Haemophilus influenzae Type f Meningitis With an Intraventricular Abscess
Miri Nakashio, Ryoko Nikaido, Junichiro Nishi, Masashi Kasai, Takeshi Morisawa

TL;DR
This paper reports a rare case of Haemophilus influenzae type f meningitis with an intraventricular abscess in a young child and highlights the challenges of treating antibiotic-resistant strains.
Contribution
The paper presents a rare clinical case of Hif meningitis with an intraventricular abscess and β-lactamase-negative ampicillin resistance.
Findings
The patient was successfully treated with a combination of dexamethasone, cefotaxime, and meropenem.
Follow-up imaging showed complete resolution of the abscess with no long-term complications.
The case emphasizes the need for surveillance of Hif serotypes and resistance patterns.
Abstract
Haemophilus influenzae (Hi) is a key pathogen causing bacterial meningitis in children. The introduction of the Haemophilus influenzae type b (Hib) vaccine has significantly reduced the incidence of invasive Haemophilus influenzae disease (IHD). However, cases caused by non-type b strains, such as type f (Haemophilus influenzae type f (Hif)), are gradually increasing, although they remain rare. We report a case of Hif meningitis complicated by an intraventricular abscess in an 11-month-old boy with no significant medical history. He presented with a high fever and lethargy over two days. Cerebrospinal fluid (CSF) analysis revealed pleocytosis and hypoglycorrhachia, while brain magnetic resonance imaging (MRI) identified an intraventricular abscess. Cultures confirmed the presence of Hif with β-lactamase-negative ampicillin resistance (BLNAR). The patient was treated with intravenous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
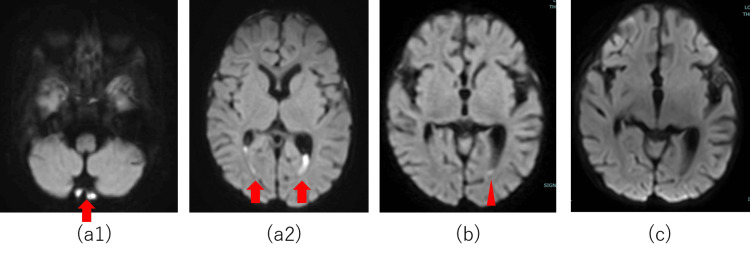 Figure 1
Figure 1| Parameter | Result | Normal range |
| pH | 7.4 | 7.35-7.45 |
| PaCO2 | 34.3 | 35-45 mmHg |
| HCO3⁻ | 21.1 | 22-26 mmol/L |
| Lactate | 2.43 | 0.5-2.2 mmol/L |
| Base excess | -3 | -2 to +2 mmol/L |
| White blood cell count | 10,980/µL | 6,000-17,500/µL |
| Metamyelocytes | 6% | 0% |
| Band neutrophils | 8% | 0%-5% |
| Neutrophils | 48% | 20%-45% |
| Lymphocytes | 35% | 40%-70% |
| Hemoglobin | 10.4 g/dL | 11.0-13.5 g/dL |
| Platelet count | 226,000/µL | 150,000-450,000/µL |
| Sodium | 130 mmol/L | 135-145 mmol/L |
| Potassium | 4.1 mmol/L | 3.5-5.0 mmol/L |
| Glucose | 93 mg/dL | 60-110 mg/dL |
| C-reactive protein | 23.216 mg/dL | <0.5 mg/dL |
| Procalcitonin | 26.13 ng/mL | <0.05 ng/mL |
| C3 | 134 mg/dL | 65-135 mg/dL |
| C4 | 35 mg/dL | 15-40 mg/dL |
| IgG | 403 mg/dL | 300-900 mg/dL |
| IgA | 36 mg/dL | 20-100 mg/dL |
| IgM | 44 mg/dL | 30-120 mg/dL |
| Parameter | Result | Normal range |
| Appearance (color) | Turbid | Clear |
| Cell count | 14,987 cells/µL | 0-10 cells/µL |
| Mononuclear cells | 25% | 100% |
| Polymorphonuclear cells | 75% | 0% |
| Total protein | 312 mg/dL | 14-20 mg/dL |
| Red blood cell count | 40 cells/µL | 0 cells/µL |
| Glucose | 1 mg/dL | 71-90 mg/dL |
| CSF-to-glucose blood ratio | 0.01% | 60%-70% |
| Antimicrobial agent | MIC (µg/mL) | Interpretation |
| Ampicillin | >4 | R |
