A Case Report of Salmonella sp. Endocarditis and Literature Review
Hermann Do Rego, Yoann Moeuf, Arshid Azarine, Martin Kloekner, Benoit Pilmis

TL;DR
This paper reports a rare case of Salmonella endocarditis in an elderly man and reviews other cases from 2014 to 2023, highlighting treatment approaches and outcomes.
Contribution
The paper adds a new clinical case and provides an updated literature review on Salmonella-induced endocarditis over the last decade.
Findings
Salmonella endocarditis commonly affects aortic and mitral valves, with a notable rate of prosthetic valve involvement.
Third-generation cephalosporins were the most frequently used antibiotics, with a median treatment duration of six weeks.
A 10% mortality rate was observed among treated patients, emphasizing the need for early diagnosis and intervention.
Abstract
Salmonella sp. is a rare cause of infective endocarditis (IE). We present a case of endocarditis diagnosed in an 80-year-old man who had undergone multiple aortic valve replacements and had a recurrence of Salmonella sp. bacteremia with hyperfixation on positron emission tomography (PET) scan and an aortic periprosthetic false aneurysm suggestive of a paravalvular abscess on cardiac scan. Treatment consisted of aortic valve replacement and curative antibiotic therapy with ceftriaxone, and the patient is still alive and asymptomatic on suppressive antibiotics with cotrimoxazole. We also present a review of Salmonella sp. IE in the PubMed and Google Scholar databases between 2014 and 2023. A total of 39 patients were included, including one case managed by our team. The median age was 55 years, and the most commonly involved valves were mitral and aortic in 43% and 41% of cases,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
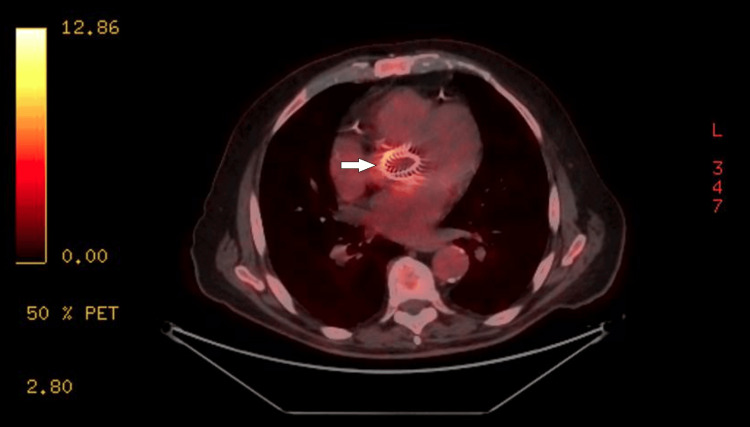 Figure 1
Figure 1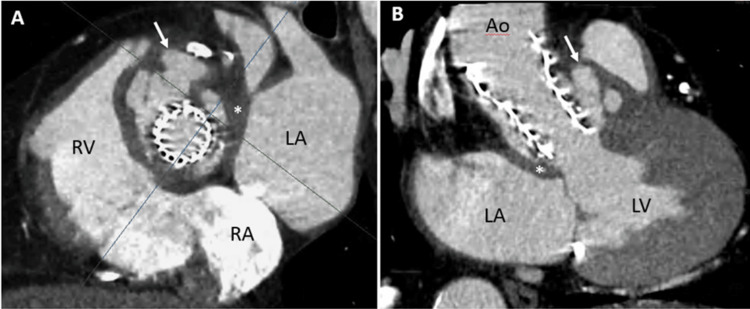 Figure 2
Figure 2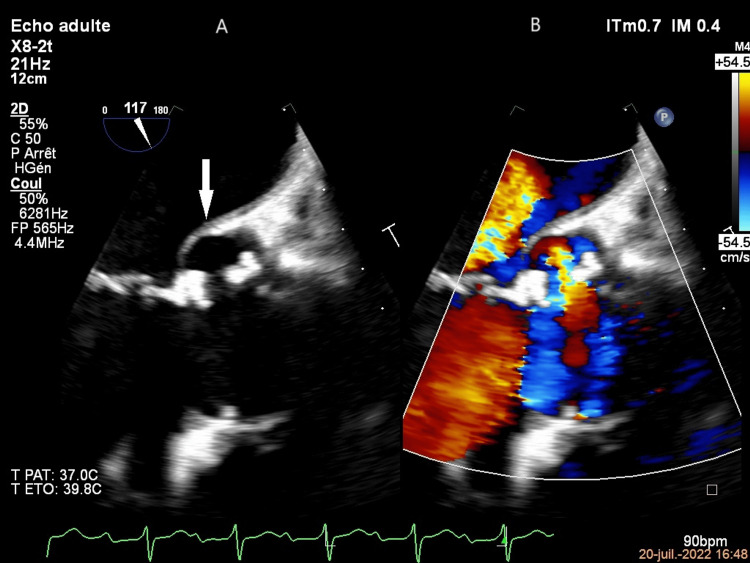 Figure 3
Figure 3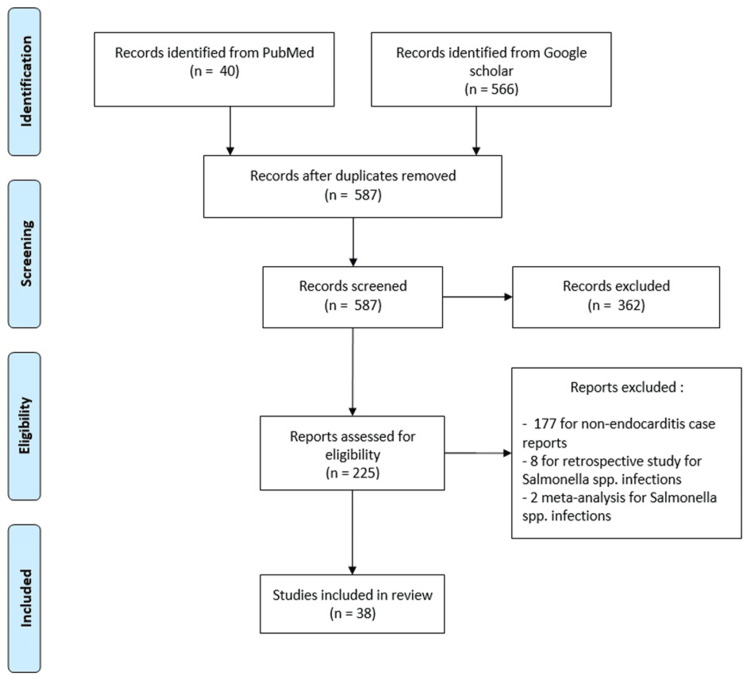 Figure 4
Figure 4| Studies | Age (years) | Sex | Comorbidities | Germ | Cardiac involvement | Elements of the medical history | Antibiotic/duration | Cardiac surgery performed | Mortality under treatment |
| Gutiérrez Macías et al. 2014 [ | 82 | Man | COPD. AF. Mitral valve prolapse |
| Native mitral | Asthenia, anorexia, fever, inflammatory syndrome. Positive blood cultures and urine cultures. Severe mitral and tricuspid regurgitation. 12 mm mitral vegetation | Ceftriaxone 6 weeks | No | No |
| Ortiz et al. 2014 [ | 73 | Woman | Asthma. Arterial hypertension. Bioprosthetic aortic valve and mitral valve mechanics |
| Mechanical mitral. Biological aortic valve with abscess | Nausea, diarrhea, fever, septic shock, respiratory distress. Positive blood cultures, 11 mm mitral vegetation, aortic valve abscess | Levofloxacin (0.75 mg/kg/d). Then gentamicin (0.6 mg/kg 3 times daily) and aztreonam (20 mg/kg 3 times daily) | No | Yes |
| Dar et al. 2014 [ | 20 | Man | Rheumatic fever |
| Native mitral | Fever, vomiting, dyspnea, Osler's nodule, subungual hemorrhage, mitral and tricuspid murmur, splenomegaly. Inflammatory syndrome. Positive blood cultures, 5x7 mm mitral vegetation | Ceftriaxone 6 weeks. Chloramphenicol 4 weeks | No | No |
| Egodage et al. 2015 [ | 40 | Man | 0 |
| Native mitral | Fever, chills, headache, cough, hepatomegaly. Inflammatory syndrome. Positive blood cultures. 0.6x0.5 cm mitral vegetation | Ceftriaxone (3 g daily) | No | No |
| Jeyakanth et al. 2015 [ | 66 | Woman | Diabetes mellitus. Bronchial asthma. Bioprosthetic aortic valve |
