Scout In, Scout out: Savi scout reflector traversing a dilated duct to the nipple in breast cancer localisation—a case report
Aman Saswat Sahoo, Monther Salman, Bhuvi Singh, Gina Weston-Petrides, Lilia Ragad, Rasheed Elayyan

TL;DR
A breast cancer patient's tracking device migrated through a dilated duct and exited the nipple, highlighting the need for careful placement.
Contribution
This is the first reported case of a Savi Scout reflector migrating through a dilated duct and emerging at the nipple.
Findings
A Savi Scout reflector migrated through a dilated duct and exited the nipple, causing pain.
Proper positioning of the reflector can prevent migration and reduce patient discomfort.
Anatomical variations like dilated ducts should be considered before device placement.
Abstract
Introduction: Savi scout system is being widely used for localising and excising breast tumours. While the migration of scout reflectors has been documented, this is the first case of a Savi Scout reflector migrating through a dilated duct near the lesion and coming out of the nipple. Case Presentation: A 56-year-old postmenopausal woman with a history of right breast intraductal papilloma which transformed to Grade II Invasive Ductal Carcinoma (IDC) has a Savi Scout reflector placed in the tumour. However, it migrated through a dilated duct and emerged at the nipple, causing severe pain. The reflector was then surgically removed, and the patient subsequently underwent wide local excision with skin marker localisation. Conclusion: Anatomical variations such as presence of dilated ducts need to be considered before placing scout reflectors. Appropriate positioning would prevent them from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
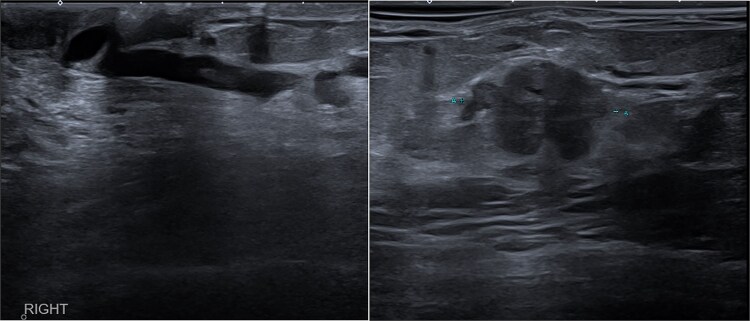 Figure 1
Figure 1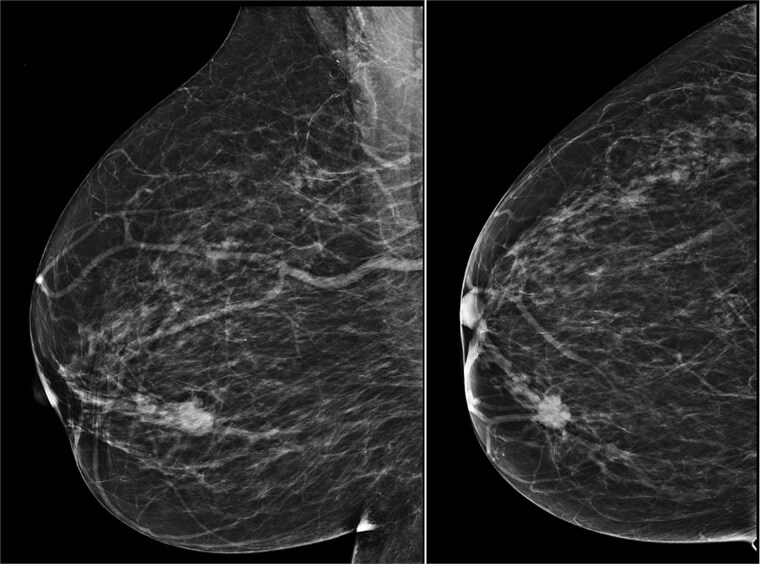 Figure 2
Figure 2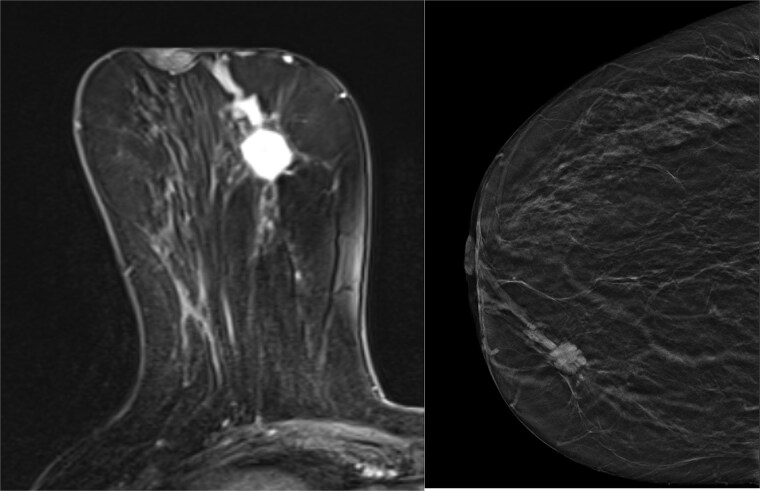 Figure 3
Figure 3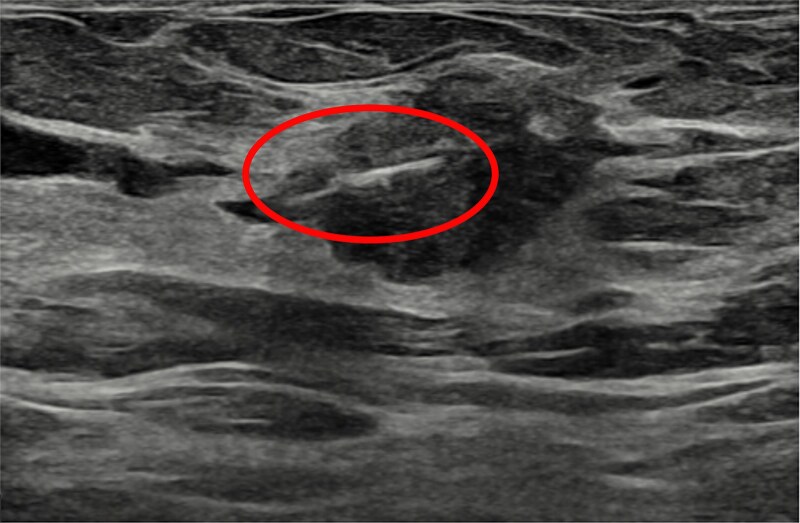 Figure 4
Figure 4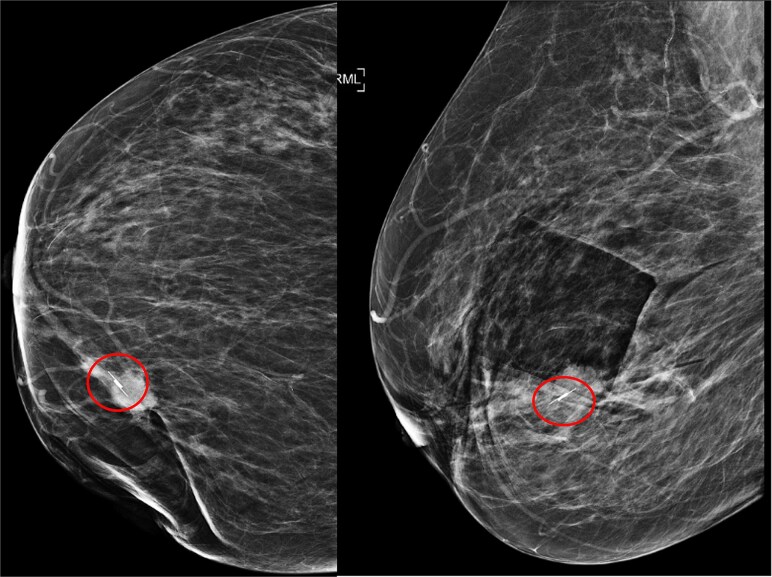 Figure 5
Figure 5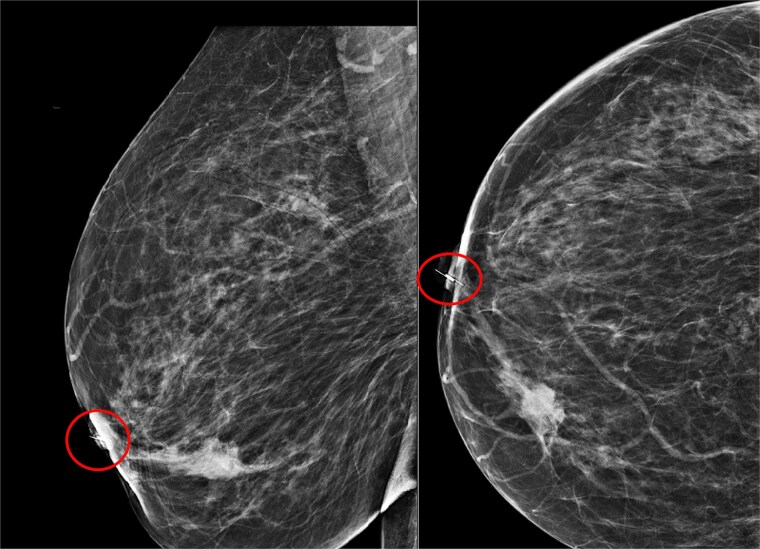 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Breast Lesions and Carcinomas · Cancer Diagnosis and Treatment
Introduction
Novel techniques to facilitate precise localisation for wide local excision include the Savi Scout (SS) system, which has been used since 2014. A small radar-activated reflector measuring 12 × 1.6 mm is placed percutaneously in the lesion under image guidance. A handheld probe is used to identify the lesion margins and allows the surgeon to easily excise the tumour [1].
