The Association Between Anesthetist Leadership Styles and Their Resilience: A Single-Center Study
Laurence Weinberg, Elizabeth P Hu, Mark M Youssef, Benjamin Churilov, Dong-Kyu Lee

TL;DR
This study found that anesthetists with transformational leadership styles have higher resilience and job satisfaction compared to others.
Contribution
The study identifies a link between transformational leadership and resilience in anesthetist leaders.
Findings
71.5% of anesthetists displayed transformational leadership behaviors.
Transformational leaders had significantly higher resilience scores.
Higher resilience was associated with greater job satisfaction and role effectiveness.
Abstract
Purpose: To explore the association between the leadership styles and resilience of anesthetists in leadership roles. Methodology: This prospective study of all anesthetists in leadership roles within a university teaching hospital in Melbourne, Australia, employed three validated, anonymous questionnaires (Multifactor Leadership Questionnaire, Authentic Leadership Questionnaire, and the Resilience Scale). Questionnaire data were summarized using descriptive statistics and presented as counts and proportions. Spearman’s rank correlation was used to evaluate quantitative continuous variables to identify linear relationships. Results: Of the 14 anesthetists in leadership roles, 14 completed all three questionnaires (response rate 100%). Ten participants (71.5%) displayed behaviors consistent with transformational leadership. Three participants (21.4%) displayed behaviors typically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
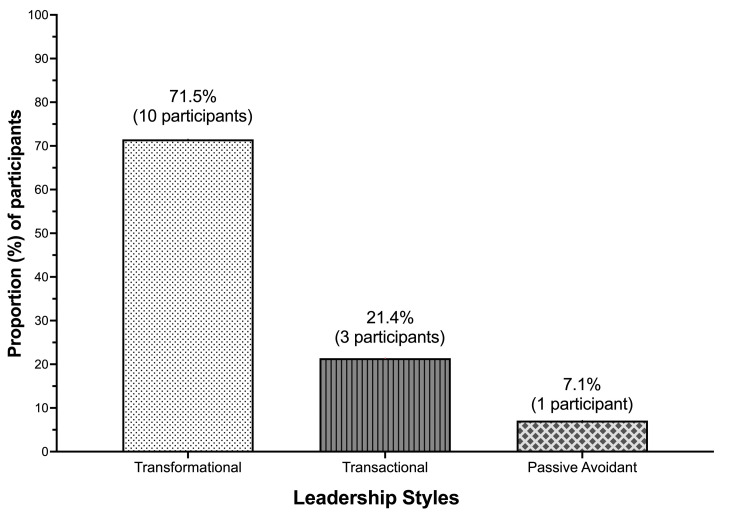 Figure 1
Figure 1 Figure 2
Figure 2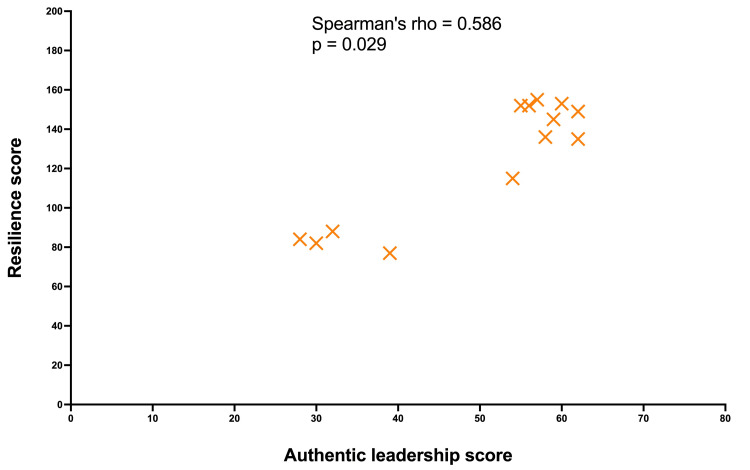 Figure 3
Figure 3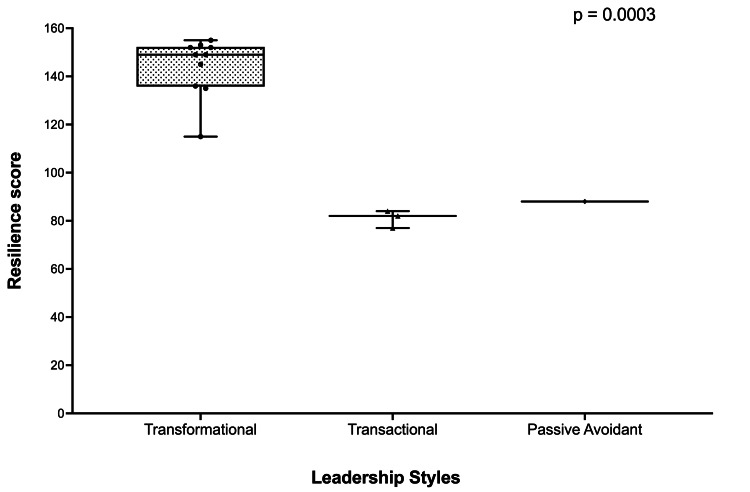 Figure 4
Figure 4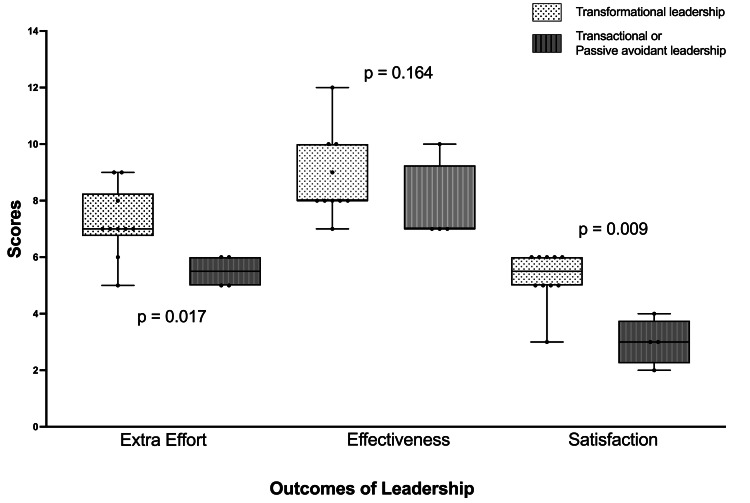 Figure 5
Figure 5| Variable | Number of participants: 14 |