| Aortic bioprosthesis. Native tricuspid | Fever, chills, diarrhea, nausea, hepatomegaly. Inflammatory syndrome, hepatic cytolysis. Positive blood cultures. Aortic vegetation 11×10 mm. Tricuspid valve vegetation 21×12 m. Right ruptured sinus of Valsalva, aneurysm and fistulous communication between the left ventricular outflow track and right atrium | Ceftriaxone (2 g/day) 3 months | No | No |
| Palangasinghe et al. 2015 [ | 55 | Man | Diabetes |
| Native aortic | Fever, headache, anorexia, nausea, splenomegaly, inflammatory syndrome. Positive blood cultures. Vegetations 5x4 mm | Ceftriaxone 4 weeks. Gentamicin 2 weeks | No | Yes |
| Blusztein and Strathmore 2016 [ | 47 | Man | Heart block. Pacemaker |
| Pacemaker lead | Fever, pacemaker site tenderness. Septic shock. Positive blood cultures | Ceftriaxone | Yes | No |
| García et al. 2016 [ | 65 | Man | Bronchopulmonary cancer on chemotherapy |
| Native aortic | Fever, bilateral coxarthralgia. Inflammatory syndrome. Positive blood cultures and hip joint culture fluid. Addition image of aortic valve on TTE | Piperacillin-tazobactam and then cotrimoxazole and amikacin and then ertapenem 6 weeks of treatment and then ertapenem as suppressive treatment | No | No |
| Stasev et al. 2017 [ | 25 | Woman | Systemic lupus (glomerulonephritis, immune thrombocytopenia, cerebrovascular disease) treated with corticosteroids |
| Native mitral | Fever, chills, dyspnea, alveolar condensation, splenic embolus. Inflammatory syndrome. Positive blood culture. Mitral vegetation 15 mm | Ceftriaxone | Yes | No |
| Huertas et al. 2017 [ | 50 | Man | Chronic hypertension. Diabetes. Myocardial infarction. Heart failure |
| Mural endocarditis | Fever, diarrhea, abdominal pain, positive blood culture, gangrenous cholecystitis. Septic and cardiogenic shock, 5 mm mural thrombus, ventricular aneurysm | Not described | Yes | No |
| Laganà et al. 2017 [ | 74 | Woman | AF. Arterial hypertension. Psoriasis |
| Mural endocarditis | Fever, emesis, and diarrhea. Ventricular fibrillation with cardiac arrest. Culture of cardiac autopsy | 0 | 0 | Yes |
| Lam et al. 2018 [ | 55 | Man | Congenital heart disease. Mechanical aortic and mitral prosthesis. Aortic tube graft. Pacemaker |
| Mechanical mitral and aortic with abscess | Fever, lipothymia. Positive blood culture. Mitral (1.1x0.6 cm) and aortic (0.9x1.1 cm) vegetation. Peri-aortic abscess | Ceftriaxone 6 weeks. Cotrimoxazole (800/160 mg daily) as suppressive treatment | No | No |
| Piyasiri et al. 2017 [ | 25 | Man | 0 |
| Native mitral | Fever, headache. Positive blood culture. Mitral vegetation | Ceftriaxone 4 weeks (3 g daily). Then azithromycin (500 mg daily) 1 week | No | No |
| Robson et al. 2018 [ | 20 | Man | 0 |
| Native mitral | Previous bacteremia. Fever, asthenia, headache, abdominal pain, inflammatory syndrome. Positive blood and stool cultures. Mitral vegetation | Ceftriaxone 6 weeks (2 g/d). Then ciprofloxacin (500 mg/d) 6 weeks | No | No |
| Gandhi et al. 2018 [ | 64 | Man | AF. Mechanical aortic prosthesis |
| Mechanical aortic | Previous bacteremia. Dyspnea, acute pulmonary edema. Severe aortic insufficiency, periprosthetic leak, proximal aortic dilatation, right aorto-ventricular fistula. Positive blood culture | Ceftriaxone 6 weeks | Yes | No |
| Dickter et al. 2019 [ | 69 | Man | Myelofibrosis complicated by leukemia, allograft with graft-versus-host disease. Pacemaker. Patent foramen ovale with septal implant. Abdominal aortic aneurysm |
| Native mitral | Previous bacteremia. Fever, diarrhea, and abdominal pain. Positive blood and stool cultures. 4 mm mitral vegetation | Ceftriaxone and then amoxicillin/clavulanic acid 3 weeks. Break 1 week. Then cotrimoxazole 1 month. Break 1 week. Then ceftriaxone (2 g/d) 6 weeks | No | No |
| Youssef et al. 2019 [ | 36 | Woman | HIV (17 CD4/m3 and viral load at 5.6 log) |
