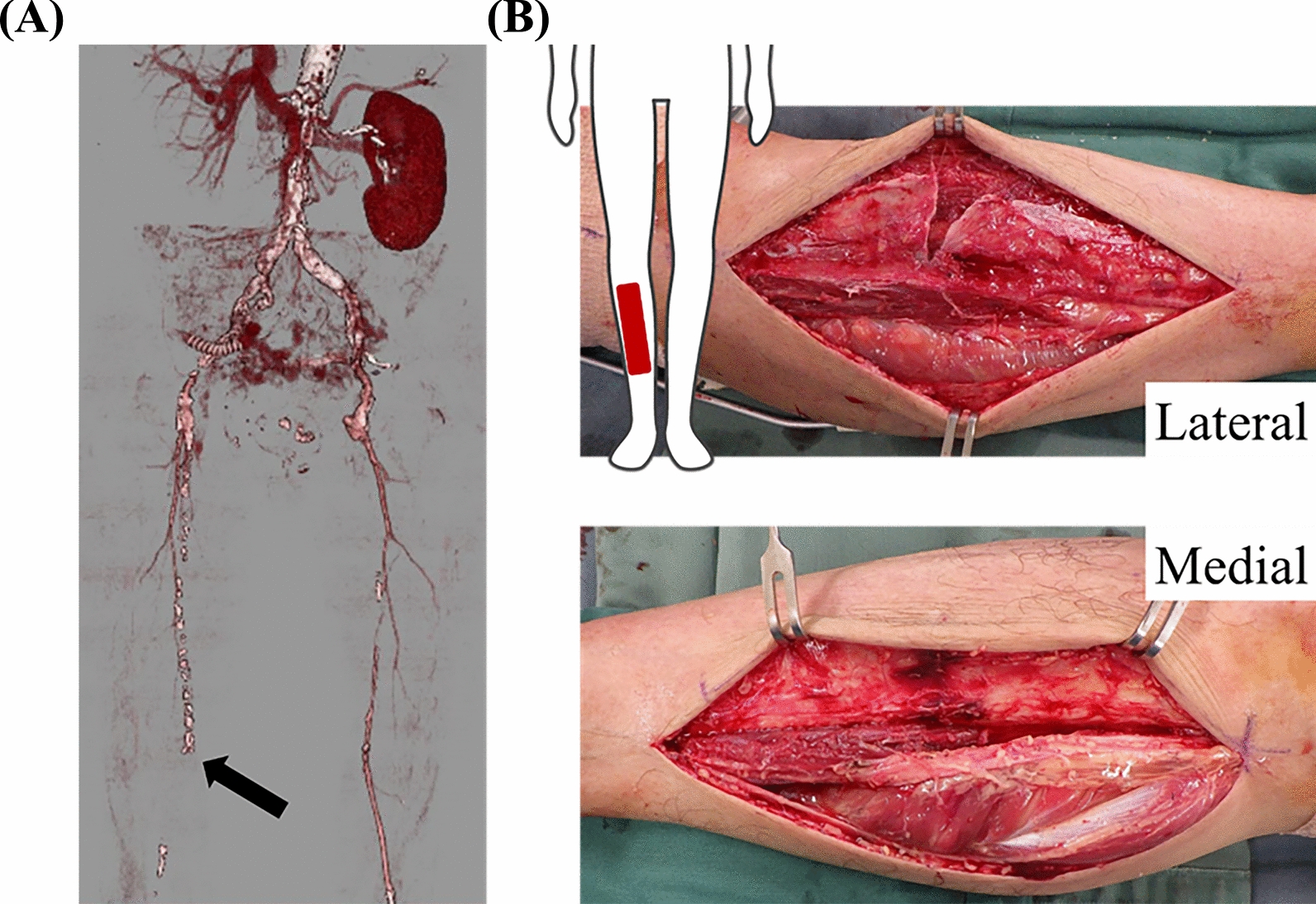 Figure 1
Figure 1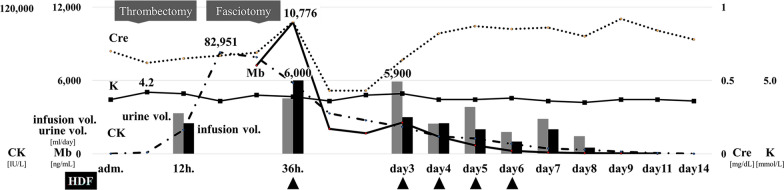 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMuscle and Compartmental Disorders · Dialysis and Renal Disease Management · Electrolyte and hormonal disorders
Background
Rhabdomyolysis is a clinical syndrome caused by skeletal muscle damage and the release of its breakdown products into the circulation, ranging from asymptomatic to severe cases, such as acute kidney injury (AKI) [1]. The release of myoglobin (Mb; molecular weight: 17.2 kDa) into the blood is involved in the development of AKI. Although renal replacement therapy (RRT) is not the first choice for AKI prevention, the removal of myoglobin and other inflammatory substances and early intervention may reduce its risk [2–5]. In the present study, we report a case of hypermyoglobinemia owing to rhabdomyolysis caused by reperfusion injury after acute limb ischemia that responded to early RRT.