| Age (years) | 44 (40:57) |
| Male gender | 11 (78%) |
| Female gender | 3 (22%) |
| Duration of practice as an anaesthetist (years) | 11 (9:24) |
| Duration in a leadership position (years) | 3.5 (2:5.3) |
| Participants with formal postgraduate leadership qualifications | 3 (21.4%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Innovations in Medical Education
Introduction
The link between leadership styles and resilience is under-researched. Leadership within the medical profession plays a pivotal role in shaping the resilience of physicians who frequently perform their duties under stressful conditions and in demanding environments. Strategies that healthcare leaders could use to cultivate resilience in medical teams have emerged as a topic of growing significance. While leadership and/or resilience have been explored in a variety of healthcare settings [1-3], to date, no research has been undertaken on the association between anesthetists’ leadership styles and their resilience as leaders.
Transformational leadership is currently a topic of significant interest and concern among those seeking to improve the practice of medicine and healthcare in general [4]. Transformational leaders motivate their teams by supporting a shared vision and providing intellectual stimulation, individualized consideration, and inspirational motivation [5]. Within healthcare, transformational leaders create environments that support, value, and encourage excellence among physicians and healthcare teams. The results from several recent studies reveal that healthcare providers supported by transformational leaders frequently exhibit higher levels of resilience [6]. Transformational leaders provide emotional support and foster open communication styles that provide physicians with the capacity to cope with the daily pressures and challenges inherent in their professional work [4].
