Post-traumatic pseudoaneurysm of the anterior tibial artery: therapeutic challenge
Poliana Mazuchini Belai, Zaira Cristina Barbosa Assis, Thiago Felipe de Moraes Vieira, Gislaine dos Santos Rodrigues Vieira, Henrique Alves de Almeida, Thiago Vaz Lopes, João da Silva, Vinicius Tadeu Ramos da Silva Grillo, Poliana Mazuchini Belai, Zaira Cristina Barbosa Assis

TL;DR
A rare case of a traumatic pseudoaneurysm in the anterior tibial artery is described, highlighting the importance of early diagnosis and surgical treatment.
Contribution
The paper presents a unique clinical case of a subacute traumatic pseudoaneurysm in the infrapatellar arteries and emphasizes the need for early detection.
Findings
A 25-year-old patient developed a pseudoaneurysm after a glass shard injury to the lower limb.
Venous Doppler ultrasound ruled out thrombosis but identified a pseudoaneurysm in the anterior tibial artery.
Surgical intervention with hematoma drainage and arterial suturing was successful.
Abstract
Subacute traumatic arterial pseudoaneurysms involving the infragenicular arteries are rarely discussed in the literature because they tend to be asymptomatic or manifest clinically subtle symptoms even at late stages. We describe the case of a 25-year-old patient with a perforation injury to the lower limb from a shard of glass, who, after two weeks, developed pain and swelling in the limb, which suggested deep vein thrombosis. Venous Doppler ultrasound ruled out thrombosis but revealed heterogeneous echogenicity in the anterior wall of the middle third of the anterior tibial artery with internal flow, suggesting a pseudoaneurysm. We opted for conventional surgical treatment and, after proximal and distal control of the artery, drainage of the local hematoma and primary suturing of the lesion were performed. Pseudoaneurysm of the infrapatellar arteries, although rare, is a challenging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
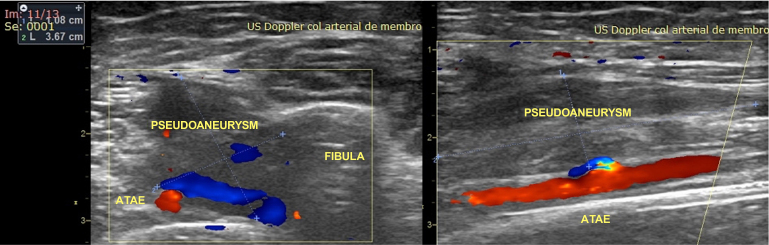 Figure 1
Figure 1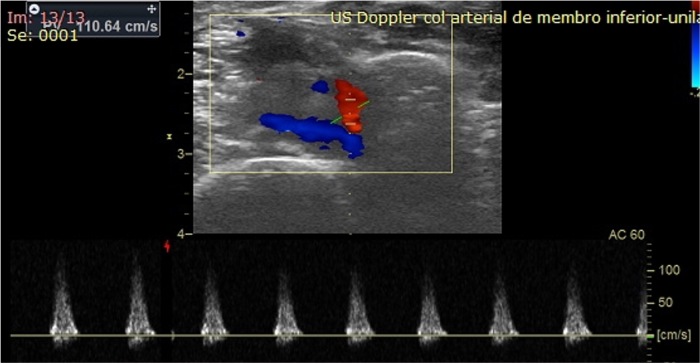 Figure 2
Figure 2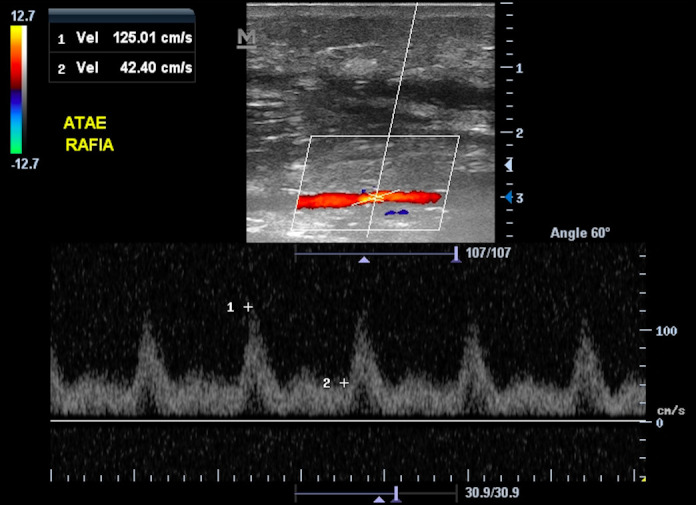 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Aortic aneurysm repair treatments · Vascular anomalies and interventions
INTRODUCTION
Pseudoaneurysms can originate in any artery in the human body. In the lower limbs, the popliteal artery is most commonly affected, followed by the superficial femoral artery and the anterior tibial artery (ATA). The ATA is the blood vessel most frequently associated with infrapatellar pseudoaneurysm, although its incidence is relatively rare.^1-3^
Pseudoaneurysms of the ATA are uncommon events that arise due to various iatrogenic causes or to blunt or penetrating trauma. Despite their rarity, these injuries are associated with significant morbidity, often posing a threat to limb integrity.^1,2,4,5^
The interval between the initial injury and the appearance of the pseudoaneurysm can vary from hours to years, depending on the location, size, and clinical manifestations. A high index of clinical suspicion is essential for accurate diagnosis of vascular injuries. Warning signs include the development of a progressive pulsatile mass, unexplained edema, and the absence of a palpable distal pulse. Differential diagnosis should include abscesses, hematomas, and neoplasms. Complications can range from severe pain, distal arterial embolism, and rupture and hemorrhage of the pseudoaneurysm to ulcer formation, which could culminate in amputation.^2,4^
Doppler ultrasonography has become the preferred imaging modality for the initial evaluation and diagnosis of pseudoaneurysms in this body region due to its high sensitivity and specificity, which range from 90-100% and 99-100%, respectively. The hallmark of pseudoaneurysms is an extraluminal blood flow pattern with variable echogenicity, a “yin-yang” mosaic sign, and turbulent systolic and diastolic blood flow, resulting in a “to-and-fro” Doppler waveform.^1,2,6,7^
PART I – CLINICAL SITUATION
We present the case of a 25-year-old female patient with leucoderma who had a perforation injury to her left lower limb from a piece of glass. The injury resulted in severe bleeding immediately after the glass was removed. In response to the emergency, an improvised tourniquet was applied at home, and the patient was taken to the hospital.