Case presentation
The patient was a 73-year-old Japanese man who previously underwent surgery for primary lung cancer and was receiving anticancer drugs. He had a history of right nephrectomy following trauma. Additionally, two years prior, he had bypass surgery connecting the subclavian artery to the bilateral femoral arteries to treat lower limb arteriosclerotic occlusive disease. In this case, he initially presented at another hospital with sudden right lower limb pain and was subsequently referred to our hospital, where he was diagnosed with acute occlusion of the right lower extremity artery. Upon arrival at our hospital, his Glasgow Coma Score (GCS) was 15 points (GCS E4V5M6). The patient’s vital signs were as follows: blood pressure, 194/73 mmHg; heart rate, 107 beats/minute; respiratory rate, 21 breaths/minute; SpO_2_, 98% (room air); and temperature, 36.2℃. In the right lower extremity, blood pressure and SpO_2_ were unmeasurable, and the skin was pale with spontaneous pain. Arterial blood gas and laboratory test results are shown in Table 1.Table 1. Laboratory findings at the time of admissionBiochemistryComplete blood countTotal protein6.9g/dLWhite blood cells12,470/µLAlbumin4.5g/dLRed blood cells3.99 × 10^6^/µLCreatinine kinase125IU/LHemoglobin14.1g/dLAST35IU/LHematocrit40.7%ALT13IU/LPlatelet178 × 10^3^/µLLDH254IU/Lγ-GTP38IU/LCoagulation statusAmylase90IU/LAPTT20.7secTotal bilirubin0.8mg/dLPT-INR0.79Direct bilirubin0.2mg/dLFibrinogen241mg/dLCreatinine0.70mg/dLFDP131.9µg/mLBUN10.9mg/dLD-dimer29.4µg/mLSodium136mEq/LPotassium3.7mEq/LArterial Blood GasChloride100mEq/LF_I_O_2_0.40Magnesium1.7mg/dLpH7.348Calcium9.3mg/dLP_a_CO_2_42.4mmHgGlucose202mg/dLP_a_O_2_199.0mmHgHbA1c5.5%HCO_3_^−^23.3mmol/LCRP0.03mg/dLBase excess−2.3Lactate4.9mmol/LAnion gap12.6AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH, lactic acid dehydrogenase; γ-GTP, γ-glutamyl transpeptidase; BUN, blood urea nitrogen; HbA1c, hemoglobin A1c; CRP, C-reactive protein; APTT, activated partial thromboplastin time; PT-INR, prothrombin time-international normalized ratio; FDP, fibrin degradation product; F_I_O_2_, fraction of inspiratory oxygen
Contrast-enhanced computed tomography revealed an occlusion beyond the right femoral artery (Fig. 1, left). The patient’s clinical course after admission is shown in Fig. 2. Following emergency endovascular thrombectomy on the first day, hemodiafiltration (HDF) was initiated on the 2nd day due to the development of rhabdomyolysis and hypermyoglobinemia. Blood tests on this day revealed high levels of creatine kinase (CK, 82,951 IU/L) and myoglobin (7,237 ng/mL). A polyester polymer alloy (PEPA) dialyzer was used for HDF. Additionally, the patient developed compartment syndrome due to elevated internal pressure in the lower leg and underwent emergency fasciotomy (Fig. 1, right). Although the myoglobin level temporarily increased to 10,776 ng/mL on the 6th day of admission, the patient was successfully weaned off HDF. Throughout the treatment, the patient’s circulation remained stable, his urine output was maintained, and creatinine levels stayed within the normal range. After receiving negative pressure wound treatment for compartment syndrome, a skin graft was performed, and the wound was closed. The patient was transferred for rehabilitation on the 35th day.Fig. 1. Diagnostic image findings. a Contrast-enhanced computed tomography scan at the time of transport to the hospital. Occlusion beyond the right femoral artery was observed (closed arrow). b On the 2nd day, the patient developed compartment syndrome in the right lower leg and underwent an emergency fasciotomy. No obvious necrotic tissue was foundFig. 2Post-hospitalization course. After transport, emergency thrombectomy was performed, and hemodiafiltration was started on the second day due to high myoglobin and creatine kinase levels. On the same day, the patient developed compartment syndrome and underwent emergency fasciotomy. Despite a further increase in myoglobin and creatine kinase levels, urine output remained stable, and creatinine and potassium levels stayed within the normal range. The patient was weaned off hemodiafiltration on the 6th day. Circulation was stable during the disease. Gray bars indicate urine volume (mL/day) and black bars indicate infusion volume (mL/day). Dialysis prescription: duration of session, 8 hours; mode, postdilution-HDF; Q_D_, 500 mL/minute; Q_B_, 200 mL/minute; Q_S_, 3.6L/h; filtration membrane, Nikkiso FDZ-21 surface area 2.1 m^2^
Discussion and conclusion