By contrast, autocratic or transactional leadership focuses on structured rules, clear expectations, hierarchies, and rewards or punishments for performance. While these leadership styles may ensure strict adherence to protocols, they may not promote physician resilience and may contribute to feelings of burnout and decreased job satisfaction [7,8]. Physicians working with autocratic or transactional leaders typically experience reduced autonomy and can find it challenging to adapt to the dynamic and often unpredictable nature of the healthcare environment. Thus, these two leadership styles may be minimally effective at promoting physician resilience. Furthermore, the autocratic or “authoritarian” leadership style leads to burnout and decreased job satisfaction and ultimately undermines the capacity of physicians to recover from adversity [8]. Several scholars have emphasized the importance of collaborative and empowering leadership styles, particularly in academic hospital settings [9]. Leaders who involve physicians in decision-making and provide opportunities for skill development can enhance physician resilience by fostering a sense of autonomy and control [10].
Due to the complex nature of their work, anesthetists in leadership roles face a multitude of stressors, notably the need to integrate academic and administrative responsibilities with ongoing care of high-risk clinical cases. The correlation between different leadership styles and the personal resilience of anesthetists in the context of leadership positions has not been explored previously.
To address this, we performed a prospective study to explore the association between leadership styles and resilience exhibited by anesthetists in leadership roles.
This study focused exclusively on anesthetists in leadership roles to examine the relationship between leadership styles and resilience within a defined group responsible for guiding and managing teams. By targeting anesthetist leaders, we sought to gain insights into how leadership behaviors influence resilience in high-pressure clinical environments, where effective decision-making, team dynamics, and role modeling are essential. Including all anesthetists within the department would introduce variability in leadership experience and responsibilities, potentially diluting the findings and limiting the ability to draw meaningful conclusions about leadership-specific traits and their impact on resilience.
Materials and methods
Setting and design
This study was conducted by Austin Health, a 900-bed university teaching hospital in Melbourne, Australia. The hospital is the only center within Victoria that provides services for acute spinal injuries, liver transplantation, and toxicology. The Department of Anesthesia at Austin Health has 132 consultant anesthetists who perform services for >45,000 elective and emergency procedures across two campuses.
The inclusion criteria were anesthetists within the department of anesthesia who served in leadership roles. These roles included members of the anesthesia executive, the deputy directors, and the anesthesia heads of research, perioperative medicine, cardiac anesthesia, simulation, and pain medicine. The anesthesia executive at Austin Health provides overarching leadership, aligning the department's goals with organizational strategy, ensuring optimal resource allocation, and fostering a culture of excellence. Deputy directors play pivotal roles in managing critical domains, such as staffing, internal operations, and governance, ensuring smooth functioning and equitable support for all team members. Heads of research, perioperative medicine, cardiac anesthesia, simulation, and pain medicine contribute specialized expertise, driving innovation, evidence-based practice, multidisciplinary collaboration, and education while addressing specific patient care and training priorities. Together, they form a cohesive leadership team that ensures comprehensive, forward-thinking decision-making for the department. Exclusion criteria included clinical anesthetists in non-leadership positions, anesthesia nurse unit managers, and non-medical anesthesia business unit managers.
After obtaining approval from the Austin Health Research Ethics Committee (approval number: HREC/110843/Austin-2024), participants were invited by email to participate in the study (see Supplementary File 3, Table 2). Participants were provided with an information form that outlined the purposes of the research (see Supplementary File 3, Table 3). By choosing to complete and submit the survey, participants indicated their voluntary agreement to participate. The information form also stated that, if participants chose to complete the data collection and surveys and submit it for analysis, this would be evidence of their implied consent. The information form provided details about the study's purpose, procedures, potential risks, and benefits, ensuring that participants had sufficient information to make an informed decision. No personal identifiers were collected, and responses were anonymous to maintain confidentiality. Participants were assured that they could withdraw from the survey at any time without penalty, ensuring their autonomy and the voluntary nature of their participation in the study. All participant surveys were completed between 10 September 2024 and 17 September 2024. All surveys were anonymous.
