Frailty Assessment to Improve Risk Stratification in Elderly Patients Undergoing Elective Cardiac Surgery
Kamile Ozeren, Ahmet Can Topcu, Ilyas Kayacioglu

TL;DR
This study explores how adding a frailty marker improves risk prediction for elderly patients undergoing heart surgery.
Contribution
The study identifies serum albumin as a potential frailty marker to enhance existing cardiac surgery risk models.
Findings
EuroSCORE II and serum albumin were significantly associated with postoperative adverse outcomes.
Adding albumin to EuroSCORE II increased its predictive power for early postoperative mortality/morbidity.
Abstract
Frailty is a biological syndrome of the elderly characterized by decreased physiological reserve and weakened response to stressors. Most cardiac surgical risk models incorporate chronologic age as a risk parameter, but not frailty. We aimed to identify the frailty assessment tool with the highest prognostic value to predict postoperative adverse outcomes in elderly patients undergoing cardiac surgery and to investigate whether addition of a frailty parameter to cardiac surgical risk models would increase predictive power. This is a single-center, prospective, observational study. Consecutive adults, undergoing elective cardiac surgery between January and May 2020, were included. The European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) and Society of Thoracic Surgeons risk scores were calculated. Fried Scale, Short Physical Performance Battery, Clinical Frailty…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
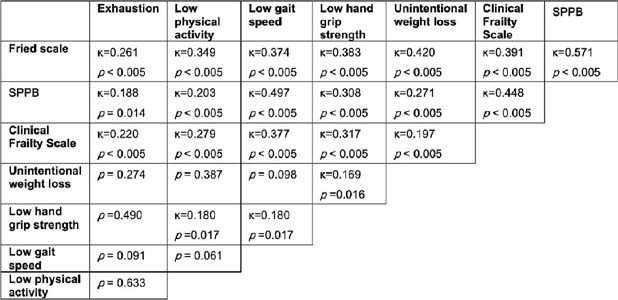 Figure 1
Figure 1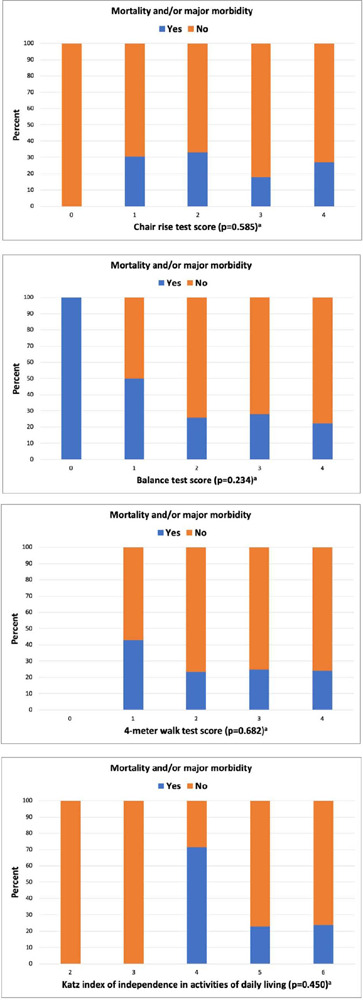 Figure 2
Figure 2| Phenotypic criteria | Measurement | Point |
|---|---|---|
| 1. Shrinking | Unintentional weight loss ≥ 4.5 kg or ≥ 5% of body weight in the past 12 months | 1 point |
| 2. Weakness | Average of hand grip strength measured 3 times using a digital hand dynamometer: | 1 point |
| Men | ||
| BMI ≤ 24 and hand grip strength ≤ 29 kg | ||
| BMI = 24.1-26 and hand grip strength ≤ 30 kg | ||
| BMI = 26.1-28 and hand grip strength ≤ 30 kg | ||
| BMI > 28 and hand grip strength ≤ 32 kg | ||
| Women | ||
| BMI ≤ 23 and hand grip strength ≤ 17 kg | ||
| BMI = 23.1-26 and hand grip strength ≤ 17.3 kg | ||
| BMI = 26.1-29 and hand grip strength ≤ 18 kg | ||
| BMI > 29 and hand grip strength ≤ 21 kg | ||
| 3. Slowness | 5-meter gait speed measured at a regular pace: | 1 point |
| Men | ||
| Height ≤ 173 cm and gait speed ≤ 0.65 m/sec | ||
| Height > 173 cm and gait speed ≤ 0.76 m/sec | ||
| Women | ||
| Height ≤ 159 cm and gait speed ≤ 0.65 m/sn | ||
| Height > 159 cm and gait speed ≤ 0.76 m/sn | ||
| 4. Low physical activity | Questioning of weekly energy expenditure using a short version of Minnesota Leisure Time Activity | 1 point |
| Questionnaire: | ||
| Men < 383 kcal/week | ||
| Women < 270 kcal/week | ||
