Sleep Interruptions Among Older Adults Admitted to the Hospital
Adrian D. Haimovich, Suzanne M. Bertisch, Venkat Jegadeesan, Jennifer P. Stevens, Mara A. Schonberg, Sarah D. Berry

TL;DR
This study looked at how long older adults can sleep without interruption and what causes sleep disruptions during hospital stays.
Contribution
The study provides insights into sleep patterns and interruptions specific to older adults in hospital emergency admissions.
Findings
Older adults experience frequent sleep interruptions during hospital stays.
Emergency department admission is associated with reduced sleep continuity.
Types of interruptions vary but commonly include medical procedures and environmental factors.
Abstract
This cohort study examined the length of uninterrupted sleep and types of sleep interruptions in older adults admitted to the hospital through the emergency department.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
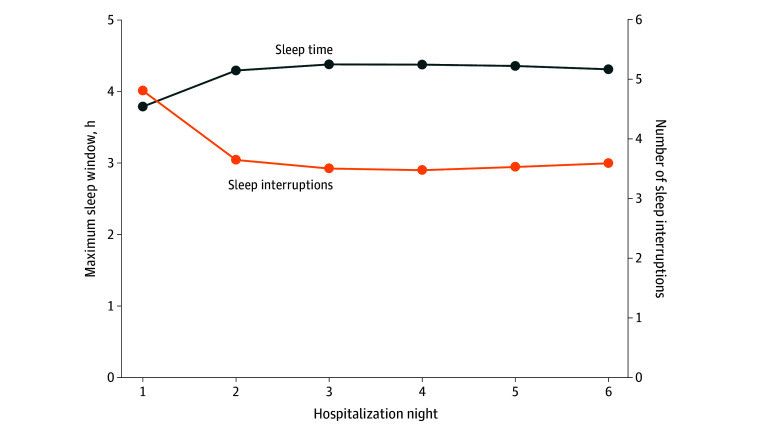 Figure 1
Figure 1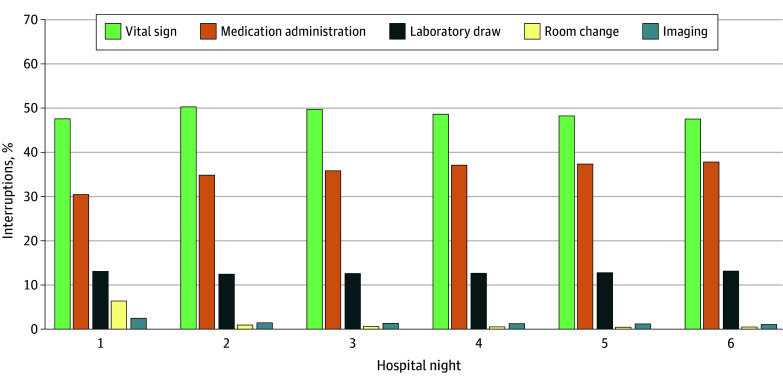 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSleep and related disorders · Context-Aware Activity Recognition Systems · Sleep and Work-Related Fatigue
Introduction
Sleep deprivation is common among hospitalized older adults and is associated with adverse effects.^1,2^ Hospital sleep barriers include environmental factors, patient conditions (eg, discomfort), and clinical care (eg, vital signs). Using data from electronic health records (EHRs), this study aims to characterize sleep interruptions for clinical care among older adults admitted from the emergency department (ED) within a large health care network.
Methods
This cohort study included patients aged 65 years or older admitted via the ED to medical-surgical beds at 6 hospitals (1 urban tertiary care, 1 suburban tertiary care, and 4 community) within the Beth Israel Lahey Health Network from June 1 to December 31, 2024. A sleep window from 9 pm to 5 am was defined for each hospitalization night, beginning after an ED clinician requested a hospital bed. Nights with incomplete data (bed request after 9 pm or discharge before 5 am) were excluded. Patient demographics and sleep interruptions—vital signs, medication administrations, imaging, or room changes—were identified using EHRs (eMethods in Supplement 1). The primary outcome was the maximum uninterrupted sleep window during hospitalization nights 1 to 6. Secondary outcomes included (1) percentage of maximum sleep windows at least 7 hours in duration in alignment with current sleep guidelines,^3^ (2) number of sleep interruptions per night, and (3) percentage of interruptions stratified by type of interruption. We stratified sleep duration and interruptions on hospitalization night 1 by whether patients boarded in the ED for 3 hours or more after bed request in accordance with the Age-Friendly Hospital Quality Measure.^4^ Beth Israel Deaconess Institutional Review Board deemed the study exempt with a waiver of informed consent because it was considered secondary research. We followed STROBE reporting guidelines. Two-sided t tests were performed, with P < .05 considered significant. Data were analyzed with Python 3.10.4 (Python Software Foundation).
