Development of tele-lifestyle-based multidisciplinary survivorship program for gynecologic oncology practice
Nathalie D McKenzie, Nnamdi I Gwacham, Julie W Pepe, Sarfraz Ahmad, James E Kendrick, Robert W Holloway

TL;DR
A telemedicine-based multidisciplinary program for gynecologic cancer survivors improved lifestyle behaviors and quality of life, but faced challenges in recruitment and retention.
Contribution
Introduces a novel tele-lifestyle-based survivorship program integrating multiple specialties for gynecologic cancer survivors.
Findings
Participants showed significant improvement in quality of life and lifestyle adherence post-program.
Recruitment was suboptimal, with only 11.7% of potential participants joining.
85% of participants reported compliance with program recommendations.
Abstract
We assessed the recruitment and retention of a short 8-week telemedicine-based group peri-habilitation program for gynecologic cancer survivors. Multidisciplinary team included: a gynecologic oncologist with additional board certification by the American College of Lifestyle Medicine, cancer-specific nutritionist, culinary medicine chef, physical therapist, exercise physiologists, mental health counselor, body image aesthetician, pelvic floor therapist, and sex therapist. Pre- and post-self-administered questionnaires assessed conformity to lifestyle medicine pillars and a general medical symptom questionnaire (MSQ). Recruitment was suboptimal (11.7%). Neither provider referrals nor flyers sufficiently directed patients to the program, but those that completed the program expressed meaningful impact on lifestyle behavioral change and improved quality-of-life across multiple parameters…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
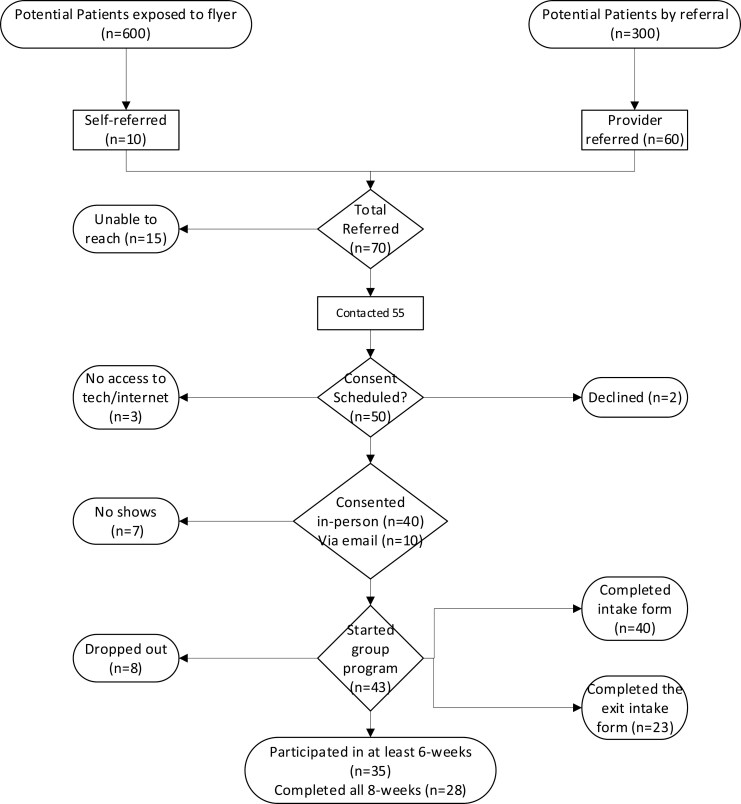 Figure 1
Figure 1| Pre-HEAL-GYN | Post-HEAL-GYN (±SD) |
|
| |
|---|---|---|---|---|
| BMI (kg/m2) | 29.13 ± 8.81 | 30.11 ± 8.36 |
| 17 |
| Sleep scores | 31.86 ± 5.87 | 27.64 ± 5.28 |
| 21 |
| Medical symptom questionnaire | 43.0 ± 23.02 | 20.75 ± 16.52 | ND | 4 |
| Overall health | 5.94 ± 1.73 | 6.95 ± 1.66 | .061 | 16 |
| Eating patterns | 4.96 ± 1.92 | 3.57 ± 1.59 |
| 23 |
| Weight management | 9.78 ± 2.41 | 9.61 ± 1.95 | .689 | 23 |
| Perceived stress | 11.48 ± 3.58 | 10.30 ± 3.27 |
| 23 |
| Resilience | 29.26 ± 4.39 | 31.22 ± 4.31 |
| 23 |
| Anxiety/Depression | 12.19 ± 8.68 | 6.91 ± 5.69 |
| 21 |
| Purpose/Connection | 34.73 ± 4.0 | 37.0 ± 3.57 |
| 22 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Family Support in Illness · Cancer-related cognitive impairment studies
Introduction
Gynecologic cancer survivors suffer from both physical and cognitive decline, while strategies to mitigate these and other quality-of-life (QoL) issues remain underutilized for this patient population.^1^ Yet, evidence suggests that adherence to the American Cancer Society nutrition and physical activity guidelines after a cancer diagnosis (ACS-NPG-AC) is associated with reduced morbidity, better QoL, and improved treatment outcomes.^2,3^ Indeed, the ACS-NPG-AC guidelines are consistent with recommendations published by other authoritative bodies including the American College of Lifestyle Medicine (ACLM) curriculum.^4^ Clinical interventions with diet or diet-plus-exercise are becoming more common, especially for other cancer types such as breast cancer.^5-7^ However, multimodality interventions incorporating all of the lifestyle pillars are largely absent and even more so for gynecologic cancers.^3,8,9^
Our tele-lifestyle-based peri-rehabilitation survivorship program (developed and modified during the COVID-19 pandemic) was branded as HEAL-GYN (Healthy Eating and Active Lifestyle—Gynecologic Cancer). This pilot program was developed to improve upon diet and exercise interventions for our gynecologic oncology patient population. HEAL-GYN focuses on all 6 pillars of lifestyle medicine.^3^ HEAL-GYN is led by a board-certified gynecologic oncologist with additional board certification by ACLM^4^ along with a multidisciplinary team who teach participants and lead activities on lifestyle pillars as recommended by the ACLM/ACS/AICR (American Institute for Cancer Research). Sexual dysfunction/intimacy/body image education is also provided.^3^ The specific interventions use a highly interactive educational format which incorporates motivational interviewing and goalsetting over 8-weekly consecutive shared peer-mentoring 90-minute sessions.^3^ During the pilot phase, we sought to explore recruitment strategies, feasibility, retention, behavioral impact, and short-term QoL for survivors.