From a patient’s perspective, the SS reflector has no external wires placed through the skin, further enhancing patient experience. It is associated with common complications like bleeding and infection. There have been documented instances of both minor and significant migration of the reflector. However, most literature reports no complications with the use of SS.
Herein, we present a case involving a patient with an impalpable invasive cancer of the breast who underwent placement of a SS reflector within the tumour. However, the reflector migrated from the tumour, traversed a dilated duct, and eventually came out through the nipple. The first of its kind.
Case presentation
A 56-year-old postmenopausal woman presented with a history of intermittent mastalgia, mild lumpiness, and clear nipple discharge of the right breast, which started a year ago. She has a previous known history of right breast intraductal papilloma without atypia 8 years ago, for which she refused the intervention at that time. Her mammogram two years ago was reassuring.
An ultrasound scan revealed a highly suspicious mass at the 2 o’clock position of the right breast periareolar area, measuring 17 mm, with a hypoechoic dilated duct measuring over 50 mm in length and 3.4 mm in diameter at the medial aspect of the right nipple (Fig. 1). The axilla appeared normal on the ultrasound scan.
Initial USS of the dilated duct of Rt breast (left), initial USS of IDC lesion in Rt breast (right).
Upon comparison of mammograms from eight years ago and two years ago, the lesion was identified as a new development (Fig. 2). An ultrasound-guided core biopsy of the right breast mass was performed. The histopathological evaluation revealed a Grade II Invasive Ductal Carcinoma.
Mammogram of the lesion in breast RMLO (left) and RCC (right).
After a multidisciplinary team meeting, a Magnetic Resonance Imaging (MRI) and breast tomosynthesis were ordered to assess the disease extent (Fig. 3). The known malignancy of the upper inner quadrant was identified, measuring 26 mm in the longest dimension. The MRI study identified an anterior extension accounting for an overall extent of 31 mm.
MRI of Rt breast (left), Tomosynthesis of Rt breast (right).
A SS reflector was placed at the site of the tumour under ultrasound guidance (Fig. 4). No immediate complications were noted. Post-insertion mammogram has been obtained.
USS showing Savi scout placed in the lesion.
Imaging revealed that the scout was successfully placed in the lesion (Fig. 5).
Mammogram post Savi scout (circled) insertion RCC view (left), mammogram post Savi scout insertion (circled) RLMO view (right).
Two days later, the patient presented to the breast clinic complaining of severe stabbing pain in the right nipple. An ultrasound and mammogram scan revealed that the scout had migrated from the site of the cancer into the duct at the tip of the nipple (Fig. 6).
Mammogram of migrated Savi scout RMLO view (left), mammogram of migrated Savi scout RCC view (right).
Under local anaesthesia, a small incision was made on the skin over the tip of the scout, and it was removed. The patient visited the clinic the next day and reported reduced pain and discomfort since the scout was removed.
The patient declined to have another SS reflector due to distress during the initial procedure. The decision has been made to proceed with skin marker-guided wide local excision, which she has had. Postoperative histopathological evaluation showed 27 mm grade 2 invasive ductal carcinoma (IDC) no special type, with no associated ductal carcinoma in situ, which is completely excised, and sentinel node biopsy was negative.
Discussion
This case describes an unreported complication where the SS migrated through a dilated duct to the nipple. The migration is attributed to a dilated duct with a diameter of 3.4 mm, large enough for the 1.6 mm wide device to traverse (Fig. 1). Bhattarai et al. [2] demonstrated the association between ductal papilloma and ductal dilation, with ducts ranging from 2 to 10 mm in diameter.