| Eustachian valve | Fever, chills, night sweats, dyspnea, cough, diarrhea. Positive blood culture. Eustachian valve vegetations 6.6x4 mm | Ceftriaxone and then ciprofloxacin 5 weeks | No | No |
| Hussain and Khalil 2019 [ | 68 | Man | Diabetes. Coronary artery disease. Lung cancer undergoing radiotherapy and chemotherapy |
| Native aortic | Abdominal pain, inflammatory syndrome. Positive blood culture. Aortic mycotic aneurysm. Vegetations on aortic valve | Ceftriaxone | No | No |
| Tran et al. 2020 [ | 38 | Man | HIV (50 CD4/mm3 and viral load at 6.23 log) |
| Native mitral | Diarrhea, recurrent fever, abdominal pain. Splenomegaly, pancytopenia. Cardiogenic shock. Positive blood culture. Nodular mitral vegetation | Not described | No | Not described |
| Pervin et al. 2020 [ | 62 | Woman | Chronic hypertension. Diabetes. Dyslipidemia. Arteritis of the lower limbs. Kidney transplant |
| Native mitral | Fever, confusion, inflammatory syndrome, abdominal pain. Positive blood culture and urine culture positive. Mitral vegetation 0.3x0.3 cm | Ceftriaxone 8 weeks. Amoxicillin as suppressive treatment | No | No |
| Kitazawa et al. 2020 [ | 76 | Man | Gastric cancer. Rheumatic fever |
| Mechanic mitral | Fever, inflammatory syndrome. Left psoas abscess. Hemolytic anemia. Positive blood culture, urine and stool culture. Mitral vegetation 8x6 mm, paravalvular mitral regurgitation | Ciprofloxacin and cefotaxime. Then levofloxacin and ceftriaxone (2 g/day) 14 weeks | Yes | No |
| Chan et al. 2020 [ | 64 | Man | HIV-AIDS stage |
| Native pulmonary | Fever, dyspnea, chest pain, heart murmur. Bilateral pulmonary embolism, pulmonary infarction, positive blood culture, 10 mm pulmonary vegetation | Ceftriaxone 6 weeks | No | No |
| Rojas et al. 2020 [ | 48 | Man | Acute myeloid leukemia |
| Native aortic | Fever, chills, dyspnea, heart murmur. Inflammatory syndrome. Positive blood culture. Aortic vegetation 12 mm | Levofloxacin 4 weeks | No | No |
| Dhayhi et al. 2021 [ | 7 | Woman | Sickle cell disease |
| Junction of the right atrium and vena cava | Fever, jaundice, abdominal pain, dyspnea. Hepatosplenomegaly. Inflammatory syndrome. Positive blood culture. Two vegetations of 7 and 8 mm | Cefotaxime and ciprofloxacin 6 weeks with amikacin 2 weeks | No | No |
| Connolly et al. 2021 [ | 50 | Woman | Rheumatic fever. Mitral and aortic mechanical valve replacement. PAH. Hypothyroidism. COPD. Arteritis of the lower limbs |
| Mechanical mitral | Previous diarrhea. Fever, chills, cough, dyspnea, nausea, vomiting, weight loss. Inflammatory syndrome, anemia. Positive blood culture. Long, filamentous, mobile vegetation on mitral valve. Fixation of mitral valve on PET scan | Ceftriaxone and ciprofloxacin 6 weeks. Amoxicillin as suppressive treatment | No | No |
| Mishra et al. 2021 [ | 50 | Man | Chronic alcoholism |
| Native aortic | Fever, chills, chest pain. Inflammatory syndrome. Positive blood culture. Aortic vegetation 2.5x2.7 mm | Piperacillin/tazobactam then cefepime (4 g daily) and levofloxacin (750 mg daily) 6 weeks | No | No |
| Rzucidło-Resil et al. 2022 [ | 39 | Woman | Barlow's disease |
| Native mitral and aortic | Fever. Inflammatory syndrome. Splenic embolus. Positive blood culture. Mitral and aortic vegetation | Levofloxacin and cotrimoxazole 6 weeks | Yes | No |
| Alhamadh et al. 2022 [ | 56 | Woman | Chronic hypertension. Diabetes. AF. Rheumatic fever. Mechanical mitral and aortic replacement |
| Mechanical aortic. Aortic root abscess | Fever, chills, dyspnea, cough, edema of the lower limbs. Inflammatory syndrome, hepatic cytolysis. Positive blood culture. Splenic embolus. Periaortic collection and pseudoaneurysm in the aorta on cardiac scan. Aortic valve and aortic root fixation on PET scan | Ceftriaxone | Yes | No |