Questionnaire surveys
Three validated questionnaires were used to explore leadership styles and their relationship to the leaders’ resilience. Permission and licensing were obtained to comply with legal requirements and copyright regarding the use of these materials.
The Multifactor Leadership Questionnaire (MLQ)
The MLQ is a psychological assessment tool used to evaluate the entire spectrum of leadership styles [11]. It consists of 36 items focusing on leadership styles and nine items focusing on leadership outcomes (see Supplementary File 3, Table 2). In the questionnaire, five scales assess transformational leadership, two assess transactional leadership, and two assess passive and/or avoidant behavior. The MLQ also assesses effort, efficacy, and contentment or satisfaction as three dimensions of leadership outcomes. It has been validated in multiple cultural contexts and organizational settings. Over the past 25 years, it has served as the primary method for accurately distinguishing between highly effective and ineffective leaders in the military, government, education, manufacturing, technology, religion, hospitals, volunteer organizations, and other settings [9,10,12].
The Authentic Leadership Questionnaire (ALQ)
The ALQ, developed in 2007 (see Supplementary File, Table 3), is a sixteen-item tool used to assess authentic leadership behaviors [13]. This questionnaire is a self-assessment of self-awareness, internalized moral perspectives, balanced processing, and relational transparency, rather than authentic leadership as assessed by those being led. The items are used to generate four ALQ scales as follows: (i) the transparency scale reflects the extent to which a leader demonstrates openness and honesty in their interactions with others; (ii) the ethical/moral scale measures a leader’s moral principles and conduct; (iii) the balanced processing scale evaluates a leader’s ability to engage in fair and objective interpretation and decision-making by considering various perspectives; and (iv) the self-awareness scale measures a leader's capacity to recognize their own abilities, shortcomings, limitations, and how they are perceived by others.
The theoretical foundations of and empirical evidence underlying the concepts of transformational and authentic leadership are closely linked. Authentic leadership has been described as a basic concept that serves as the cornerstone of transformational leadership [14]. While transformational leadership emphasizes the connection of employees' sense of identity and self-worth to the organization, as well as their leadership capabilities, authentic leadership primarily focuses on efforts to nurture followers’ overall sense of self [15]. Moreover, both transformational and authentic leaders prioritize authentic acts and behaviors [16]. Both also highlight the significance of self-awareness, positive role modeling, encouraging follower autonomy, positive interactions between followers and leaders, and the creation of an ethical and supportive organizational environment [9]. These similarities and relationships also provide supplementary leadership frameworks.
For the present study, ALQ scores were calculated for each ALQ scale. The sum of all responses for each scale item was calculated and divided by the total number of scale items. A score of 1-15 signifies weaker authentic leadership, while scores within 16-20 signify stronger authentic leadership. By comparing scores in each of these components, we ascertained the relative strengths and weaknesses of each participant in the research.
The ALQ has been validated by multiple studies performed across a range of cultural and work environments, based on original work reported by Walumbwa et al. [17]. We integrated ALQ responses with the MLQ to evaluate self-awareness, transparency, ethics/morality, and processing abilities exhibited by the study participants and thus measured the complete spectrum of authentic and transformational leadership behaviors.
The Resilience Scale
The resilience scale is a validated 25-item questionnaire that measures resilience in the work environment (see Supplementary File 3, Table 4) [18]. The scale consists of six levels of resilience, with a score of 25-100 signifying very low resilience, 101-115 low resilience, 116-130 moderately low resilience, 131-145 moderate resilience, 146-160 moderately high resilience, and 161-175 high resilience. It identifies five essential characteristics of resilience. First, self-reliance reflects belief in one's own talents and one’s capacity to rely on oneself to recognize personal positive attributes, strengths, and limitations [19,20]. Second, purpose indicates one’s recognition of a meaningful purpose in life and an appreciation of one's own contributions [21]. Third, equity implies that one can maintain a measured and well-balanced view of one's life and experiences and the capacity to regulate strong reactions to adversity [22,23]. Perseverance refers to persistence when confronted with hardship or discouragement. Finally, authenticity is the recognition that one’s journey is distinct and is accompanied by a sense of liberation and perception of one’s own distinctiveness [24].