| Cefaclor | 8 | R |
| Ceftriaxone | 0.5 | S |
| Ampicillin/sulbactam | 1 | R |
| Imipenem | 0.5 | S |
| Meropenem | 0.25 | S |
| Azithromycin | 1 | S |
| Gatifloxacin | ≤0.12 | S |
| Moxifloxacin | ≤0.5 | S |
| ST | ≤10 | S |
| Hospital day | Day 0 | Day 2 | Day 5 | Day 28 | Day 42 | Day 55 |
| Cell count | 14,987 cells/µL | 12,080 cells/µL | 232 cells/µL | 330 cells/µL | 41 cells/µL | 19 cells/µL |
| Total protein | 312 mg/dL | 190 mg/dL | 133 mg/dL | 98 mg/dL | 56 mg/dL | 43 mg/dL |
| Glucose | 1 mg/dL | 54 mg/dL | 36 mg/dL | 34 mg/dL | 34 mg/dL | 40 mg/dL |
| CSF-to-glucose blood ratio | 0.01% | 0.31% | 0.34% | 0.38% | 0.34% | 0.38% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Pneumonia and Respiratory Infections · Tracheal and airway disorders
Introduction
Haemophilus influenzae (Hi) is a common resident of the upper respiratory tract and a major pathogen causing infections such as pneumonia and otitis media. Occasionally, it can lead to invasive diseases, including sepsis and meningitis [1]. This bacterium comprises six serotypes (a-f) and non-typeable strains (non-typeable Haemophilus influenzae (NTHi)) [1]. Encapsulated strains, compared to NTHi, are more resistant to neutrophil phagocytosis and have a greater tendency for hematogenous dissemination, which contributes to their increased pathogenicity [1]. Among these, type b (Haemophilus influenzae type b (Hib)) is the most virulent [1]. Prior to the introduction of the Hib vaccine, Hib was the leading cause of invasive Haemophilus influenzae disease (IHD) [1].
The widespread use of the Hib vaccine has significantly reduced the absolute number of IHD cases [1]. As a result, the predominant causative strains of IHD have shifted from type b to non-type b [1]. Among these non-type b strains, NTHi accounts for the majority of cases [1]. Despite this trend, capsular Haemophilus influenzae-associated IHD remains rare [1].
Here, we report a case of Haemophilus influenzae type f (Hif) meningitis complicated by an intraventricular abscess.
Case presentation
A previously healthy 11-month-old boy presented to our hospital with a two-day history of high fever and subsequent lethargy. His medical history included short bowel syndrome following neonatal bowel resection for jejunoileal atresia. He had received all scheduled vaccinations, including three doses of the Hib vaccine, which were administered at two, three, and four months of age. Additionally, he had been taking cefditoren pivoxil for two days as prescribed by his previous physician for otitis media. Upon arrival (day 0), the patient exhibited impaired consciousness, with a Glasgow Coma Scale score of 4 (E2V1M1), and pallor. His vital signs were as follows: temperature of 40.8℃, blood pressure of 90/47 mmHg, heart rate of 172 beats per minute, respiratory rate of 44 breaths per minute, and oxygen saturation of 98% (room air). Physical examination revealed no bulging anterior fontanelles or nuchal rigidity. Blood tests (Table 1) showed elevated levels of C-reactive protein (23.2 mg/dL), procalcitonin (26.1 ng/mL), and a white blood cell count of 10,980/μL with neutrophil predominance.