| Allard et al. (2022) [ | 36 | Woman | Chronic alcoholism. Addiction to methamphetamine |
| Native tricuspid | Coma, pleuropneumonia, shock, positive blood and pleural fluid cultures, flaming hemorrhages, tricuspid vegetation 18 mm | Levofloxacin 6 weeks | No | No |
| Brenneman et al. 2022 [ | 60 | Man | AF. Diabetes. Cirrhosis. Pacemaker |
| Pacemaker lead | Previous bacteremia. Fever, chills, abdominal pain. Positive blood culture. Vegetation on 10 mm lead | Ciprofloxacin 1 week. Then ertapenem (1 g/d) 4 weeks | Yes | No |
| Basyal et al. 2023 [ | 65 | Man |
|
| Mechanical mitral | Diarrhea, fever, septic shock, renal failure, 15 mm vegetations. Positive blood culture | Ceftriaxone | Yes | No |
| Kitaya et al. 2023 [ | 66 | Man | Chronic hypertension. AF. Chronic renal failure. Aortic valve replacement |
| Mechanical aortic. Aortic ring abscess | Previous bacteremia and gastroenteritis. Fever, para-prosthetic leak, aortic ring abscess. Positive blood culture | Meropenem (3 g/d) 1 week. Ceftriaxone (2 g/d) 6 weeks. Cotrimoxazole (800/160x2/d) as suppressive treatment | Yes | No |
| Winicki et al. 2023 [ | 57 | Man | Polyintoxication (alcohol, tobacco, methamphetamines, cocaine, marijuana) |
| Native aortic | Chills, nausea, diarrhea, acute renal failure, positive blood culture. Small vegetations | Ceftriaxone and levofloxacin 6 weeks | No | No |
| Zaghdoudi et al. 2023 [ | 9 months | Boy (man) | Operated congenital heart disease (coarctation of the ductus arteriosus and coarctation of the aortic arch). Postoperative endocarditis |
| Pulmonary patch | Fever, tachycardia, systolic murmur, hepatomegaly, inflammatory syndrome. Positive blood culture. Pulmonary patch stenosis with vegetations and pulmonary insufficiency | Amoxicillin (200 mg/kg per day) 6 weeks and gentamicin (5 mg/kg per day) 5 days | No | No |
| Murray et al. 2023 [ | 26 | Man | HIV. Hepatitis C. Polyintoxication (heroin, methamphetamine, cocaine, cannabis) |
| Native mitral and tricuspid | Fever, cough, dyspnea, polypnea, mitral and tricuspid systolic murmurs, inflammatory syndrome, hepatic cytolysis. Positive blood culture, mitral and tricuspid valve perforation, severe valvular regurgitation | Amoxicillin and ceftriaxone 6 weeks | Yes | No |
| George et al. 2023 [ | 52 | Woman | Rheumatic fever. Mitral bioprosthesis. Pacemaker. Heart failure |
| Mitral bioprosthesis | Fever, asthenia, diarrhea. Septic and cardiogenic shock. Positive blood and stool cultures. Mitral valve dehiscence | Not described 6 weeks | Yes | No |
| van Kruijsbergen et al. 2023 [ | 80 | Man | TAVI. COPD. Chronic renal failure |
| Aortic bioprosthesis | Fever, abdominal pain, diarrhea. Inflammatory syndrome, acute on chronic renal failure, moderate aortic insufficiency, TAVI fixation on PET scan. Positive blood culture | Ceftriaxone 6 weeks | Yes | Yes |
| Zahoor et al. 2023 [ | 25 | Man | 0 |
| Native aortic | Fever, chills, night sweats, cough, dyspnea, aortic murmur, acute pulmonary edema, aortic vegetations, severe aortic insufficiency, moderate mitral insufficiency. Positive blood culture | Ceftriaxone (2 g/d) and meropenem (2 g/d) 3 weeks | No | No |
| Our case | 80 | Man | History of endocarditis. Aortic bioprosthesis. Cold agglutinin disease. AF. Prostate cancer |
| Aortic mechanical. Circulating aortic abscess | Previous bacteremia. Fever, rhinorrhea, dyspnea. Inflammatory syndrome. Positive blood culture. TAVI fixation on PET scan. Circulating abscess on TTE and coroscanner | Ceftriaxone (2 g/day) 12 weeks. Cotrimoxazole (800/160 mg daily) as suppressive treatment | Yes | No |
| Patients' characteristics (n=39) | |
| Median age, years (interquartile range) | 55 (37-65) |
| Woman, n (%) | 11 (28) |
| Immunodepression, n (%) | 9 (23) |
| Previous bacteremia, n (%) | 6 (15) |