Statistical analysis
The results of the questionnaires were summarized using descriptive statistics, with data presented as counts and proportions. Non-normal distributions were summarized and presented as medians and interquartile ranges. Because the sample size was small, all data were considered non-normally distributed. Spearman’s rank correlation was computed to assess the relationship between resilience and leadership styles. Spearman’s coefficient (rho) was presented to indicate the strength and direction of the relationship. The p-value and the 95% confidence interval are presented to provide a comprehensive understanding of the relationship between the variables and the precision of the estimate. The coefficient ranges from -1 to +1. A positive value indicates a positive monotonic relationship, while a negative value indicates a negative monotonic relationship. The closer the coefficient is to ±1, the stronger the monotonic relationship. The strength of the relationship was determined as follows: rho = 1: Perfect monotonic relationship; 0.8 ≤ rho < 1: Very strong monotonic relationship; 0.6 ≤ rho < 0.8: Strong monotonic relationship; 0.4 ≤ rho < 0.6: Moderate monotonic relationship; 0.2 ≤ rho < 0.4: Weak monotonic relationship; 0 < rho < 0.2: Very weak monotonic relationship; and rho = 0: No monotonic relationship.
Results
Baseline characteristics
Of the 14 participants in leadership roles who were invited to participate, 14 (100%) completed all three questionnaires. The median age, duration of qualification (years since completion of anesthesia specialty training), formal leadership training or postgraduate qualifications in leadership, and number of years in a leadership position are summarized in Table 1.
Transformational leadership style
In total, 10 participants (71.5%) reported behaviors consistent with transformational leadership (Figure 1). These leaders reported routinely fostering a sense of pride among their affiliated colleagues and acting selflessly on behalf of the department. They asserted that they conducted themselves in a manner intended to cultivate the admiration of others and demonstrated a sense of authority and self-assurance.
Bar graph showing leadership styles among anesthetists in leadership positions
In response to the MLQ, participants with transformational leadership traits reported discussing their paramount values and convictions with others, the significance of maintaining a robust sense of purpose, and the need to foster a shared sense of mission. These leaders reported that they scrutinized their fundamental assumptions for ongoing suitability as leaders and sought diverse viewpoints when resolving issues. They reported frequently soliciting input from other department members, considering the impact of challenges from several perspectives, and proposing novel approaches to complete tasks. These anesthetists reported dedicating significant amounts of time to instruction and mentoring and regarding others as unique individuals rather than as group members. They acknowledged the unique needs, abilities, and goals of each individual, and stated that they were willing to assist others in cultivating their strengths.
Transactional leadership style
Three participants (21.4%) reported behaviors typically associated with transactional leadership (Figure 1). Two distinct transactional styles were apparent.
Anesthetists who followed the first style reported a constructive approach focused on rewarding individuals for their accomplishments. They also reported making their expectations clear, providing recognition when goals were met, establishing clear objectives, encouraging high levels of performance, offering incentives for successful outcomes, and closely monitoring others for any deviations or errors. In contrast to those reporting transformational leadership styles, this group indicated that they offered support to others in return for their efforts, clearly assigned responsibility for attaining performance goals, and provided clarity on rewards available to those who achieved stated objectives. They also reported exhibiting contentment when others fulfilled their expectations.
Anesthetists who followed the second style reported a focus on the continual monitoring of deviations and mistakes. They described having explicit guidelines for adherence and defining what qualifies as inadequate performance. At the same time, they asserted their authority to penalize those who failed to meet these standards. This leadership style involves vigilant oversight of deviations, mistakes, and errors, followed by prompt remedial measures designed to address irregularities, exceptions, and departures from established norms. A review of the MLQ responses revealed that these anesthetists reported focusing exclusively on addressing errors, grievances, and shortcomings, meticulously documenting all mistakes, and prioritizing the resolution of failures to meet established criteria.