Cerebrospinal fluid (CSF) analysis (Table 2) revealed significant pleocytosis (14,987/μL) and hypoglycorrhachia (glucose level: 1 mg/dL). A cerebrospinal fluid smear suggested the presence of Gram-negative bacilli.
Based on these findings, bacterial meningitis was diagnosed. Treatment with intravenous dexamethasone (0.6 mg/kg/day for two days), cefotaxime (300 mg/kg/day), and meropenem (120 mg/kg/day) was initiated promptly.
On day 2, CSF and blood cultures identified β-lactamase-nonproducing ampicillin-resistant (BLNAR) Haemophilus influenzae. Following antimicrobial susceptibility testing (Table 3), therapy was de-escalated to cefotaxime monotherapy.
On day 5, magnetic resonance imaging (MRI) was performed to investigate the persistent fever. Diffusion-weighted imaging of the brain revealed hyperintense areas in the posterior fossa and posterior horns of the bilateral lateral ventricles, suggesting an intracerebral abscess (Figure 1). Given the absence of hydrocephalus and the improvement in blood and CSF test results with antibiotic therapy alone, invasive procedures such as CSF drainage were considered unnecessary. On day 17, a drug rash attributed to cefotaxime necessitated switching to meropenem. A follow-up MRI on day 29 showed complete resolution of the abscess (Figure 1), and by day 55, the CSF cell count decreased (Table 4). The patient completed treatment on day 62 without complications.
DWI findings on brain MRIOn day 5, diffusion-weighted images revealed regions of hyperintensity in the posterior cranial fossa and dorsal horns of the bilateral lateral ventricles (a1 and a2). On day 12, these regions exhibited contractions (b). By day 29, these regions were completely resolved (c).DWI: diffusion-weighted imaging, MRI: magnetic resonance imaging
Blood examinations performed during hospitalization revealed normal immunoglobulin and complement levels, including normal IgG subclasses. The antibody titer against the Hib vaccine was within the normal range. Lymphocyte subset analysis and lymphocyte proliferation test performed on day 23 of life also showed normal results. Additionally, the Bacillus Calmette-Guérin (BCG) vaccine was administered at five months of age, with no issues observed in the subsequent reaction.
Serotyping identified the isolated Haemophilus influenzae as type f, classified as sequence type (ST) 124. PCR analysis confirmed the presence of BLNAR due to mutations in the penicillin-binding protein 3 (PBP3) gene.
Discussion
Based on the present case, we put forth two clinically significant recommendations.
First, the increased virulence of Hif can lead to meningitis. This is partly due to the protein H, found in its capsular membrane and present in most Hib and Hif, which contributes to its strong ability to cause disease [2,3]. Protein H tends to bind with hydronectin, a protein in the blood plasma, which hinders the host's complement system and helps the bacterium adhere to alveolar epithelial cells in the lungs [3]. The binding interaction with hydronectin has been identified in certain surface proteins of NTHi and Hib, suggesting a potential mechanism underlying the high pathogenicity of these bacteria. Additionally, Hif is more genetically stable than other types, and most Hif belongs to a specific genotype called ST124, regardless of regionality [4]. Although several cases of Hif meningitis with intraventricular abscesses have been reported, complete recovery without long-term complications, as observed in this case, is very rare. Sensorineural hearing loss is the most common long-term complication of Haemophilus influenzae meningitis. However, in this case, the patient did not develop any complications, likely due to the prompt initiation of appropriate treatment. Hif infections are diverse and severe, often leading to complications. This makes their diagnosis and treatment particularly challenging [4].