The American Society of Breast Surgeons [3] recommends excising papillomas due to their malignancy risk, as 67% of papillary lesions with atypia are upgraded upon excision. In this case, an intraductal papilloma may have progressed to invasive ductal carcinoma.
Ultrasound and mammogram images showed the tumour adjacent to a dilated duct, emphasizing the importance of careful device placement. Kramer et al. [4] highlight that tomosynthesis-guided Scout reflector placement with a lateral arm attachment improves control, precision, and efficiency by allowing single-view procedures, reducing radiation and time.
Hayes et al. [5] reported a 1% migration rate with SS with potential complications such as pain, infection, and non-functional devices Mango et al. [6] noted migration in one of fifteen cases due to post-biopsy hematoma, though no reports exist of SS migration to the nipple. In a study with 72 SS reflectors, the reported migration rate was 0% [7]. Magseed, an alternative, has a twisted design which promotes tissue in-growth which anchors it firmly reducing chances of migration. In a study of 1123 Magseeds only 2.5% migrated [8]. LOCalizer, another alternative, in a study of 848 patients had a migration rate of 0.7% [9]. There is no statistical difference between the migration rate of all these devices. Wire localisation has a re-positioning rate of 4% [10] and these wire-free methods are a significant improvement. The SS is preferred for patients undergoing neoadjuvant chemotherapy as it uses infrared signals which do not generate MRI artifacts unlike the Magseed. This allows earlier deployment of SS in patients. However, it may fail to generate signals in deeply located lesions.
This case highlights the need for attention when placing localization devices near dilated ducts. However, there are no reports of migration of the SS reflector from the original tumour site to the nipple.
Conclusion
The primary takeaway is the role of imaging, identification of ducts and precise localisation, considering structural anatomy, to minimise the migration of the SS reflector or other localisation devices, moreover, importance of excising papillary lesions to prevent future malignant transformations and structural changes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kasem I, Mokbel K. Savi scout® radar localisation of non-palpable breast lesions: systematic review and pooled analysis of 842 cases. Anticancer Res 2020;40:3633–43. 10.21873/anticanres.14352.32620602 · doi ↗ · pubmed ↗
- 2Bhattarai N, Kanemaki Y, Kurihara Y. et al. Intraductal papilloma: features on MR Ductography using a microscopic coil. Am J Roentgenol 2006;186:44–7. 10.2214/AJR.04.1600.16357375 · doi ↗ · pubmed ↗
- 3The American Society of Breast Surgeons . Consensus guideline on concordance assessment of image-guided breast biopsies and Management of Borderline or high-risk lesions [internet]. Available from:. https://www.breastsurgeons.org/docs/statements/Consensus-Guideline-on-Concordance-Assessment-of-Image-Guided-Breast-Biopsies.pdf.
- 4Kramer JM, Jordan SG, Chiang JTA. Use of the lateral arm in tomosynthesis-guided SCOUT reflector placement procedures. Clin Imaging 2024;109:110130. 10.1016/j.clinimag.2024.110130.38490080 · doi ↗ · pubmed ↗
- 5Hayes MK, Bloomquist E, Wright H. et al. Evaluation of longer duration use of the SAVI SCOUT surgical guidance system for excision of breast and axillary lesions in neo-adjuvant therapy patients: a pilot study short title: SAVI SCOUT time pilot study [internet]. 2018. Available from: https://cdn.clinicaltrials.gov/large-docs/49/NCT 03015649/Prot_SAP_001.pdf.
- 6Mango V, Ha R, Gomberawalla A. et al. Evaluation of the SAVI SCOUT surgical guidance system for localization and excision of nonpalpable breast lesions: a feasibility study. Am J Roentgenol 2016;207:W 69–72. 10.2214/ajr.15.15962.27304083 · doi ↗ · pubmed ↗
- 7Wazir U, Kasem I, Michell MJ. et al. Reflector-guided localisation of non-palpable breast lesions: a prospective evaluation of the SAVI SCOUT® system. Cancers 2021;13:2409. 10.3390/cancers 13102409.34067552 PMC 8156313 · doi ↗ · pubmed ↗
- 8Depretto C, Pepa GD, De Berardinis C. et al. Magnetic localization of breast lesions: a large-scale European evaluation in a National Cancer Institute. Clin Breast Cancer 2023;23:e 491–8. 10.1016/j.clbc.2023.08.004.37704563 · doi ↗ · pubmed ↗