Passivity and avoidance leadership style
One anesthetist (7.1%) reported characteristics consistent with “passive-avoidant behavior” (Figure 1). This participant reported a failure to provide systematic and timely responses to circumstances and crises and actively avoided the establishment of clearly defined agreements, expectations, goals, and standards. Because this participant tended to refrain from engaging with others, this leadership style might be more accurately described as “non-leading.” These results suggest that this individual was unwilling to undertake the obligations inherent in their role as an anesthetist; they failed to provide sufficient information to others, neglected to provide feedback, and did not recognize or strive for contentment among their supervisees. Data from the MLQ revealed that this individual typically refrained from engaging in vital matters, was unavailable when needed, evaded decision-making, and procrastinated when asked to respond to pressing inquiries.
Relationship between leadership styles and resilience
As shown in Figure 2, Spearman’s rank correlation analysis revealed a strong positive association between resilience and transformational leadership scores (rho = 0.738; 95% CI: 0.326-0.915; p = 0.004). There was a moderate positive association between resilience and authentic leadership scores (rho = 0.586, 95% CI: 0.068-0.88; p = 0.029) (Figure 3). These statistically significant results indicate a positive relationship between higher levels of resilience and stronger transformational and authentic leadership qualities in our study population.
Spearman’s rank correlation assessing the relationship between resilience scores and transformational leadership scoresThe Spearman’s coefficient (rho) indicates the strength and direction of resilience and transformational leadership scores. Each yellow cross represents a single participant.
Spearman’s rank correlation assessing the relationship between resilience scores and authentic leadership scoresSpearman’s coefficient (rho) indicates the strength and direction of resilience and authentic leadership scores. Each yellow cross represents a single participant.
There was no significant association observed between the number of years that participants were in leadership roles and resilience scores (rho = 0.238, 95% CI: -0.350 to 0.692; p = 0.409). Similarly, there was no significant association observed between age and the following variables: authentic leadership scores (rho = 0.256, 95% CI: -0.334 to 0.701; p = 0.374), transformational leadership scores (rho = 0.222, 95% CI: -0.365 to 0.683; p = 0.441), transactional leadership scores (rho = -0.146, 95% CI: -0.638 to 0.431; p = 0.614), and passive-avoidant leadership scores (rho = -0.064, 95% CI: -0.586 to 0.497; p = 0.828).
As shown in Figure 4, anesthetists with higher authentic leadership scores were more likely to report greater resilience. These findings revealed that these anesthetists as a group were more inclined to foster confidence by transparently disclosing facts and expressing genuine thoughts and emotions. They also reported an inclination to support the importance of individuals, create strong connections, and perceive their authentic selves, encompassing both favorable and unfavorable traits. They also reported a tendency to speak openly about their genuine intentions and desires and to express themselves with the utmost precision.
Box and whisker plots showing resilience scores and leadership stylesData presented as median and 25th and 75th quartiles.
Anesthetists with higher ALQ scores exhibited strong moral viewpoints that provided them with the capacity to internalize and self-manage. In other words, self-regulation was driven by intrinsic moral principles and ideals rather than extrinsic standards, such as those imposed by one's social circle, healthcare institutions, or the prevailing society. Ultimately, these anesthetists reported a greater equilibrium in their abilities to conduct objective analyses of all pertinent information and actively seek perspectives that question their strongly held beliefs.
Leadership effort, effectiveness, and satisfaction
Anesthetists with transformational leadership qualities had significantly higher scores in categories that reflected extra effort exerted and overall role satisfaction (see Figure 5). Specifically, these leaders demonstrated increased levels of motivation, engagement, and initiative among their teams, which translated into consistently higher performance outcomes. The data suggest that transformational leadership traits, such as inspiring and motivating others, fostering an environment of trust, and providing individualized support, were directly associated with enhanced satisfaction. The perception of anesthetists’ effectiveness in their roles did not differ significantly between transformation leaders and transactional or passive/avoidant leaders.
