Rare finding of Corynebacterium bovis in a facial surgical wound
Sach Thakker, Micah Belzberg, Elise Ng

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1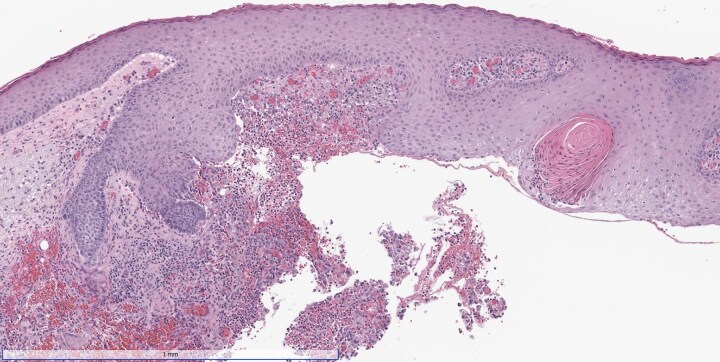 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiphtheria, Corynebacterium, and Tetanus · Anorectal Disease Treatments and Outcomes · Mycobacterium research and diagnosis
Dear Editor, A man in his 50s developed atypical operative site skin changes 2 weeks after Mohs surgery for an invasive squamous cell carcinoma on his right cheek [American Joint Committee on Cancer (AJCC) stage T1, Brigham and Women’s Hospital (BWH) stage T1]. The growth was cleared in a single stage and closed in a layered fashion with polyglactin 910 and polypropylene sutures. His medical history included a liver transplant for which he was taking long-term tacrolimus for immunosuppression; and a deep venous thrombosis for which he was taking apixaban. Initially, the wound healed well without signs of infection. However, 2 weeks postsurgery the patient experienced progressive redness, dull pain and swelling near the suture line. Oral doxycycline provided slight improvement, but symptoms worsened, prompting re-evaluation. Physical examination revealed a violaceous, erythematous plaque with induration and patterned purpuric plaques at the suture positions (Figure 1). Punch biopsy showed a granulomatous and neutrophilic infiltrate, while Gram stain highlighted clusters of Gram-positive cocci and coccobacilli (Figure 2). Wound swab was deferred in the absence of purulent drainage or fluctuance. An additional punch biopsy for culture grew Corynebacterium bovis as identified using matrix-assisted laser desorption–ionization time-of-flight mass spectrometry. Susceptibility testing revealed sensitivities to erythromycin, gentamicin, penicillin and vancomycin. Our institution’s infectious disease department chose a 7-day course of amoxicillin 500 mg three times daily, based on the results of the sensitivity testing, in respect of the ‘antibiotic ladder’ and in accordance with the literature.^1–3^ The patient subsequently experienced complete symptom resolution. The infection resolved with antibiotic treatment alone, avoiding suture removal and surgical revision.
Corynebacterium bovis is a facultatively anaerobic, catalase-positive, Gram-positive bacterium, commonly associated with bovine mastitis and dermatitis in immunocompromised mice. Human infections are rare, with only 18 reported cases, primarily at ocular, prosthetic joint or neurosurgical sites.^1,2^ In this case, the source of infection was unclear as the patient denied contact with farm animals or rodents. Corynebacterium bovis has been isolated from Merino sheep in Argentina, and following surgery the patient wore a new Merino sweater.^3^ There are no established guidelines for C. bovis infections in humans, although penicillin has shown effectiveness.^1–3^ However, the literature notes increasing instances of biofilm-forming and multidrug-resistant strains of Corynebacterium, including C. bovis, emphasizing the need for targeted antimicrobial treatment.^4^ Unlike other Corynebacterium species, C. bovis is not among normal human flora, and its presence in deeper tissue cultures should not be dismissed as contamination.^5^ Additionally, polyglactin 910 sutures often induce granulomatous reactions and are more susceptible to biofilm formation compared with non-braided sutures, suggesting avoidance of these suture types in patients at increased risk of infection, such as those on long-term immunosuppression.^6,7^ Evidence supporting antibiotic prophylaxis for immunosuppressed patients undergoing dermatological procedures is mixed and it is therefore not routinely performed at our institution.^8^
Funding sources: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability: The data underlying this article will be shared on reasonable request to the corresponding author.
Ethics statement: Not applicable.
Patient consent: Written patient consent for publication was obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gabay S, Tene Y, Ben-Ami R, Shapira Y. Corynebacterium bovis surgical site infection and brain abscess: the first case report and literature review. ID Cases 2023; 33:e 01782.37273774 10.1016/j.idcr.2023.e 01782 PMC 10236288 · doi ↗ · pubmed ↗
- 2Elsheikh M, Elsayed A, Bennett N, Connor M. Corynebacterium bovis: a rare case of persistent bacterial keratitis and corneal perforation. Cureus 2021; 13:e 16913.34513486 10.7759/cureus.16913 PMC 8412843 · doi ↗ · pubmed ↗
- 3Abdala AM, Farber M, Robles CA. Sisal wool skin disease in merino sheep in the Argentine Patagonia region: identification and molecular diagnosis of Corynebacterium bovis from skin lesions. Vet Dermatol 2022; 34:7–13.36177533 10.1111/vde.13124 · doi ↗ · pubmed ↗
- 4Chandran R, Puthukkichal DR, Suman E, Mangalore SK. Diphtheroids—important nosocomial pathogens. J Clin Diagn Res 2016; 10:DC 28–31.10.7860/JCDR/2016/19098.9043 PMC 529643228208859 · doi ↗ · pubmed ↗
- 5Chow S, Bui U, Clarridge J. Corynebacterium bovis eye infections, Washington, USA, 2013. Emerg Infect Dis 2015; 21:1687–9.26291771 10.3201/eid 2109.150520 PMC 4550150 · doi ↗ · pubmed ↗
- 6Cartmill BT, Parham DM, Strike PW et al How do absorbable sutures absorb? A prospective double-blind randomized clinical study of tissue reaction to polyglactin 910 sutures in human skin. Orbit 2014; 33:437–43.25244631 10.3109/01676830.2014.950285 · doi ↗ · pubmed ↗
- 7Henry-Stanley MJ, Hess DJ, Barnes AM et al Bacterial contamination of surgical suture resembles a biofilm. Surg Infect (Larchmt) 2010; 11:433–9.20673144 10.1089/sur.2010.006PMC 2967823 · doi ↗ · pubmed ↗
- 8Balakirski G, Löser CR, Dippel E et al Surgical site infections after microscopically controlled skin surgery in immunocompromised patients: a retrospective two-center cohort study. Arch Dermatol Res 2020; 312:491–9.32009218 10.1007/s 00403-020-02035-8 · doi ↗ · pubmed ↗