Drug-Induced Liver Injury After Zoledronic Acid Infusion and Literature Review
Christopher Boldt, Pooja Prasad, Huifang Lu

TL;DR
A 50-year-old woman developed acute liver injury after receiving zoledronic acid, highlighting a rare but serious side effect of the drug.
Contribution
This case report adds to the limited evidence on zoledronic acid-induced hepatotoxicity and raises awareness among clinicians.
Findings
The patient experienced acute liver injury shortly after zoledronic acid infusion.
Liver enzymes normalized within 11 days after the incident.
No preexisting liver disease or viral hepatitis was found in the patient.
Abstract
Zoledronic acid, a bisphosphonate, is commonly used to treat and prevent osteoporosis. Here we report a rare case of acute hepatotoxicity after zoledronic acid infusion in a 50-year-old female patient with no preexisting liver disease taking anastrozole and abemaciclib. Only a few hours after her infusion, the patient developed severe body aches, nausea, and abdominal bloating. Laboratory tests revealed an acute liver injury. Acute viral hepatitis workup was negative, and she was subsequently diagnosed with a hepatocellular drug-induced liver injury. Her transaminitis downtrended over the following day and normalized after 11 days. Given this rarely reported side effect, there is a paucity of evidence to guide treatment decisions. The goal of this case report is to increase awareness of this adverse effect, especially among patients taking other potentially hepatotoxic drugs.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
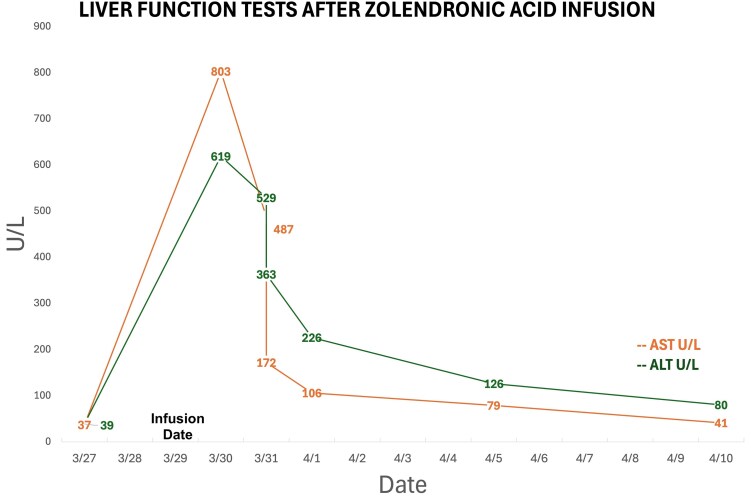 Figure 1
Figure 1| Laboratory test | Units (conventional) | Units | Normal reference range, conventional (SI) |
|---|---|---|---|
| (SI) | |||
| Aspartate Aminotransferase | 803 U/L | 13.4 µkat/L | 10-30 U/L (0-0.58 µkat/L) |
| Alanine aminotransferase | 619 U/L | 10.3 µkat/L | 10-40 U/L (0.17-0.92 µkat/L) |
| Alkaline phosphatase | 122 U/L | 2.0 µkat/L | 30-130 U/L (0.73-2.45 µkat/L) |
| Gamma-glutamyl transpeptidase | 639 U/L | 10.7 µkat/L | 5-40 U/L (0.08-0.67 µkat/L) |
| Phosphorus | 1.7 mg/dL | 0.54 mmol/L | 2.5-4.5 mg/dL (0.81-1.45 mmol/L) |
| Bilirubin (total) | 0.8 mg/dL | 13.6 µmol/L | 0.1-1.2 mg/dL (1.7-20.5 µmol/L) |
| Amylase | 70 U/L | 1.17 µkat/L | 40-140 U/L (0.38-1.42 µkat/L) |
| Lipase | 50 U/L | 0.84 µkat/L | 0-160 U/L (0.17-2.35 µkat/L) |
| Creatine kinase | 50 U/L | 0.84 µkat/L | 20-50 U/L (0.63-2.91 µkat/L) |
| Calcium | 8.9 mg/dL | 2.4 mmol/L | 8.5-10.2 mg/dL (2.2-2.7 mmol/L) |
| Serological testing for viral hepatitis | |||
| Anti-hepatitis A antibody | Negative | — | — |
| Hepatitis B surface antigen | Negative | — | — |
| Anti-hepatitis B surface antibody | Negative | — | — |
| Hepatitis B e antigen | Negative | — | — |
| Anti-hepatitis B e antibody | Negative | — | — |
| Anti-hepatitis B core antibody | Negative | — | — |
| Hepatitis B virus deoxyribonucleic acid | Negative | — | — |
| Anti-hepatitis C antibody | Negative | — | — |
| Hepatitis C virus ribonucleic acid | Negative | — | — |