Results
We included 19 017 patient admissions, accounting for 73 151 patient-nights. Mean (SD) patient age was 78.8 (8.6) years; 10 201 patients [53.6%] were female, with EHR-documented races and ethnicities as follows: 3.1% Asian, 6.6% Black, 4.0% Hispanic or Latino, and 85.8% White. Mean maximum sleep window was 3.8 (95% CI, 3.7-3.8) hours on hospitalization night 1, 4.3 (95% CI, 4.3-4.3) hours on night 2, and 4.3 (95% CI, 4.3-4.4) hours on night 6 (P < .001 for night 1 vs nights 2 and 6) (Figure 1). Percentage of maximum sleep windows at least 7-hours long was 2.9% (95% CI, 2.7-3.2) on night 1, 5.4% (95% CI, 5.1-5.7) on night 2, and 5.3% (95% CI, 4.4-5.8) on night 6 (P < .001 for night 1 vs nights 2 and 6). Mean number of sleep interruptions was 4.9 (95% CI, 4.8-4.9) on night 1, 3.7 (95% CI, 3.6-3.7) on night 2, and 3.6 (95% CI, 3.5-3.7) on night 6 (P < .001 for night 1 vs nights 2 and 6). The most common sleep interruption was checking vital signs, followed by medication administration (Figure 2). On night 1, 65.1% of patients boarded 3 hours or more in the ED and had a mean maximum sleep window of 3.7 (95% CI, 3.7-3.7) hours; those who boarded less than 3 hours had a mean maximum sleep window of 3.9 (95% CI, 3.9-4.0; *P *< .001). Patients boarding in the ED had more interruptions (4.9 [95% CI, 4.9-5.0] vs 4.6 [95% CI, 4.6-4.7]; P < .001), with similar proportions of patients having at least 7 hours of uninterrupted sleep (2.8% [95% CI, 2.6%-3.1%] vs 3.4% [95% CI, 2.9%-3.8%]; P =.76).
Number of Sleep Interruptions and Maximum Sleep Window by Hospitalization Night
Proportion of Overnight Interruptions by Clinical Task by Hospitalization Night
Discussion
Sleep disruptions were common, particularly on night 1, and were exacerbated among older patients boarding in the ED. Increased interruptions on night 1 may reflect ongoing evaluation. Across nights, vital signs were the primary interruption type. Quality improvement initiatives targeting clinical interruptions with multimodal rest-promoting interventions have not substantially altered sleep windows and patient satisfaction.^5,6^
Study limitations include reliance on timestamps to track interruptions, limited capture of diverse sleep disturbance types, absence of patient acuity measures, and use of single time points for imaging. Further research is needed to evaluate and mitigate hospital sleep disruption and its association with adverse patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stewart NH, Arora VM. Sleep in hospitalized older adults. Sleep Med Clin. 2018;13(1):127-135.29412979 10.1016/j.jsmc.2017.09.012PMC 5880551 · doi ↗ · pubmed ↗
- 2Burger P, Van den Ende ES, Lukman W, . Sleep in hospitalized pediatric and adult patients: a systematic review and meta-analysis. Sleep Med X. 2022;4(100059):100059.36406659 10.1016/j.sleepx.2022.100059 PMC 9672415 · doi ↗ · pubmed ↗
- 3Watson NF, Badr MS, Belenky G, . Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. J Clin Sleep Med. 2015;11(6):591-592.25979105 10.5664/jcsm.4758 PMC 4442216 · doi ↗ · pubmed ↗
- 4Depart of Health and Human Services; Centers for Medicare & Medicaid Services. Medicare and Medicaid Programs and the Children’s Health Insurance Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and Policy Changes and Fiscal Year 2025 Rates; Quality Programs Requirements; and Other Policy Changes. Federal Register. May 2, 2024. Accessed October 3, 2024. https://www.federalregister.gov/documents/2024/05/02/
- 5Najafi N, Robinson A, Pletcher MJ, Patel S. Effectiveness of an analytics-based intervention for reducing sleep interruption in hospitalized patients: a randomized clinical trial. JAMA Intern Med. 2022;182(2):172-177. doi:10.1001/jamainternmed.2021.738734962506 PMC 8715385 · doi ↗ · pubmed ↗
- 6Catley CD, Paynter K, Jackson K, . Redesigning the hospital environment to improve restfulness. JAMA Netw Open. 2024;7(12):e 2447790. doi:10.1001/jamanetworkopen.2024.4779039630451 PMC 11618460 · doi ↗ · pubmed ↗