| Digestive signs, n (%) | 21 (54) |
| Prosthetic valve endocarditis, n (%) | 12 (31) |
| Aortic valve, n (%) | 16 (41) |
| Mitral valve, n (%) | 17 (43) |
| Polyvalvular endocarditis, n (%) | 5 (13) |
| Abscess, n (%) | 5 (13) |
| Extra-valvular endocarditis, n (%) | 5 (13) |
| Positive blood culture, n (%) | 38 (97) |
| Embolic complications, n (%) | 7 (18) |
| Germ, n (%) | |
|
| 7 (18) |
|
| 16 (41) |
|
| 3 (8) |
| Type of species not specified | 7 (18) |
| Others | 6 (15) |
| Cardiac surgery | 14 (36) |
| Mortality under treatment | 4 (10) |
| Patients' antibiotic therapy (n=39) | |
| Monotherapy (n, %) | 23 (59) |
| Curative antibiotic therapy (n, %) | |
| Levofloxacin/ciprofloxacin | 12 (31) |
| Ceftriaxone/cefotaxime | 26 (67) |
| Cefepime | 1 (2.5) |
| Meropenem/ertapenem | 4 (10) |
| Piperacillin-tazobactam | 2 (5) |
| Aztreonam | 1 (2.5) |
| Chloramphenicol | 1 (2.5) |
| Cotrimoxazole | 4 (10) |
| Azithromycin | 1 (2.5) |
| Gentamicin/amikacin | 5 (13) |
| Duration of treatment, weeks (interquartile range) | 6 (6-6) |
| Suspensive treatment (n, %) | |
| Cotrimoxazole | 3 (8) |
| Amoxicillin | 2 (5) |
| Ertapenem | 1 (2.5) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Salmonella and Campylobacter epidemiology · Infectious Aortic and Vascular Conditions
Introduction
Salmonella spp. are responsible for a variety of human infections, including typhoid fever and non-typhoidal salmonellosis. Typhoid fever is responsible for 22 million cases per year and 200,000 deaths per year, while the incidence of non-typhoidal salmonellosis is 93.8 million cases per year with 155,000 deaths per year worldwide [1,2].
These species can cause simple gastroenteritis or bloodstream infections affecting multiple organs (endovascular infections, osteoarticular infections, dermo-hypodermatitis, urinary tract infections, etc.). They may also be responsible for 30% of bloodstream infections in Africa, but their incidence appears to be low in developed countries [3,4].
Endovascular lesions such as aortitis are typical and responsible for high mortality [5]; however, infective endocarditis (IE) caused by Salmonella spp. is a rare disease described only in case reports in the medical literature, and there are still no prospective or retrospective studies on the subject.* *
Salmonella sp. is estimated to represent 0.03% of cases of IE, compared with Staphylococcus aureus in 31% of cases or oral streptococci in 17% of cases, if we refer to certain international prospective cohorts, in particular the International Collaboration on Endocarditis (ICE) cohort (2000-2005) and the GAMES cohort (2008-2018) [6,7].
The most recent reviews on Salmonella endocarditis are the study by Cheng et al., published in 2016, which included 87 patients from 1976 and 2014 [8] and the study by Kitazawa et al., published in 2020, which included 38 patients between 1947 and 2019. Four of them were beyond 2012 [9].
However, these studies followed patients over a long period of time and did not take into account improvements in medical management over time. These include early diagnosis using clinical scores such as the Duke criteria, improvements in echocardiography equipment, the use of computed tomography (CT) scanners to better characterize embolic complications and positron emission tomography (PET) scanners to identify infectious sites or prosthesis infections, and better microbiological identification using molecular biology techniques. Treatment has also been optimized with the identification of better antibiotic regimens and early identification of patients who could benefit from early valve replacement surgery [10]. In addition, new guidelines (European and American) have been published in 2015 and 2023.