| Year published | Age (years)/sex | Bisphosphonate | Underlying disease (PMH) | Time of first reported LFT elevation after starting therapy | Time to LFT normalization after discontinuation | Other complications | |
|---|---|---|---|---|---|---|---|
| Case 1 [ | 2010 | 53/F | Zoledronic acid | Paget disease | 24 hours | 7 days | NA |
| Case 2 [ | 2013 | 73/F | Zoledronic acid | Primary osteoporosis | 72 hours | 12 days | NA |
| Case 3 [ | 2015 | 50/F | Zoledronic acid | Glucocorticoid-induced osteoporosis (Bechet's) | 72 hours | 9 days | NA |
| Case 4 [ | 2017 | 73/F | Zoledronic acid | Primary osteoporosis | 7 days | 91 days | Autoimmune hepatitis |
| Case 5 [ | 2022 | 55/F | Zoledronic acid | Sheehan syndrome | 24 hours | 6 days | NA |
| Our case | 2024 | 50/F | Zoledronic acid | Aromatase inhibitor- | 12 hours | 13 days | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and treatments · Lung Cancer Treatments and Mutations · Neuroendocrine Tumor Research Advances
Introduction
While aromatase inhibitors have revolutionized breast cancer treatment, prolonged use is associated with side effects, such as bone loss and increased fracture risk [1]. Zoledronic acid (ZOL), a bisphosphonate (BP) given intravenously, has been approved for treating aromatase inhibitor-induced osteoporosis. The overall safety of BP treatment is well established. The most common adverse effects are flu-like symptoms after ZOL infusion, including fever, chills, myalgia, and arthralgia. BP-induced liver injury is rare, and specifically with ZOL, there have been only 5 previously reported cases [2-6]. Here we report acute hepatotoxicity after ZOL infusion, which did not recur after switching to another BP.
Case Presentation
A 50-year-old female patient presented to the rheumatology clinic for osteoporosis management. Her past medical history was notable for invasive ductal carcinoma of her right breast, treated with surgery, chemotherapy, radiation, and then hormonal therapy with anastrozole and abemaciclib, to be taken for the next 10 years. About 4 months before starting anastrozole, she had a dual-energy x-ray absorptiometry scan indicating osteopenia, with T scores ranging from −1.9 to −2.4. Two weeks after starting her anastrozole prescription, she was first seen in our bone health clinic. Given her T scores in the osteopenic range while now on hormonal therapy, antiresorptive treatment was recommended. Despite counseling, the patient declined and proceeded first to try conservative measures. Her dual-energy x-ray absorptiometry scan 1 year later showed a 3.0% to 6.0% bone mineral density loss with T scores now from −2.2 to −2.7, moving her into the osteoporotic range. Now with osteoporosis while on an aromatase inhibitor, she agreed to antiresorptive therapy. After an extensive discussion of her options, including once every 6 months ZOL 4 mg intravenously, denosumab 60 mg subcutaneously every 6 months, or ZOL 5 mg intravenously once every 12 months, a compromise was made to start with ZOL 5 mg intravenously due to the cost of international travel and lodging, which was prohibitive for this patient [7, 8].