Acute limb ischemia occurs due to a sudden decrease in arterial perfusion in the extremities, necessitating rapid revascularization such as endovascular treatment or surgery. While the occurrence of acute limb ischemia is rare, its incidence is higher in patients with preexisting advanced peripheral arterial disease, as seen in this case. Nontraumatic cases, such as the present case, can be broadly classified as embolic or thrombotic; however, the most common etiology is acute thrombosis of bypass grafts or stents [6]. Ischemia-damaged skeletal muscle cells are placed in an anaerobic environment where aerobic metabolism and oxidative phosphorylation are markedly reduced, eventually leading to cell death. Reperfusion releases electrolytes, CK, and Mb [7]. Rhabdomyolysis is a clinical syndrome caused by skeletal muscle damage and the release of these substances into the circulation. It can range from asymptomatic to severe, including compartment syndrome and AKI [1, 8]. Rhabdomyolysis diagnosis is usually made by confirmation of elevated blood levels of components present in muscle cells, such as CK and Mb (> five times the upper limit of normal for CK) [2, 9, 10]. However, CK levels are highly variable, and their effects on individuals differ widely, while the nephrotoxicity caused by CK remains unclear. In contrast, some studies suggest that Mb is not a reliable diagnostic indicator [2]; however, nephrotoxicity has been indicated for some time [11] and is considered the main cause of AKI triggered by rhabdomyolysis [12]. This suggests its usefulness as a biomarker [13], and since there have been reports that AKI incidence was significantly higher in cases with peak serum Mb levels > 15,000 μg/L, it is considered a reliable indicator for determining disease status [1, 10].
Renal replacement therapy (RRT) is not the first choice for preventing AKI progression due to rhabdomyolysis, particularly in patients with preserved urine output [1]. However, when urine output is reduced, Mb tends to form a column with uromodulin in the thick ascending leg, inhibiting renal excretion of Mb and promoting tubular damage [1], indicating that the removal of Mb and other inflammatory substances and early intervention may reduce this risk [2–5]. Although reports indicate that continuous RRT is more stable than intermittent RRT in terms of circulatory dynamics [3], many patients with rhabdomyolysis maintain stable circulatory function after adequate infusion load, making intermittent RRT a viable option. However, it remains unclear whether hemodialysis or HDF is more effective.
Although we administered adequate infusions for rhabdomyolysis from the outset [14], Mb levels continued to rise. Despite maintaining urine output, we determined that early intervention beyond infusions was necessary. Bicarbonate and mannitol have been demonstrated to be ineffective in treating rhabdomyolysis [14], and loop diuretics may exacerbate Mb precipitation and worsen distal tubular obstruction [15]. While some guidelines suggest initiating RRT for rhabdomyolysis on the basis of conventional indications for AKI and the degree of renal dysfunction [16], other studies indicate that early HDF may reduce the risk of AKI [5]. The patient had previously undergone bypass grafting for lower extremity arteriosclerosis obliterans and was prone to thrombosis, with compartment syndrome postoperatively. Additionally, the patient had undergone nephrectomy owing to a previous traumatic injury, resulting in a relatively low renal reserve. This condition increased the likelihood of declining urine output, making the patient more susceptible to AKI and its progression to chronic renal failure. Therefore, we decided to initiate RRT. We selected HDF (dialysis prescription shown in Fig. 2) because it is the standard method employed in our intensive care unit. Given the molecular weight of Mb, we expected a higher removal rate. In our experience, patients with Mb levels > 3,000 ng/mL or with a tendency to develop AKI often started HDF on the 2nd day of treatment. We decided to withdraw HDF based on the patient’s vital signs; urine volume; and Cre, CK, and Mb values as well as their trends. In our department, Mb values are used as an index to determine the effectiveness of treatment, and trends in CK values are used only as a reference. Although CK and Mb values can be measured at any time in our hospital, the effects of CK on the body, such as nephrotoxicity, as described above, remain unclear, and we have found no consensus on using CK values as an indicator for induction and withdrawal of blood purification [17, 18]. Regarding RRT, because the patient’s vital signs were stable and urine output was maintained from the beginning, we judged that the patient’s hemodynamics were stable and decided to perform intermittent HDF after consultation with a clinical engineer. For efficient Mb removal, a PEPA dialyzer (Nikkiso, FDZ-21, surface area of 2.1 m^2^) was selected as the filtration membrane. Throughout the treatment, urine output remained sufficient, and Cre levels stayed within the normal range. As demonstrated in this case, early initiation of HDF may effectively prevent AKI progression in patients with hypermyoglobinemia and reduced renal reserve. Additionally, intermittent RRT can be sufficient when the patient’s hemodynamic condition is stable.
In conclusion, we encountered a case of acute blood purification therapy for hypermyoglobinemia caused by rhabdomyolysis following reperfusion injury after acute limb ischemia. Early intervention with hemodialysis may help prevent AKI progression in such cases. Furthermore, this study suggests that intermittent hemodiafiltration dialysis can be an effective treatment option.