The aim of this review is to report the case of a patient who had Salmonella endocarditis in our center and then to review the most recent cases in the medical literature.
Case presentation
We present the case of an 80-year-old patient with a history of IE of the native aortic valve in 1992 but no available microbiological data. He underwent bioprosthetic aortic valve replacement for severe aortic stenosis in 2012. In 2018, he presented with a second episode of IE of the bioprosthetic aortic valve, which was documented as Enterococcus faecalis. Following the degeneration of the aortic bioprosthesis, he also underwent a valve-in-valve transcatheter aortic valve implantation (TAVI) in 2019 due to his age. His past medical history includes hemolytic anemia due to cold agglutinin disease, atrial fibrillation on curative anticoagulation for stroke prevention, and localized prostate cancer treated by prostatectomy.
On May 5, 2002, the patient presented with chills and asthenia, without fever or other associated symptoms, with a biological inflammatory syndrome (his C-reactive protein (CRP) level was 61 mg/L). As he had a history of prosthetic heart valves, he was admitted to the cardiology department. Three sets of peripheral blood cultures obtained between May 6 and May 7 and separated by at least two hours were positive for Salmonella enterica subsp. enterica serovar Dublin. Antibiotic susceptibility testing revealed resistance to amoxicillin, ticarcillin, and piperacillin. A transthoracic echocardiogram (TTE) and cardiac CT scan showed no evidence of IE, but the patient refused to undergo a transesophageal echocardiogram (TEE) because of previous discomfort. A thoracoabdominopelvic CT scan was performed to assess the extent of the infection and identify a portal of entry, but no deep-seated infection was found. After seven days of treatment with ceftriaxone, the clinical course and inflammatory syndrome were favorable. Ten pairs of blood cultures were negative between May 8 and May 16, and the patient was discharged from the hospital.
On June 2, 2022, the patient presented with fever, chills, rhinorrhea, and exertional dyspnea, without other functional signs, and was referred to the emergency department and then admitted to the internal medicine department where he was diagnosed with biological inflammatory syndrome (his CRP level was 133 mg/L and his nasopharyngeal polymerase chain reaction (PCR) severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was negative). Blood cultures obtained on June 3 and June 4 were again positive for Salmonella spp. (same antibiogram as serovar as before), and antibiotic treatment with ceftriaxone was started on June 4. Given the recurrence of Salmonella bacteremia and the presence of a prosthetic heart valve, a PET scan was performed. It showed circumferential hypermetabolism of the bioprosthesis (SUV max=7) predominantly at the left lateral border without evidence of distant emboli (Figure 1).
PET scanCircumferential hyperfixation of the aortic bioprosthesis (white arrow)PET: positron emission tomography
The patient was transferred to the cardiac intensive care unit (CICU) for close monitoring due to the development of type 1 atrioventricular block. He was hemodynamically stable. A TTE showed a periprosthetic anechoic image without severe valvular insufficiency, and a cardiac CT scan revealed a 28x19 mm false aneurysm associated with a 5 mm pertussis in the left ventricular (LV) outflow tract (left anterolateral), which in context appeared to be a circulating detergent paravalvular abscess (Figure 2).
Cardiac CT scanAortic periprosthetic false aneurysm (white arrow) suggestive of a circulating abscess. (A) Aortic cross-sectional plane showing a multifocal circulating periprosthetic image around the aortic root. (B) Reformatted three-chamber view showing the expansion of the circulating mass during systoleCT: computed tomography; RV: right ventricle; RA: right atrium; LA: left atrium; Ao: ascending aorta
Due to the paravalvular abscess, it was decided to proceed with aortic valve replacement with bioprosthesis and abscess debridement on June 15; intraoperative bacteriological samples were negative. The patient improved with apyrexia and reduction of the inflammatory syndrome, with the first negative blood culture on June 8 and subsequent blood cultures until June 25.
Antibiotic therapy with ceftriaxone was continued for six weeks, but a TEE performed on July 20 revealed three large false aneurysms around the aortic annulus. All three were at risk of rupture and in communication with the left ventricle, but had no internal echogenic features (Figure 3); the same lesions were seen on the cardiac scan on July 20. Given the high risk of surgical complications, it was decided not to perform a second operation and to continue antibiotic therapy for six weeks. At the end of the curative treatment, the cardiac scan showed the presence of periaortic abscesses of almost the same size as on the July 20 cardiac scan, but there was no increase in fluorodeoxyglucose (FDG) uptake on the PET scan.
TEE mid-esophageal long-axis view(A) TEE without Doppler color showing the abscess (white arrow). (B) TEE with Doppler color showing the fistulae between the abscess and the aortic rootTEE: transesophageal echocardiogram
Due to the persistence of the false aneurysm and the presence of material, suppressive antibiotic therapy with cotrimoxazole was chosen, given the resistance to amoxicillin and the low risk of acquiring co-drug resistance compared to quinolones. This will be reassessed later depending on the patient's progress.
As Salmonella is an Enterobacteriaceae that commonly causes gastrointestinal infections, it was decided to perform a colonoscopy, which revealed extensive uncomplicated diverticulosis and multiple subcentimeter polyps. A mucosectomy was performed on four subcentimeter polyps, and pathology revealed tubular adenomas with low-grade dysplasia. According to gastroenterology, this could be the etiology of the bacteremia.
