Diffuse large B-cell lymphoma presenting as acute adrenal hemorrhage
Fabio Torres, Uriel Suárez, Paola Pizano

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
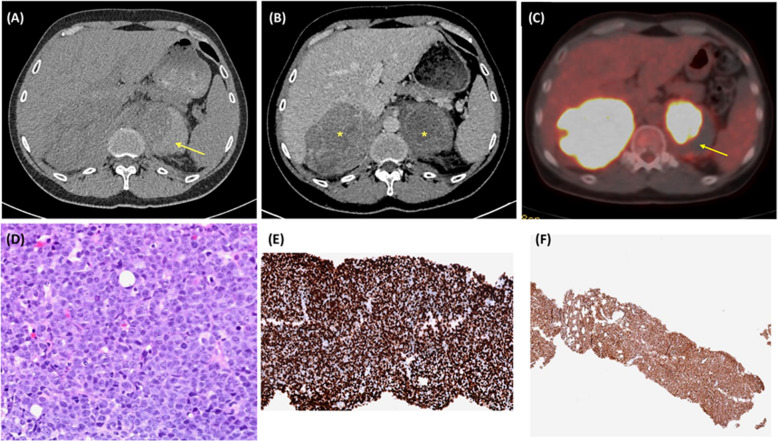 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension · Lymphoma Diagnosis and Treatment
Figure 1. (A) Transverse non-contrast abdominal computed tomography (CT) with a hyperdense content within the left adrenal gland (yellow arrow) secondary to adrenal bleeding. (B) Transverse contrast-enhanced abdominal CT with a massive enlargement of adrenal glands (asterisks). (C) Positron emission tomography-CT with increased fluorodeoxyglucose (FDG) uptake by adrenal glands suggestive of lymphoma (yellow arrow shows a zone with decreased FDG uptake due to acute adrenal bleeding). (D) Hematoxylin and eosin staining of right adrenal biopsy. This section did not include zones with active adrenal hemorrhage (hematoxylin–eosin staining × 20). (E–F) MYC (× 10) and MUM1 (× 2) immunohistochemistry
Case presentation
A 45-year-old man presented to the emergency department with a 1-day history of abdominal pain in the left flank and vomiting. No hypotension, rebound tenderness, or hepatosplenomegaly was observed. Laboratory studies revealed elevated levels of lactate dehydrogenase (LDH; 523 IU/L) and low hemoglobin (11·9 g/dL). Abdominal computed tomography (CT) revealed bulky adrenal masses with left adrenal hemorrhage (AH; Fig. 1A and B). No lymphadenopathy was observed. Positron emission tomography-CT revealed avid fluorodeoxyglucose (FDG) adrenal lesions and a zone with decreased FDG uptake due to acute AH (Fig. 1C). An adrenal biopsy revealed diffuse growth of large-sized atypical lymphoid cells with irregular nuclei, vesicular chromatin, and scanty cytoplasm (Fig. 1D). The immunostaining was positive for CD20 and BCL2. MYC and MUM expression were observed in approximately 100% of the cells (Fig. 1E and F) without CD10. The final diagnosis was diffuse large B-cell lymphoma, subtype activated B-cell-like. The abdominal pain improved with rituximab, cyclophosphamide, hydroxydaunorubicin, oncovin, and prednisone treatment.
Lymphoma is a differential diagnosis of acute abdominal pain in patients with elevated LDH levels and adrenal bleeding. In most patients with AH, the diagnosis is made incidentally using imaging tests [1, 2]. The clinical presentation ranges from nonspecific abdominal pain to adrenal insufficiency. Lymphomas are an emerging cause of this complication. Secondary adrenal lymphoma involvement is the most common etiology, followed by primary adrenal lymphoma [3]. This diagnosis should be considered in all patients with adrenal hemorrhage, even in the absence of adenopathy or splenomegaly.
The reference list from the paper itself. Each links out to its DOI / PubMed record.