Within a few hours of receiving her first infusion of ZOL, the patient reported severe bone pain, abdominal pain, bloating, and nausea. She presented to the emergency department afebrile, normotensive, but tachycardic. She denied fevers, chills, and any history of drug or alcohol consumption.
Diagnostic Assessment
Physical exam was notable for diffuse abdominal distention and tenderness without rebound or guarding. No jaundice or pruritus was appreciated. Laboratory tests were significant for an elevated transaminitis, alkaline phosphatase, and gamma-glutamyl transpeptidase; low phosphorus; normal bilirubin; normal amylase/lipase; normal creatine kinase; and normal calcium. Her serological testing for viral hepatitis was negative (Table 1). Before this event, her serum liver enzyme levels were always within normal range on routine screening tests (Fig. 1). A computed tomography scan of her abdomen/pelvis did not show any acute new findings. She had no prior history of liver disease and no evidence of metabolic dysfunction-associated steatotic liver disease on imaging. Her medications at that time included anastrozole, abemaciclib, vitamin D3, gabapentin, polyethylene glycol, and sennoside.
Liver function test elevation following zoledronic acid infusion.
Treatment
The timing of the presentation and history suggested a hepatocellular drug-induced liver injury. The patient's pain and nausea improved with analgesics (ibuprofen 400 mg tablet every 6 hours as needed for mild pain and morphine sulfate immediate release 15 mg tablet every 4 hours as needed for moderate/severe pain) and antiemetics (first-line ondansetron 4 mg tablet every 4 hours as needed and second-line prochlorperazine IV push 5 mg every 6 hours as needed). Her liver function tests downtrended during her hospital admission (Fig. 1), and she was subsequently discharged when symptoms resolved. Anastrozole and abemaciclib were both held for 1 week while she was an inpatient and restarted on hospital discharge, and her liver function tests continued to downtrend as an outpatient.
Outcome and Follow-up
Over the next month, her transaminitis gradually normalized. The decision was made to avoid ZOL in the future, and the patient was given alendronate a year later, which has been well tolerated. We discussed trialing denosumab, but since the patient lives overseas and could only visit our institution annually, she would have needed to find a local physician to treat her osteoporosis. Instead, she chose to start oral alendronate and follow up annually due to these logistical limitations. In addition, she will need antiresorptive therapy for more than 5 years as her anastrozole was planned for 10 years; thus the potential rebound bone loss and fracture risk after prolonged denosumab without close monitoring was a concern.
Discussion
Fever, myalgia, and flu-like symptoms are some of the most common side effects after ZOL infusion. However, ZOL and other bisphosphonate-induced hepatotoxicity have rarely been reported [2-6, 9-11]. Up to this point, 5 previous cases have described liver injury following ZOL administration (Table 2): a 53-year-old female treated for Paget disease [2], a 73-year-old female treated for primary osteoporosis [3], a 50-year-old female with glucocorticoid-induced osteoporosis [4], and a 55-year-old with Sheehan syndrome [5]. In these cases, the patient's liver injury occurred less than 3 days after ZOL infusion, and liver function tests (LFTs) returned to baseline within 12 days. Interestingly, 1 case described ZOL-induced autoimmune hepatitis requiring short-term immunosuppression after LFTs did not downtrend after more than 72 hours [5]. In our case, liver injury occurred within a few hours of ZOL infusion, and LFTs reached normal limits after 11 days. Given the rapid resolution of her LFTs, autoimmune hepatitis testing and early glucocorticoid treatment was not done. However, further testing would have been warranted if the LFTs did not downtrend within 24 hours.
Additionally, 3 prior cases have described liver injury following oral BP (alendronate and risedronate) administration [9-11]. In these cases, liver injury occurred 56 to 365 days after initial administration, then returned to baseline in 64 to 365 days. The difference in timing of liver injury due to oral BP is likely due to variable dosing compared to ZOL. There have been other cases of BP-induced hepatotoxicity reported with clodronate, risedronate, and ibandronate. In more than half of these cases, patients had a prior history of liver disease, and like our case, BP liver toxicity was mild to moderate [6].