Discussion
This case study presents the case of an 80-year-old patient with endocarditis, manifested by a recurrence of *Salmonella enterica *subsp. *enterica *serovar Enteritidis and complicated by a circulating abscess around the aorta. The patient required surgical intervention, including valve replacement and drainage of the abscess, followed by prolonged antibiotic therapy. It is unclear whether the recurrence of bacteremia was related to the onset of endocarditis or whether it was a recurrence of the initial bacteremia, but the first hypothesis seems more likely because it was an early recurrence of bacteremia, the PET scan did not show any site of infection other than the perivalvular abscess, and the patient had no functional digestive signs, but one study shows that these are not always present in bloodstream infections with Salmonella spp. [4].
In contrast to infectious vasculitis such as aortitis, endocarditis caused by Salmonella spp. is a rare disease, with only a limited number of case reports in the medical literature. We performed a literature review of Salmonella sp. endocarditis cases published from January 2014 to December 2023 by conducting a bibliographic search in the PubMed and Google Scholar databases using the following keyword: "endocarditis salmonella".
After a search of the PubMed and Google Scholar databases, 38 cases were retained [11-47], and exclusions are detailed in the flowchart (Figure 4).
Flowchart
In addition to the patient reported in the observation, the review includes 39 patients whose main characteristics are detailed in Table 1.
The median age was 55 years (interquartile range (IQR): 37-65). The majority of patients were male (72%), of whom 23% were immunosuppressed (Table 2).
In the medical history, six (15%) patients presented with a first episode of treated bacteremia, classifying the endocarditis as a recurrent infection, and 21 (54%) patients presented with gastrointestinal symptoms (nausea, vomiting, diarrhea, or abdominal pain) before or at the time of endocarditis diagnosis. All blood cultures were positive except for one case report. This was a cardiac autopsy culture because the patient died before blood could be obtained (Table 2).
The most commonly involved valves were the mitral and aortic valves in 41% (16/39) and 43% (17/35) of cases, respectively. Twelve (31%) patients had prosthetic valve endocarditis. Five percent (13/39) of endocarditis cases were complicated by perivalvular abscesses. Embolic complications occurred in 18% of cases (Table 2).
Salmonella enterica subsp. enterica serovar Enteritidis was the main causative organism in 41% (16/39) of patients, while 18% (7/39) were associated with typhoidal Salmonella, either serovar Typhi or Paratyphi (Table 2).
Treatment was medical in 64% (25/39) of cases and medico-surgical in 36% (14/39) (Table 2). The most commonly prescribed antibiotic was a third-generation cephalosporin in 67% (26/39) of cases. Combination therapy was prescribed in 41% of cases. Seventy-five percent of patients (8/12) who had received quinolones were on combination therapy. Nineteen percent (5/26) of patients who had received a third-generation cephalosporin were on combination therapy. The median duration of treatment was six weeks (IQR: 6-6), but in 13 clinical cases, the duration was not described. Suppressive therapy was prescribed in 15% of cases (Table 3). The reasons for cardiac surgery were severe vascular insufficiency in six cases, periprosthetic collection or abscess in three cases, high embolic risk in two cases, pacemaker removal in two cases, and the presence of a pseudoaneurysm in two cases.
Intra-hospital or follow-up mortality was not described but mortality during medical management was 10% (Table 2). The majority of deaths in case reports were related to disease progression and/or surgical complications.
A total of 38 case reports were identified through an exhaustive search of the PubMed and Google Scholar databases between 2014 and 2023, highlighting the rarity of the disease, although there may be non-publication bias.
The population appears to be similar to other cohorts [48,49], with the majority of men having a median age of approximately 55 years and prosthetic valve endocarditis occurring in 31% of cases. As in the reviews by Cheng et al. and Kitazawa et al. [8,9], the main valve involved was the mitral valve in 43% of the cases.
Salmonella sp. is a bacterium that causes gastrointestinal infections that may be complicated by bacteremia and secondary foci. However, gastrointestinal symptoms such as diarrhea were found in just over half of the cases, and bacteremia treated before the endocarditis episode was found in 15% of cases, suggesting that endocarditis was responsible for the recurrence.
Typhoidal Salmonella was more likely to cause endocarditis in the absence of comorbidities, and of the four patients with no medical history, all were infected with "Typhi" or "Paratyphi" serovars. These serovars are the most virulent in the genus Salmonella due to their strict human carriage and the presence of a polysaccharide capsule that protects the bacteria from phagocytosis. Typhoidal Salmonella infections could benefit from a more aggressive strategy, such as high-dose antibiotics or dual therapy. However, there are no studies demonstrating this, and in our study, we did not show that typhoidal Salmonella caused more deaths, but the number of cases was low (one death, i.e., 14%, compared with two cases of non-typhoidal Salmonella, i.e., 12.5%).