| 5. Exhaustion | An answer of “often (≥ 3 days)” to any of the following questions: | 1 point |
| “In the last week, how often did you feel that everything you did was an effort?” | ||
| “In the last week, how often did you feel that you could not get going?” |
|
| |||
|
|
|
| |
| < 10 sec. | - | - | 0 points |
| 10 sec. | < 10 sec. | - | 1 point |
| 10 sec. | 10 sec. | < 3 sec. | 2 points |
| 10 sec. | 10 sec. | 3 to 9.99 sec. | 3 points |
| 10 sec. | 10 sec. | 10 sec. | 4 points |
|
| |||
| Unable to perform | 0 points | ||
| > 8.7 sec. | 1 point | ||
| 6.21 to 8.7 sec. | 2 points | ||
| 4.82 to 6.2 sec. | 3 points | ||
| < 4.82 sec. | 4 points | ||
|
| |||
| Unable to perform | 0 points | ||
| ≥ 16.7 sec. | 1 point | ||
| 13.7 to 16.6 sec. | 2 points | ||
| 11.2 to 13.6 sec. | 3 points | ||
| ≤ 11.1 sec. | 4 points | ||
| Age (years), median (IQR) | 70 (67; 74) |
| Female sex, n (%) | 57 (34.76) |
| Body mass index (kg/m2), median (IQR) | 28.4 (25.7; 32.5) |
| Left ventricular ejection fraction (%), median (IQR) | 55 (45; 60) |
| Glomerular filtration rate (ml/dk/1,73 m2), median (IQR) | 71.7 (58.1; 86) |
| Creatinine (mg/dl), median (IQR) | 0.995 (0.83; 1.17) |
| NYHA class, n (%) | |
| II | 109 (66.46) |
| III | 55 (33.54) |
| Current smoker, n (%) | 21 (12.8) |
| Hypertension, n (%) | 89 (54.27) |
| Diabetes, n (%) | 65 (39.63) |
| Chronic renal disease, n (%) | 47 (28.66) |
| Chronic obstructive pulmonary disease, n (%) | 73 (44.51) |
| Arrhythmia, n (%) | 22 (13.41) |
| Carotid artery disease, n (%) | 25 (15.34) |
| Peripheral artery disease, n (%) | 6 (3.66) |
| History of stroke, n (%) | 18 (10.98) |
| Previous myocardial infarction, n (%) | 56 (34.15) |
| Previous cardiac surgery, n (%) | 8 (4.88) |
| EuroSCORE II (%), median (IQR) | 2.27 (1.47; 3.98) |
| STS-PROM (%), median (IQR) | 1.4 (0.92; 2.41) |
| STS-PROMM (%), median (IQR) | 10.28 (7.76; 15.04) |
| Operation, n (%) | |
| CABG | 106 (64.63) |
| Valve surgery | 38 (23.17) |
| Combined procedure | 20 (12.2) |
| Primary composite endpoint, n (%) | 41 (25) |
| Mortality, n (%) | 15 (9.1) |
| Stroke, n (%) | 6 (3.7) |
| Acute renal failure, n (%) | 9 (5.5) |
| Prolonged mechanical ventilation, n (%) | 18 (11) |
| Deep sternal wound infection, n (%) | 11 (6.7) |
| Reoperation, n (%) | 18 (11) |
| Prolonged hospital stay, n (%) | 26 (15.9) |
| Prolonged intensive care unit stay, n (%) | 35 (21.3) |
| Hospital readmission for any reason, n (%) | 18 (11) |
| n (%) | Age (years), median (IQR) | BMI (kg/m2), median (IQR) | Sex | ||
|---|---|---|---|---|---|
| Female, n (%) | Male, n (%) | ||||
|
| |||||
| No | 123 (75) | 69 (67; 73) | 28.71 (25.97; 32.76) | 40 (70.2) | 83 (77.6) |
| Yes | 41 (25) | 71 (69; 75) | 27.55 (25.06; 30.86) | 17 (29.8) | 24 (22.4) |
|
| |||||
| No | 138 (84) | 69 (67; 74) | 28.37 (25.4; 32.45) | 46 (80.7) | 92 (86) |