Second, it is crucial to consider drug resistance in Haemophilus influenzae. While β-lactamase-positive ampicillin-resistant (BLPAR) strains are predominant in the USA and European countries, BLNAR rates have risen to 40% in Japan due to drug misuse, which is particularly concerning [5]. Especially in children under the age of three, BLNAR rates are notably high [6]. This could be due to easy spread among nurseries and peers, frequent antibiotic use, and lower antibody levels against Haemophilus influenzae's common P6 antigen [6]. Many Hif strains are susceptible to penicillin; however, BLNAR Hif strains have also been reported in Japan [7-9]. Following the introduction of public funding for the Hib vaccine in 2011, the first case of Hif meningitis was reported in 2013. Since then, all reported cases of invasive Hif infections were identified as BLPAR strains [7]. However, since 2019, sporadic reports of invasive Hif disease caused by BLNAR strains have emerged, highlighting a concerning trend in antimicrobial resistance [8,9]. This case represents another example of this phenomenon, an infrequent instance of meningitis caused by BLNAR Hif.
Therefore, in Japan, cephem antibiotics should be preferred over penicillin when IHD is suspected. If BLNAR is the causative bacteria, de-escalation can be challenging and the selection of antibacterial agents may be restricted in case of side effects, as observed in this case.
Conclusions
In conclusion, we report an extremely rare case of Hif meningitis complicated by an intraventricular abscess, highlighting the strong virulence of this capsulated strain.
While non-Hib capsulated strains of Haemophilus influenzae have been increasing in Western countries where Hib vaccination was introduced earlier, reports of such cases remain rare in Japan. However, their prevalence may rise in the future. Notably, this case also involved a BLNAR strain, reflecting the high proportion of antibiotic-resistant Haemophilus influenzae observed in Japan. This case underscores the necessity of continued monitoring of Haemophilus influenzae serotypes and antimicrobial resistance patterns. Systematic data accumulation and surveillance are crucial for tracking trends and implementing effective preventive and therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Haemophilus influenzae infections in the H. influenzae type b conjugate vaccine era J Clin Microbiol Agrawal A Murphy TF 372837324920112190051510.1128/JCM.05476-11PMC 3209133 · doi ↗ · pubmed ↗
- 2Identification of a Haemophilus influenzae factor H-Binding lipoprotein involved in serum resistance J Immunol Fleury C Su YC Hallström T Sandblad L Zipfel PF Riesbeck K 5913592319220142483539210.4049/jimmunol.1303449 · doi ↗ · pubmed ↗
- 3Haemophilus influenzae type f hijacks vitronectin using protein H to resist host innate immunity and adhere to pulmonary epithelial cells J Immunol Al-Jubair T Mukherjee O Oosterhuis S 5688569519520152653839010.4049/jimmunol.1501197 · doi ↗ · pubmed ↗
- 4Haemophilus influenzae type f in the post-Haemophilus influenzae type b vaccination era: a systematic review J Med Microbiol Reilly AS Mc Elligott M Mac Dermott Casement C Drew RJ 71202210.1099/jmm.0.00160636306238 · doi ↗ · pubmed ↗
- 5Multiclonal expansion and high prevalence of β-lactamase-negative Haemophilus influenzae with high-level ampicillin resistance in Japan and susceptibility to quinolones Antimicrob Agents Chemother Honda H Sato T Shinagawa M 62201810.1128/AAC.00851-18PMC 612550229987153 · doi ↗ · pubmed ↗
- 6Nationwide survey of the development of drug resistance in the pediatric field in 2000-2001, 2004, 2007, 2010, and 2012: evaluation of the changes in drug sensitivity of Haemophilus influenzae and patients' background factors J Infect Chemother Shiro H Sato Y Toyonaga Y Hanaki H Sunakawa K 2472562120152559697710.1016/j.jiac.2014.11.012 · doi ↗ · pubmed ↗
- 7Analysis of Haemophilus influenzae serotype f isolated from three Japanese children with invasive H. influenzae infection J Med Microbiol Hoshino T Hachisu Y Kikuchi T 3553586420152565730110.1099/jmm.0.000031 · doi ↗ · pubmed ↗
- 8β-lactamase nonproducing ampicillin-resistant Haemophilus influenzae type f meningitis in an infant Pediatr Int Okamoto N Nishisho S Fuke N Wakabayashi T Kusaka T 065202310.1111/ped.1545036529651 · doi ↗ · pubmed ↗