Box and whisker plots showing leadership behavior scores and leadership stylesThe box shows the median and 25th and 75th quartiles. The whiskers represent the minimum and maximum values. Each dot represents a single participant.
Discussion
Key findings
To the best of our knowledge, this is the first study to explore the association between anesthetists’ leadership styles and their resilience. Our results revealed that more than two-thirds of anesthetists in leadership roles reported traits consistent with both transformational and authentic leadership. Furthermore, these findings indicate that transformational and authentic leadership styles correlated significantly with measures of resilience.
These findings also indicate that 20% of the anesthetists in leadership positions reported behaviors more consistent with transactional or passive-avoidant leadership. The results of this study reveal that anesthetists who reported these behaviors also reported significantly lower levels of resilience. As a group, these individuals reported putting less effort into their roles, lower levels of effectiveness, and lower levels of job satisfaction compared to those who scored higher for transformational leadership styles.
These findings align with those reported in previous studies and indicate that leadership actions exhibit a strong correlation with job engagement [25,26] and that resilience is a crucial attribute among those hoping to achieve favorable professional outcomes [27]. These findings emphasize that leaders must develop and safeguard their personal and professional resilience to remain effective in demanding and high-pressure healthcare settings and operate within supportive and nurturing healthcare cultures that promote and value resilience [28].
Factors contributing to leadership styles
Many large university hospitals are traditionally considered to have conservative organizational cultures that value stability, adherence to established procedures, and hierarchical structures, all of which may promote transactional leadership. The practice of academic medicine at large university teaching hospitals also tends to be highly regulated. In such settings, transactional leadership may be encouraged as it ensures compliance with standards and processes [29]. Similarly, because large university hospitals tend to consist of multiple layers of management, transactional leadership may be perceived as more practical for maintaining control and consistency. Hospitals driven by short-term goals and metrics may favor transactional leaders who can provide immediate results rather than transformational leaders with a more long-term vision. Similarly, settings with little to no trust between leaders and employees may foster transactional leadership due to a reliance on explicit rules and rewards for compliance.
In contrast, healthcare systems that foster innovation, empower teams, and inspire a shared vision that transcends standard compliance are more likely to encourage a culture of transformational leadership [30]. By prioritizing long-term impact, research excellence, and patient-centered care, hospitals are more likely to develop leaders who inspire change, drive strategic growth, and cultivate a culture of continuous improvement.
Only three out of 14 (21.4%) anesthetists in leadership positions in our study cohort had formal leadership training qualifications. All three displayed transformational leadership traits. In the absence of an adequate leadership training and development program, physicians may default to a transactional leadership style. Moreover, organizations that resist change may discourage transformational leadership that challenges the status quo of traditional and conservative cultures.
Strengths and limitations
To the best of our knowledge, this is the first study to explore the association between anesthetists’ leadership styles and their resilience. The use of validated standardized questionnaires ensured consistent data collection and analysis, facilitating comparison and generalization. Despite the relatively small leadership group, responses were anonymous, which facilitated more candid and honest responses to sensitive questions. By systematically analyzing the behaviors and resilience strategies of clinical leaders, our findings underscore the importance of fostering resilience as a core component of leadership training, enabling hospitals to cultivate leaders who can navigate the complex, high-stakes environments inherent in healthcare. Finally, our findings can inform the design of leadership programs by emphasizing resilience-building techniques, such as stress management, reflective practice, and team dynamics, ensuring that clinicians in leadership positions are equipped with the skills to lead effectively and sustain high performance. Integrating these insights into leadership development can enhance organizational culture, improve patient care outcomes, and build a more resilient healthcare workforce.
However, the study has several limitations. The present study did not explicitly evaluate the impact of personal qualities, such as self-efficacy, self-awareness, emotional regulation, and drive for improvement. While we acknowledge that these intrinsic characteristics contribute to the cultivation of essential leadership attributes (including effective communication, clinical competence, interpersonal accessibility, and the capacity to serve as an exemplar), it is important to note that our research methodology indirectly addressed these factors. The three validated instruments employed in our study - the Resilience Scale, the Multifactor Leadership Questionnaire, and the Authentic Leadership Questionnaire - contain specific items that assess various dimensions of these personal qualities. Consequently, we posit that many of these individual attributes were inherently captured within the comprehensive framework of our assessment tools, providing an indirect measure of their influence on clinical leadership effectiveness.