| Yes | 26 (16) | 71.5 (68; 74) | 29 (26.12; 32.85) | 11 (19.3) | 15 (14) |
|
| |||||
| No | 129 (79) | 69 (67; 73) | 28.64 (25.59; 32.88) | 46 (80.7) | 83 (77.6) |
| Yes | 35 (21) | 71 (68.5; 75) | 27.78 (25.99; 31.44) | 11 (19.3) | 24 (22.4) |
| P-value | |||||
|
| |||||
| No | 146 (89) | 70 (67; 74) | 28.37 (25.88; 32.02) | 53 (93) | 93 (86.9) |
| Yes | 18 (11) | 69 (66; 73) | 29.38 (24; 34.63) | 4 (7) | 14 (13.1) |
| Fried scale, n (%) | |
| Non-frail | 126 (76.8) |
| Frail | 38 (23.2) |
| Short Physical Performance Battery, n (%) | |
| Not frail | 122 (74.4) |
| Frail | 42 (25.6) |
| Clinical Frailty Scale, n (%) | |
| Not frail | 94 (57.3) |
| Frail | 70 (42.7) |
| Unintentional weight loss, n (%) | |
| Not frail | 132 (80.5) |
| Frail | 32 (19.5) |
| Low hand grip strength, n (%) | |
| Not frail | 102 (62.2) |
| Frail | 62 (37.8) |
| Low gait speed, n (%) | |
| Not frail | 83 (50.6) |
| Frail | 81 (49.4) |
| Low physical activity, n (%) | |
| Not frail | 83 (50.6) |
| Frail | 81 (49.4) |
| Exhaustion, n (%) | |
| Not frail | 134 (81.7) |
| Frail | 30 (18.3) |
| Balance test, median (IQR) | 4 (3 to 4) |
| 4-meter walk test, median (IQR) | 3 (3 to 4) |
| Chair rise test, median (IQR) | 4 (3 to 4) |
| Katz index, median (IQR) | 6 (5 to 6) |
| Albumin (g/dl), median (IQR) | 4.04 (3.68 to 4.36) |
| Primary endpoint | Risk ratio | 95% CI | |||
|---|---|---|---|---|---|
| No | Yes | ||||
| EuroSCORE II, median (IQR) | 2.09 (1.42; 3.77) | 3.33 (1.89; 4.31) | 0.045a | ||
| STS-PROM, median (IQR) | 1.35 (0.92; 2.30) | 1.60 (0.94; 2.42) | 0.150a | ||
| STS-PROMM, median (IQR) | 10.18 (7.52; 14.05) | 11.15 (8.31; 18.99) | 0.109a | ||
| Fried scale, n (%) | 0.831b | 1.070 | 0.579-1.976 | ||
| Non-frail (0 to 2) | 95 (75.4) | 31 (24.6) | |||
| Frail (3 to 5) | 28 (73.7) | 10 (26.3) | |||
| SPPB, n (%) | 0.836b | 1.065 | 0.587-1.932 | ||
| Not frail (9 to 12) | 92 (75.4) | 30 (24.6) | |||
| Frail (0 to 8) | 31 (73.8) | 11 (26.2) | |||
| Clinical Frailty Scale, n (%) | 0.101b | 1.555 | 0.915-2.642 | ||
| Not frail (0 to 4) | 75 (79.8) | 19 (20.2) | |||
| Frail (5 to 9) | 48 (68.6) | 22 (31.4) | |||
| Unintentional weight loss, n (%) | 0.999b | 1 | 0.512-1.952 | ||
| Not frail | 99 (75) | 33 (25) | |||
| Frail | 24 (75) | 8 (25) | |||
| Hand grip strength, n (%) | 0.577b | 1.165 | 0.682-1.990 | ||
| Not frail | 78 (76.5) | 24 (23.5) | |||
| Frail | 45 (72.6) | 17 (27.4) | |||
| Gait speed, n (%) | 0.787b | 1.076 | 0.633-1.829 | ||
| Not frail | 63 (75.9) | 20 (24.1) | |||
| Frail | 60 (74.1) | 21 (25.9) | |||
| Low physical activity, n (%) | 0.928b | 0.976 | 0.574-1.659 | ||
| Not frail | 62 (74.7) | 21 (25.3) | |||
| Frail | 61 (75.3) | 20 (24.7) | |||
| Exhaustion, n (%) | 0.816b | 1.083 | 0.558-2.102 | ||
| Not frail | 101(75.4) | 33 (24.6) | |||
| Frail | 22 (73.3) | 8 (26.7) | |||
| Albumin, n (%) | 0.003b | 2.398 | 1.327-4.336 | ||
| Not frail | 76 (83.5) | 15 (16.5) | |||