Methods
Design
A longitudinal prospective pilot design with pre- and postquestionnaires using self-administered inventories about healthy behavior and a comprehensive medical symptom questionnaire (MSQ). All patients were interviewed after completing the program. We also used a team-based approach to conduct descriptive qualitative appraisal from focus group discussions, directly informed from the semi-structured interview questions that captured perceptions of acceptability of the program. Paired sample nonparametric tests were employed for the individual tests. No P-value adjustments were made for multiple tests conducted.
Patient population
Persons with a diagnosis of any gynecologic cancer treated at a single gynecologic oncology practice consisting of 4 physicians and 3 mid-level providers over an 18-month period.
Recruitment and program referral
Flyers were displayed on walls and doors within exam rooms, hallways, and as leaflets available at the practice check-out counter. Referral to the program relied on recall by physicians/providers during end of treatment discussions or cancer surveillance visits. Target patient population for the program was persons having completed treatment for gynecologic cancers within the previous 6-months; however, all patients were welcome to self-refer.
Retention
In addition to the hospital systems automated 24- to 48-hour previsit call/text reminders, 30 minutes prior to each of the 8-sessions, a medical assistant called all registered participants to make an additional reminder and to identify electronic issues precluding participation in that day’s session. Reasons for not being able to or no longer wanting to participate in the program were noted.
Pilot program description
Eight consecutive telemedicine-based shared medical visits each with a different focus topic. Our telemedicine team members included a cooking demonstration with a culinary medicine chef, a discussion with a registered dietician to discuss food quality, calories, and nutrient density, a mental health counselor, an exercise physiologist, and personal trainer instruction that included group exercise to provide safe alternatives to traditional exercise. Emphasis placed on the 6-pillars of lifestyle medicine^3,4^ (ie, whole-food plant-predominant diet, physical activity, sleep hygiene, stress management, “social connectedness,” limiting/avoid risky substances, eg, cigarettes). Prior to beginning the program, all participants received a printed copy of the ACLM adult-starter kit booklet highlighting strategies to enhance the 6-pillars. All 8-week cohorts received their program in the following sequence: Week 1: Intro and thorough discussion of all 6-pillars of lifestyle medicine ending with focus on social network optimization. Week 2: Healthy cooking demonstration inclusive of shopping and meal prep counseling. Week 3: Stress management. Week 4: Physical activity/exercise education and Yoga class participation. Week 5: Healthy eating for Cancer lecture and individual coaching. Week 6: Sleep optimization and strength training class. Week 7: Residual side effect education with body image and sexual issue lecture. Week 8: Conclusion and coaching for sustainability. Sessions concluded with each participant stating their SMART (Specific, Measurable, Attainable, Realistic, Time-specific) goal for that session’s topic. Each telemedicine encounter ranged from 90 to 120 minutes and were conducted every Wednesday in 8-consecutive week blocks. The physician billed for their time and the remainder of the health team’s time and supplies were covered through an intramural philanthropic grant. Participants were invited to join a closed-private social media group for peer-engagement and support. At the end of the feasibility study, additional resources were made available to provide individual consultations with a health coach beyond the program for the period of 1-year.
Results
Seventy gynecologic cancer patients were initially referred to this pilot program (12-month period) and 50 patients enrolled, of which 23 had complete data (Figure 1). Patients’ mean age was 58.8 years and mean starting body-mass index was 29.9 kg/m^2^. Patients with other (nongynecologic cancer types) who asked to join the program are not included in this report.
Recruitment and retention flow chart of the Healthy Eating and Active Lifestyle for Gynecologic Cancers pilot program.