We only surveyed anesthetists in leadership roles, and the data may not be generalizable to clinicians in leadership roles, or indeed other anesthetists, in other departments or institutions. Only anesthetist leaders were included in this survey, not the members of staff they lead, who might have very different perspectives on their leadership styles. There could well be a disjuncture between how leaders perceive their leadership and how those being led perceive that leadership. This single-center study, conducted at a university teaching hospital in Australia, may not be generalizable to healthcare settings in other hospitals or countries. Furthermore, the results cannot exclude response bias, i.e., respondents providing inaccurate or socially desirable responses because of perceived hospital expectations.
The study may have been affected by inherent limitations in the questionnaires, such as the absence of strict cutoff scores and/or studied methods to categorize individuals’ favored leadership styles. Instead, these tools reflect a range of behaviors that must be interpreted within their specific and unique contexts. Finally, and most importantly, these questionnaires provide only an initial understanding of the complex issues that contribute to leadership and resilience and may not capture what might be achieved using qualitative research methods. For example, in-depth interviews or focus group research may have provided us with greater insight into other factors contributing to both resilience and leadership styles, such as emotional intelligence, capacity for conflict resolution, and staff burnout.
Conclusions
In summary, the findings of this study reveal that anesthetists who exhibit transformational and authentic leadership characteristics are likely to be more resilient than those with transactional or passive-avoidant leadership styles. Higher levels of resilience are associated with greater role effectiveness and higher levels of job satisfaction. Future hospital leadership development programs should focus on cultivating transformative leadership abilities through training, workshops, and mentoring programs designed to enhance understanding and the application of transformational leadership practices.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: a systematic review of quantitative studies J Nurs Manag Labrague LJ 189319052920213384308710.1111/jonm.13336 PMC 8250179 · doi ↗ · pubmed ↗
- 2Resilience in medical doctors: a systematic review Postgrad Med J Mc Kinley N Karayiannis PN Convie L Clarke M Kirk SJ Campbell WJ 1401479520193092671610.1136/postgradmedj-2018-136135 · doi ↗ · pubmed ↗
- 3Medical leadership, a systematic narrative review: do hospitals and healthcare organisations perform better when led by doctors?BMJ Open Clay-Williams R Ludlow K Testa L Li Z Braithwaite J 07201710.1136/bmjopen-2016-014474 PMC 562345528947438 · doi ↗ · pubmed ↗
- 4Transformational leadership and psychological well-being of service-oriented staff: hybrid data synthesis technique Int J Environ Res Public Health Kim HD Cruz AB 81891920223580584610.3390/ijerph 19138189 PMC 9266046 · doi ↗ · pubmed ↗
- 5Transformational Leadership, 2nd Edition Bass BM Riggio RE Oxfordshire, UK Taylor and Francis 2006 http://www.perlego.com/book/1546534/transformational-leadership-pdf
- 6The effect of transformational and transactional leadership styles on organizational readiness for change among health professionals SAGE Open Nurs Mekonnen M Bayissa Z 23779608231185923920233744897310.1177/23779608231185923 PMC 10336755 · doi ↗ · pubmed ↗
- 7Physician burnout—evidence that leadership behaviors make a difference: a cross-sectional survey of an academic medical center Mil Med Hu JS Phillips J Wee CP Pangaro LN 07188202310.1093/milmed/usac 31236260483 · doi ↗ · pubmed ↗
- 8Association of burnout, professional fulfillment, and self-care practices of physician leaders with their independently rated leadership effectiveness JAMA Netw Open Shanafelt TD Makowski MS Wang H 03202010.1001/jamanetworkopen.2020.7961 PMC 729861232543700 · doi ↗ · pubmed ↗