| Frail | 26 (60.5) | 17 (39.5) | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Frailty in Older Adults · Hip and Femur Fractures
INTRODUCTION
World population is aging, and so is the cardiac surgery population. Patients ≥ 65 years of age make up more than half of the adult cardiac surgery population^[1]^. Advanced age is a significant risk factor for postoperative adverse outcomes, however, chronological age does not always reflect biological age^[2]^. The most common cardiac surgical risk models incorporate chronologic age as a risk parameter, but not patients’ frailty status or biological age^[3,4]^. Frailty is a biological syndrome characterized by decreased physiological reserve and weakened response to stressors, associated with advanced age^[5,6]^. There is no gold standard definition of frailty, and its prevalence varies considerably depending on which assessment tool is used^[6,7]^. The phenomenon of frailty is widely studied in patients over the age of 65 and should be included in the risk assessment process of surgical candidates of this age group^[6,7]^.
We aimed to identify the frailty assessment tool with the highest prognostic value to predict postoperative adverse outcomes in elderly patients undergoing cardiac surgery and to investigate whether addition of a frailty parameter to cardiac surgical risk models would increase the predictive power of these models.
METHODS
Study Design and Participants
This is a single-center, prospective, observational study. The study protocol was approved by Haydarpasa Numune Education and Research Hospital Clinical Research Ethics Committee on July 22, 2019 (ID: HNEAH-KAEK 2019/KK/76). A written informed consent was obtained from each participant. All procedures related to the study were in accordance with the ethical standards of the 1964 Helsinki Declaration. The study protocol was registered on ClinicalTrials.gov on December 10, 2019 (NCT04191915). Consecutive adult patients, scheduled to undergo elective cardiac surgery between January 15 and May 15, 2020, at Dr. Siyami Ersek Thoracic and Cardiovascular Surgery Education and Research Hospital, were assessed for enrollment. Inclusion criteria were (1) patient’s age ≥ 65 years and (2) patient undergoing coronary artery bypass grafting (CABG), heart valve surgery, or combined CABG and valve surgery. Patients were excluded if they (1) were undergoing emergency surgery; (2) refused to participate; (3) had hemodynamic instability; or (4) had neuropsychiatric disorders.
Cardiac Surgical Risk Assessment
The European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) and the Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Risk Model were used to assess operative risk^[3,4]^. STS scores were calculated to estimate both predicted risk of mortality (STS-PROM) and predicted risk of mortality and major morbidity (STS-PROMM)^[4]^.