Assessing preexisting risk factors, our patient had no known history of liver disease but was receiving concurrent immunotherapy with abemaciclib. Abemaciclib, a CDK-4 and CDK-6 inhibitor, can be a rare cause of liver injury. Taniguchi et al noted that patients taking abemaciclib while concurrently taking an aromatase inhibitor had an increased risk of liver injury [12]. Although our patient was taking both medications at the time, she had previously tolerated them for more than a year without hepatic injury until the administration of ZOL. The rapid, transient rise in LFTs following her first ZOL infusion is suggestive of BP-specific liver injury, which may have been augmented by taking abemaciclib and anastrozole.
The mechanism of BP-induced liver injury is not well understood. One mouse model study noted that ZOL induced apoptosis by increasing proinflammatory cytokines and oxidative stress, which can lead to subsequent liver damage [13]. Similarly, the transient increase in cytokines may explain the more common flu-like symptoms after ZOL infusion.
Learning Points
Hepatotoxicity is a rarely reported adverse effect of ZOL that resolved with discontinuation of the medication and did not recur after switching to another antiresorptive therapy.Patients with preexisting liver disease or taking concomitant hepatotoxic medications should be safely monitored for signs of liver damage.
Contributors
All authors made individual contributions to authorship. H.L. was involved in diagnosing and managing the patient and reviewing the manuscript. C.B. and P.P. were engaged in writing and submitting the manuscript. All authors reviewed and approved the final draft.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lester J, Coleman R. Bone loss and the aromatase inhibitors. Br J Cancer. 2005;93(S 1):S 16‐S 22.16100521 10.1038/sj.bjc.6602691 PMC 2361688 · doi ↗ · pubmed ↗
- 2Polyzos SA, Kountouras J, Anastasilakis AD, et al Zoledronic acid-induced transient hepatotoxicity in a patient effectively treated for Paget disease of bone. Osteoporos Int. 2011;22(1):363‐367.20407889 10.1007/s 00198-010-1230-5 · doi ↗ · pubmed ↗
- 3Lu Y, Pei Y, Shao Y, et al Hepatotoxicity induced by zoledronic acid in an aged woman with primary osteoporosis. EXCLI J. 2013;12:115‐117.27034632 PMC 4803018 · pubmed ↗
- 4Jiang Y, Fu Y, Xing XP, et al Zoledronic acid-induced hepatotoxicity relieved after subsequent infusions in a Chinese woman with glucocorticoid-induced osteoporosis. Eur J Med Res. 2015;20(1):68.26297149 10.1186/s 40001-015-0161-1PMC 4546306 · doi ↗ · pubmed ↗
- 5Laway BA, Mir SUI, Bashir MI. Transient hepatitis secondary to zoledronic acid in a woman with Sheehan syndrome. Indian J Endocrinol Metab. 2022;26(1):93‐94.35662756 10.4103/ijem.ijem_484_21PMC 9162249 · doi ↗ · pubmed ↗
- 6Schneider JS, Montani M, Stickel F. Drug-induced autoimmune hepatitis following treatment with zoledronic acid. Case Rep Gastroenterol. 2017;11(2):440‐445.29033761 10.1159/000479314 PMC 5624238 · doi ↗ · pubmed ↗
- 7Kotian P, Boloor A, Sreenivasan S. Study of adverse effect profile of parenteral zoledronic acid in female patients with osteoporosis. J Clin Diagn Res. 2016;10(1):OC 04‐OC 06.10.7860/JCDR/2016/17061.7021 PMC 474063326894105 · doi ↗ · pubmed ↗
- 8Shapiro CL, Van Poznak C, Lacchetti C, et al Management of osteoporosis in survivors of adult cancers with nonmetastatic disease: ASCO clinical practice guideline. J Clin Oncol. 2019;37(31):2916‐2946.31532726 10.1200/JCO.19.01696 · doi ↗ · pubmed ↗