Participants reported a statistically significant improvement along several parameters, specifically, perceived stress, levels of anxiety, and depression decreased. Levels of purpose and social connection increased. Significant improvements were also noted in patients’ eating patterns and ability to manage their weight during the 8 weeks (Table 1). Only 4 participants completed the MSQ section of the survey; however, there was a notable decrease in general symptoms (Table 1). Patients reported an increase in perceived levels of overall health after completion of the program although small numbers preclude statistical significance.
The participants’ self-reported overall compliance with the varying elements of the HEAL-GYN program was generally very high (90%). Additionally, 100% of participants would “highly recommend the program” and none complained of stress or altered mood associated with online instructions.
Mixed-method qualitative open-ended survey [feedback for program improvement] by participants included the following suggestions: “better for patients who are done with treatment as sometimes I felt to weak or nauseous to participate fully,” “advertise this program more, because I would have joined sooner if I knew about it,” “I wish we could follow-up after the 8-week program was over,” “My job worked it out with me, but I wish this program was offered after working hours for people like me who work 9-5 jobs” and “I did see the flyers, but my own doctor didn’t bring it up, so I didn’t think it was important, maybe all doctors should recommend it.”
Discussion
Ideal study design for multimodality lifestyle-based interventions remains a challenge and may vary depending on cancer site and individual patient functionality status. We report on the acceptability of a multimodality tele-lifestyle-based survivorship pilot intervention to inform a larger prospective study. Whether diet and exercise alone play the largest role in lifestyle-contributing outcomes remains unclear; however, the addition of other pillars of wellness is unanimously reported as very important by our participants. Limitations of our study include the relatively small numbers with complete data precluding our ability to make any claims regarding benefit. However, our results provide pilot data that a multidisciplinary peri-habilitation survivorship program for gynecologic cancer survivors using a telemedicine-based platform could be acceptable (100% of those who completed, “high recommended” the program), with ~81% retention (35/43 completed at least 6-sessions). Furthermore, this short 8-week program demonstrates the potential to positively impact patients reported multiscale lifestyle scores and physical function. Notably, we found suboptimal referrals (20%; 60/300 survivors seen in that time period) to this program from within our practice Therefore, education and “buy-in” from our colleagues is crucial to increase referrals. Additionally, 600 patient traffic in hallways exposed to flyers on walls but 10 “self-referred,” we suspect that increased funding aimed at patient-centered marketing of our program may be another opportunity to increase participation. Furthermore, it is important to highlight that interest in, compliance with, and referral to like programs are likely variable per institution, geography, resources, and beliefs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mamguem Kamga A , Bengrine-Lefevre L, Quipourt V, et al Long-term quality-of-life and sexual function of elderly people with endometrial or ovarian cancer. Health Qual Life Outcomes. 2021;19:56. https://doi.org/10.1186/s 12955-021-01675-233579310 PMC 7881660 · doi ↗ · pubmed ↗
- 2Rock CL , Thomson CA, Sullivan KR, et al American cancer society nutrition and physical activity guideline for cancer survivors. CA Cancer J Clin. 2022;72:230-262. https://doi.org/10.3322/caac.2171935294043 · doi ↗ · pubmed ↗
- 3Mc Kenzie ND , Ahmad S. Impact of lifestyle interventions on gynecologic cancers: beyond diet and exercise. Am J Lifestyle Med. 2022;18:7-20. https://doi.org/10.1177/1559827622112376439184272 PMC 11339763 · doi ↗ · pubmed ↗
- 4Rippe JM. Lifestyle medicine: The health promoting power of daily habits and practices. Am J Lifestyle Med. 2018;12:499-512. https://doi.org/10.1177/155982761878555430783405 PMC 6367881 · doi ↗ · pubmed ↗
- 5Swisher AK , Abraham J, Bonner D, et al Exercise and dietary advice intervention for survivors of triple-negative breast cancer: effects on body fat, physical function, quality of life, and adipokine profile. Support Care Cancer. 2015;23:2995-3003. https://doi.org/10.1007/s 00520-015-2667-z 25724409 PMC 4624214 · doi ↗ · pubmed ↗
- 6Montagnese C , Porciello G, Vitale S, et al Quality of life in women diagnosed with breast cancer after a 12-month treatment of lifestyle modifications. Nutrients. 2020;13:136. https://doi.org/10.3390/nu 1301013633396551 PMC 7824271 · doi ↗ · pubmed ↗
- 7Kim J , Hong Y, Baek S, Lee KP, Ahn S. The synergistic effect of physical activity and nutrition to improve the quality of life in breast cancer patients: a systemic review. Phys Act Nutr. 2022;26:22-31. https://doi.org/10.20463/pan.2022.0021 PMC 992511336775648 · doi ↗ · pubmed ↗
- 8Koutoukidis DA , Beeken RJ, Manchanda R, et al Recruitment, adherence, and retention of endometrial cancer survivors in a behavioral lifestyle program: The Diet and Exercise in Uterine Cancer Survivors (DEUS) parallel randomized pilot trial. BMJ Open. 2017;7:e 018015. https://doi.org/10.1136/bmjopen-2017-018015 PMC 564012028993394 · doi ↗ · pubmed ↗