Frailty Assessment
Frailty tests were performed by a single operator (K.O.) one day prior to surgery. Several widely accepted and commonly used tests, Fried scale, Short Physical Performance Battery (SPPB), Clinical Frailty Scale (CFS), serum albumin, and Katz index were utilized for frailty assessment. Fried scale’s and SPPB’s components were also individually tested for their ability to predict outcome. Five components of Fried’s frailty phenotype were examined as described by Fried et al.:^[5]^ shrinking (unintentional weight loss), weakness (low hand grip strength), self-reported exhaustion, slowness (low gait speed), and low physical activity (Supplementary Table 1). Patients were diagnosed as frail if they met ≥ 3 criteria. The SPPB, another frailty assessment tool based on phenotypic approach, is comprised of three components: slowness, weakness, and balance^[8]^. Standing balance, four-meter walk, and chair rise tests were used to measure balance, gait speed, and weakness, respectively, as described by Guralnik et al.^[8]^ (Supplementary Table 2). Each component was scored 0 to 4, and patients received a total score of 0 to 12. An SPPB score of 0 to 8 classified patients as frail^[9]^. Current version of the CFS^[10]^, which was originally designed by Rockwood et al. to represent and correlate with a frailty index, was administered to score patients’ frailty degree on a scale of 1 (very fit) to 9 (terminally ill) based on their functional status. The most common cutoff value of ≥ 5 was used to classify patients as frail^[11]^. Serum albumin was recorded as a biomarker of frailty^[12,13]^.
**Supplementary
**Supplementary
Katz Index of Independence in Activities of Daily Living was applied to participants. One point was given for self-reported performance of each of the following activities without supervision, direction, or personal assistance: bathing, dressing, toileting, transferring, continence, feeding. Each participant obtained a score of 0 (very dependent) to 6 (independent).
Follow-up and Study Endpoints
Patients were followed-up for 30 days after surgery or during index hospitalization (whichever is longer).
The primary endpoint was a composite of operative mortality and/or any major morbidity including stroke, acute renal failure, prolonged ventilation, deep sternal wound infection, and re-operation, as described by the STS^[4]^. Participants who experienced any of the abovementioned adverse outcomes were considered to have reached the primary endpoint. Operative mortality included all deaths, regardless of cause. Stroke was defined as global or focal neurological dysfunction caused acutely by ischemia or hemorrhage and lasting for at least 24 hours. Acute renal failure was defined as occurrence of any of the following: new-onset need for renal replacement therapy, a serum creatinine level of ≥ 4 mg/dl with an increase of ≥ 0.5 mg/dl from baseline, a ≥ 3-fold increase in creatinine from baseline, a urine output of ≤ 0.3 ml/kg/hour for ≥ 24 hours, or anuria for ≥ 12 hours. Prolonged ventilation was defined as reintubation or mechanical ventilation ≥ 24 hours.
Secondary endpoints were prolonged hospital stay (> 14 days), prolonged intensive care unit stay (> 48 hours), and hospital readmission for any reason.
Statistical Analysis
Power analysis was performed to estimate sample size using G*Power software v3.1.7. The primary endpoint of composite mortality and/or major morbidity was tested with a predicted incidence of 19.3% as previously reported by Afilalo et al.^[2]^ in a similar patient population. At least 150 participants were needed to achieve an 80% (Beta=0.2) power at the 5% (Alpha=0.05) level of significance according to Cohen’s kappa coefficient.
IBM SPSS Statistics for Windows (version 28.0, Armonk, NY: IBM Corp.) was used for statistical analyses. Categorical variables were presented as numbers (n) and proportions (%). Continuous variables were presented as median (interquartile range [IQR]). Normality of quantitative data was assessed with Shapiro-Wilk test, Q-Q plots, and histograms. Independent samples t-test was used to compare normally distributed variables. Mann-Whitney U test was used to compare non-normally distributed variables. Qualitative data were analyzed with Pearson’s chi-squared test. Fleiss’ kappa and Cohen’s kappa were used to assess agreement of frailty tests on identifying patients as frail. Missing data was handled using pairwise deletion. Frailty assessment results were analyzed as categorical variables except for albumin. Albumin measurement was treated as a continuous variable, and the optimal cutoff with the highest sensitivity and specificity for the primary endpoint was identified using univariate logistic regression analysis. Multinominal logistic regression analysis was performed to create predictive models. Receiver operating characteristic curves were plotted from logistic regression models, and areas under curves were compared using DeLong’s method. Risk ratio with 95% confidence interval was calculated to assess relative risk of being frail to experience the primary outcome. A two-sided P-value of < 0.05 was considered statistically significant.