The main antibiotics used were third-generation cephalosporins and quinolones, administered as monotherapy in the majority of cases, with the duration of curative treatment ranging from three to 16 weeks, with a median duration of six weeks. The reason for extending treatment beyond six weeks was not justified in all trials, but there did not seem to be an association with complications in the observations in the case reports. With only one death observed with monotherapy (4%) compared with two deaths (16%) with combination therapy, combination therapy did not appear to be more effective than monotherapy. Combination therapy was considered when several antibiotics were used simultaneously (for aminoglycosides for more than five days). Suppressive antibiotic therapy was more likely to be used in patients with immunosuppression or mechanical prostheses. With the exception of the recommended combination therapy, these observations are consistent with European and American guidelines for gram-negative endocarditis. It should be noted that only two cases of extended-spectrum β-lactamase (ESBL) were reported, resulting in treatment with carbapenems.
Due to the retrospective nature of the study and the small number of patients, it is not possible to draw conclusions about the optimal antibiotic regimen and duration of treatment.
Cardiac surgery was performed in 36% of patients, which is lower than the 50% usually seen in cohorts. With the exception of one case, there were no deaths among patients who underwent valve replacement. We have no explanations or hypotheses to explain the difference in surgery rates in our review, but this underuse of cardiac surgery needs testing in a larger study.
The mortality rate in our study was 10%, which remains lower than that observed in the studies of Cheng et al. [8] and Kitazawa et al. [9], which reported rates of 42.5% and 45%, respectively, when considering cases reported since at least 1946. However, if the period from 2003 to 2014 is considered in the Cheng et al. study, the mortality rate decreases to 13.3%. Furthermore, the EURO-ENDO cohort study [45] reported an in-hospital mortality rate of 17.1%. These differences in mortality are probably due to improvements in the management of endocarditis over time, whether in terms of diagnosis, antimicrobial therapy, or surgery, for example, a European study estimated that early cardiac surgery reduced in-hospital mortality over time [10,50].
The main limitation is that the mortality described in previous reviews [8,9] and our own is based on publishers' reporting, with differences in the definition of mortality, including pre-treatment mortality, end-of-treatment mortality, or mortality at a distance during follow-up. It is also possible that this mortality is underestimated due to possible publication bias, for which the only corrective measure is to establish a prospective cohort over time or to maintain a registry.
Because of the many biases involved in reviewing case reports, we did not perform statistical tests. The observations from this review are purely exploratory, and we hope that they will be used to guide prospective studies or randomized controlled trials, in particular, to determine the optimal duration of treatment, whether to opt for monotherapy or dual therapy, and whether to resort to cardiac surgery.
Conclusions
Endocarditis caused by Salmonella spp. is a rare cardiovascular infection, as this genus is responsible for gastrointestinal disease. If the bacteremia is recurrent or persistent, an echocardiogram (TTE or TEE) should be performed in search of endocarditis, especially if the patient has a prosthetic heart valve. Treatment consists of a course of antibiotics for at least six weeks, including beta-lactam antibiotics (penicillins, cephalosporins) in combination therapy as recommended by guidelines (the European Society of Cardiology and American Heart Association) for gram-negative bacillary endocarditis. Although combination therapy does not appear to improve prognosis in our review, the level of evidence does not allow us to conclude one way or the other. The indication for valve replacement must also be based on guidelines. Compared with previous reviews, our review shows a low mortality rate during treatment and a low need for cardiac surgery. These observations in our review need to be confirmed in a prospective study, as well as the optimal duration of treatment and the use of combination therapy and cardiac surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salmonella: a review on pathogenesis, epidemiology and antibiotic resistance Front Life Sci Eng SK Pusparajah P Ab Mutalib NS Ser HL Chan KG Lee LH 28429382015
- 2Epidemiology, clinical presentation, laboratory diagnosis, antimicrobial resistance, and antimicrobial management of invasive Salmonella infections Clin Microbiol Rev Crump JA Sjölund-Karlsson M Gordon MA Parry CM 9019372820152618006310.1128/CMR.00002-15PMC 4503790 · doi ↗ · pubmed ↗
- 3Community-acquired bloodstream infections in Africa: a systematic review and meta-analysis Lancet Infect Dis Reddy EA Shaw AV Crump JA 4174321020102051028210.1016/S 1473-3099(10)70072-4PMC 3168734 · doi ↗ · pubmed ↗
- 4A population-based study on the incidence, risk factors, and outcome of Salmonella bloodstream infections in South Sweden 2012-2022 Infect Dis Ther Björklund L Mattisson Y Bläckberg A Sunnerhagen T Ljungquist O 5015191320243839350310.1007/s 40121-024-00929-y PMC 10965858 · doi ↗ · pubmed ↗
- 5Risk factors for bacteraemia and endovascular infection due to non-typhoid Salmonella: a reappraisal QJM Hsu RB Lin FY 8218279820051620382510.1093/qjmed/hci 126 · doi ↗ · pubmed ↗
- 6Non-HACEK gram-negative Bacillus endocarditis Ann Intern Med Morpeth S Murdoch D Cabell CH 82983514720071808705310.7326/0003-4819-147-12-200712180-00002 · doi ↗ · pubmed ↗
- 7Non-HACEK gram negative bacilli endocarditis: analysis of a national prospective cohort Eur J Intern Med Calderón Parra J De Castro-Campos D Muñoz García P 71789220213398039510.1016/j.ejim.2021.04.021 · doi ↗ · pubmed ↗
- 8Salmonella infective endocarditis J Microbiol Immunol Infect Cheng WL Li CW Li MC Lee NY Lee CC Ko WC 3133204920162588248910.1016/j.jmii.2015.02.659 · doi ↗ · pubmed ↗