RESULTS
A total of 164 patients were included (57 women, 34.76%). Median patient age was 70 years (range, 65-85; IQR, 67-74). One hundred six (64.63%) patients underwent isolated CABG, 38 (23.17%) underwent isolated valve surgery, and 20 (12.2%) underwent combined CABG and valve surgery. The study population had a median EuroSCORE II of 2.27% (IQR, 1.47-3.98), STS-PROM of 1.4% (IQR, 0.92-2.41), and STS-PROMM of 10.28% (IQR, 7.76-15.04) (Table 1).
All participants completed follow-up (100%). Primary endpoint, the composite of postoperative mortality and/or any major morbidity, was observed in 41 (25%) patients. Operative mortality rate was 9.1% with 15 deaths. Prolonged hospital and intensive care unit stay occurred in 26 (15.9%) and 35 (25.3%) patients, respectively. Eighteen (11%) hospital survivors were rehospitalized within the follow-up period (Table 2).
Demographics were not significantly associated with postoperative adverse outcomes (Table 3). Patients who experienced mortality and/or major morbidity were slightly older than those who did not; median age 71 (IQR, 69-75) vs. 69 (IQR, 67-73) years (P=0.048), respectively (Table 3). However, a point-biserial analysis did not demonstrate a significant correlation between age and primary outcome (r=0.151, P=0.053).
There was variability between frailty tools regarding frailty prevalence. Thirty-eight (23.2%) patients were categorized as frail by Fried’s scale, 42 (25.6%) by SPPB, and 70 (42.7%) by CFS (Table 4). Moreover, the agreement between Fried’s scale, SPPB, and CFS regarding frailty diagnosis was less than good (P<0.005) (Figure 1). Study population was relatively independent in daily living activities with a median Katz index of 6 (IQR, 5 to 6). Albumin data was missing for 30 participants. Remaining 134 patients had a median albumin level of 4.04 g/dl (IQR, 3.68 to 4.36) (Table 4). Among cardiac surgery risk scores and frailty assessment tools, only EuroSCORE II and albumin were significantly associated with the primary endpoint (P=0.045 and P=0.031, respectively) (Table 5, Figure 2). An albumin level of 3.84 g/dl had the highest sensitivity and specificity to predict a composite of mortality and/or major morbidity (area under curve = 0.637). Using the cutoff of albumin < 3.84 g/dl, we identified 43 (26.2%) patients as frail. Patients in the lower albumin group had a significantly increased relative risk of experiencing the primary endpoint with a risk ratio of 2.398 (95% confidence interval, 1.327-4.336) (Table 5). Surgical risk scores and frailty tests were not associated with any of the secondary endpoints (P>0.05).
Fig. 1. Fleiss’ kappa test results demonstrating lack of agreement between frailty assessment tools on identifying patients as frail. SPPB=Short Physical Performance Battery.
Table 5: Relationship of cardiac surgical risk models and frailty assessment tools with the primary endpoint.
Fig. 2. Association of (A) chair rise test, (8) balance test, (C)4-meter walk test, (0)Katz index with postoperative mortality and/or major morbidity a Mann-Whitney U test.
In order to investigate whether addition of a frailty parameter to cardiac surgical risk scoring systems would increase prognostic power, a diagnostic model was created by combination of EuroSCORE II and serum albumin, and the new model’s ability to predict the primary endpoint was assessed. Whereas EuroSCORE II’s R-squared value increased from 0.07 to 0.144 after addition of albumin, the new model was not associated with the primary outcome (P=0.571).
DISCUSSION
The results of the present study indicate that assessment of frailty beforecardiacsurgeryinelderlypatientshasthepotentialtoimprove efficiency of risk prediction and decision-making processes in this delicate patient population. This is in concordance with previous research demonstrating that frailty assessment has incremental predictive value over widely utilized risk scoring systems including the STS and EuroSCORE^[14,15,16,17,18,19]^. In the FRAILTY-AVR study, which included 1020 patients across 14 centers and three countries, Afilalo et al.^[14]^ investigated the value of frailty to predict all-cause mortality and disability one year after surgical and transcatheter aortic valve replacement (TAVR). The authors concluded that frailty, measured by the Essential Frailty Toolset, was a strong predictor of mortality and disability^[14]^. Similarly, in a study of 400 adults aged ≥ 74 years, Sündermann et al.^[16]^ observed that Comprehensive Assessment of Frailty (CAF) toolset accurately identified patients at risk of 30-day mortality following cardiac surgical procedures. In the one-year follow-up of the same cohort, a simplified version of the CAF toolset also predicted adverse events at mid-term^[17]^.
Albumin was the only frailty tool that predicted early postoperative mortality and morbidity in elective cardiac surgery patients ≥ 65 years of age. This correlates with recent evidence reporting that lower preoperative albumin is associated with increased risk of adverse outcomes in adults undergoing cardiac procedures^[12,13,14]^. In a retrospective analysis of 470 patients, Hebeler et al.^[12]^ revealed that among a set of frailty assessment tools, albumin was the only frailty marker associated with one-year mortality in patients undergoing TAVR. Similarly, in a retrospective study by Forcillo et al.^[13]^ including 361 high- and extreme-risk TAVR patients, albumin was the only frailty test that was predictive of 30-day all-cause mortality.
We also demonstrated that addition of albumin as a frailty marker to EuroSCORE II risk model did not increase the model’s ability to predict early postoperative mortality and morbidity, however has the potential to do so; a finding that supports previous research reporting improved prognostic power after inclusion of a frailty parameter to traditional risk scores^[1,15,16]^. This finding is especially important since EuroSCORE II includes poor mobility as a risk variable, but not as a measure of frailty, rather as a measure of disability secondary to musculoskeletal or neurological dysfunction^[3]^. Whereas there is evidence that poor mobility has superior predictive value for adverse outcomes after TAVR compared to several frailty indices, it should be noted that poor mobility as defined by EuroSCORE II is not a frailty measure^[3,20]^. The STS has been collecting five-meter gait speed data as a potential frailty marker for over a decade, however, gait speed variable has not been included in the current version of the STS risk model due to missing data in 95% of patients^[1]^. Performance-based tests such as gait speed and hand grip strength are time-consuming, often require specialized environment and equipment, and may not always be suitable for the practicing clinician to perform^[21,22,23]^. Albumin, a cheap, quick, easy-to-perform biomarker of frailty, may be considered as an adjunct or alternative to poor mobility and five-meter gait speed test for inclusion in the EuroSCORE II and STS adult cardiac surgery risk models. Albumin may also be useful in the follow-up of prehabilitation of frail adults before cardiac surgery^[24]^. By all means, inclusion of a convenient frailty marker to current cardiac surgical risk scoring systems would be significantly beneficial for the elderly patients, especially those with severe aortic stenosis who need a decision between surgery and TAVR^[14]^. Even though frailty, disability, and comorbidity are distinct entities, they cannot be entirely separated from each other. Frailty is primarily a concern of older age, and disabilities and comorbidities increase in incidence with older age. A frail person is more prone to become disabled or comorbid, and vice versa. Therefore, it is reasonable to assume that frailty tools, which stem from a frailty phenotype and assess frailty as a distinct entity, are more useful in community-based research rather than clinical research^[22,25,26,27]^. This might be the explanation why phenotypic approaches such as Fried’s scale and SPPB failed to predict postoperative adverse outcomes in our population of patients with cardiac disease. In addition, frailty tests that measure performance are susceptible to patient manipulation. It was the authors’ observation that some patients tried to reflect themself better or worse than they actually are. Albumin is more resistant to such manipulation. With this regard, it should be noted that there are several tools to assess frailty based on various approaches. The most appropriate tool for a given setting and patient population should be utilized and included in the surgical evaluation process as an indicator to decide whether a patient is a suitable candidate for surgery or not.
A lack of significant association or correlation between demographics and the primary endpoint indicates that frailty was an age- and sex-independent predictor of adverse outcomes in our cohort. Besides, EuroSCORE II and STS-PROM underestimated mortality, and STS-PROMM underestimated composite of mortality and morbidity. This correlates with a recent study by Taleb-Bendiab et al.^[28]^, which reported that both EuroSCORE II and STS score significantly underestimated postoperative risk in 1229 elderly patients undergoing cardiac surgery. These findings, along with other reports, suggest that cardiac surgical risk stratification of elderly patients should include a measure of frailty, independently of chronological age^[1,29,30]^. This also explains why we observed higher-than-expected mortality and morbidity rates in our study population.
Body mass index was not associated with postoperative outcomes. This is in accordance with research reporting that frailty is not synonymous with low body weight^[6,27]^. An obese patient may be sarcopenic with reduced muscle mass. Therefore, low body mass index should not be used as a sign of frailty.
Limitations
There are several limitations to the present study. Sample size was not large enough to assess association of frailty with mortality and morbidities as isolated endpoints. Therefore, a composite endpoint was chosen. Due to observational design, albumin data was missing in 30 participants. This did not cause a concern regarding statistical power, however, resulted in a reduction in sample size during creation of combined diagnostic models. Despite consecutive sampling, EuroSCORE II of the patient cohort was on the lower spectrum. This might have created a spectrum bias and explain why EuroSCORE II had lower than expected predictive value. A limited number of frailty tools were investigated due to observational design and limited funding. Follow-up duration was short, so we were not able to evaluate the predictive value of frailty on long-term outcomes after cardiac surgery. Finally, patients undergoing TAVR were not included in the analysis.
CONCLUSION
Among frailty tests, serum albumin measurement had the highest predictive value for a composite of early postoperative mortality and morbidity in elderly patients undergoing elective cardiac surgery. Addition of albumin measurement as a frailty marker to EuroSCORE II cardiac surgical risk scoring system has the potential to improve EuroSCORE II’s ability to predict postoperative adverse outcomes. Further investigation with a larger sample from a wider spectrum of preoperative risk is warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Afilalo J Sharma A Zhang S Brennan JM Edwards FH Mack MJ Gait speed and 1-year mortality following cardiac surgery: a landmark analysis from the society of thoracic surgeons adult cardiac surgery database J Am Heart Assoc 2018723 e 01013910.1161/JAHA.118.01013930571598 PMC 6405557 · doi ↗ · pubmed ↗
- 2Afilalo J Steele R Manning WJ Khabbaz KR Rudski LG Langlois Y Derivation and validation of prognosis-based age cutoffs to define elderly in cardiac surgery Circ Cardiovasc Qual Outcomes 20169442443110.1161/CIRCOUTCOMES.115.00240927407052 · doi ↗ · pubmed ↗
- 3Nashef SA Roques F Sharples LD Nilsson J Smith C Goldstone AR Euro SCORE II Eur J Cardiothorac Surg 201241473474410.1093/ejcts/ezs 043discussion 744-522378855 · doi ↗ · pubmed ↗
- 4O'Brien SM Feng L He X Xian Y Jacobs JP Badhwar V The society of thoracic surgeons 2018 adult cardiac surgery risk models: part 2-statistical methods and results Ann Thorac Surg 201810551419142810.1016/j.athoracsur.2018.03.00329577924 · doi ↗ · pubmed ↗
- 5Fried LP Tangen CM Walston J Newman AB Hirsch C Gottdiener J Frailty in older adults: evidence for a phenotype J Gerontol A Biol Sci Med Sci 2001563 M 146M 15610.1093/gerona/56.3.m 14611253156 · doi ↗ · pubmed ↗
- 6Afilalo J Alexander KP Mack MJ Maurer MS Green P Allen LA Frailty assessment in the cardiovascular care of older adults J Am Coll Cardiol 201463874776210.1016/j.jacc.2013.09.07024291279 PMC 4571179 · doi ↗ · pubmed ↗
- 7Graham A Brown CH 4th Frailty, aging, and cardiovascular surgery Anesth Analg 201712441053106010.1213/ANE.000000000000156027622718 PMC 5675521 · doi ↗ · pubmed ↗
- 8Guralnik JM Ferrucci L Pieper CF Leveille SG Markides KS Ostir GV Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery J Gerontol A Biol Sci Med Sci 2000554 M 221M 23110.1093/gerona/55.4.m 22110811152 PMC 12149745 · doi ↗ · pubmed ↗