During initial care at the emergency room, no signs of active bleeding were observed, so a simple suture was made at the site of the injury and, after the procedure, the patient was discharged with a prescription for anti-inflammatory medication.
Two weeks after the initial injury, the skin lesion was healing satisfactorily and the suture was removed. However, pain and edema persisted in the left lower limb, which led to suspicion of deep vein thrombosis, and venous Doppler ultrasound of the limb was requested.
Deep vein thrombosis was ruled out by Doppler ultrasound, which was performed by a vascular surgeon. However, the analysis revealed heterogeneous echogenicity in the anterior wall of the middle third of the ATA, with dimensions of 1.83 cm × 1.56 cm in the anteroposterior and latero-lateral diameters, respectively (Figure 1). Color Doppler imaging showed high-resistance pulsatile flow within the pseudoaneurysm (Figure 2). It is important to emphasize that the distal segment of the anterior tibial artery and the other infragenicular arteries remained patent, exhibiting normal flow patterns.
Color Doppler ultrasonography showing pseudoaneurysm of the anterior tibial artery. Left: transverse view showing a 1.08 cm × 3.67 cm pseudoaneurysm of the left anterior tibial artery (ATAE in the image). Right: longitudinal view showing the pseudoaneurysm and the solution of continuity in the anterior wall of the left anterior tibial artery, with aliasing at the site.
Color Doppler ultrasound showing high-resistance pulsatile flow within the pseudoaneurysm of the anterior tibial artery.
PART II – TREATMENT
Conventional surgery was the selected course of action. After administration of antibiotic prophylaxis with first-generation cephalosporin, the patient underwent spinal anesthesia with sedation. The precise site of the arterial injury was marked on the skin with the aid of Doppler ultrasound. A longitudinal incision was made along a predetermined path in the middle third of the leg. After proximal and distal control of the ATA and ligation of one of the anterior tibial veins, the site of the pseudoaneurysm was approached. The local hematoma was drained and, when a penetrating injury to the ATA was identified, a primary suture was made with 6-0 polypropylene monofilament.
On the first postoperative day, the patient’s general condition was good and she was discharged from hospital, with symptomatic medications and physical therapy prescribed. The patient was reassessed 3 months after discharge, presenting cutaneous hypoesthesia at the surgical site, while ultrasound showed that the ATA was patent (Figure 3).
Color Doppler ultrasound performed 3 months after surgery, showing preserved flow in the left anterior tibial artery at the suture site.
DISCUSSION
Arterial pseudoaneurysms resulting from lower limb trauma are rarely addressed in the literature because they tend to be asymptomatic or present with subtle clinical symptoms in late stages. However, the need for early diagnosis is imperative, given their potentially catastrophic complications.^8^
Penetrating injuries to the vessels are often severe, presenting bleeding, expanding hematoma, pulse deficit, or bruit, which allow immediate diagnosis. A lack of such signs often results in delayed diagnosis of vascular complications.^9^ In the present case, despite severe bleeding at the time of the injury, the initial emergency room evaluation did not reveal other significant signs or symptoms, which impeded early diagnosis.
It is important to note that, after 2 weeks, the patient was referred for Doppler ultrasound due to pain and edema in the limb, with deep vein thrombosis initially suspected. However, additional analysis of the arterial system revealed that it was a pseudoaneurysm of the ATA. Differential diagnoses of a pseudoaneurysm include deep vein thrombosis, hematoma, arteriovenous fistula, and soft tissue or bone tumors. The importance of imaging tests in such cases should be emphasized, not only to rule out other causes, but to accurately confirm a diagnosis of pseudoaneurysm.^2^
Persistent pain and swelling in the affected limb should raise suspicion of a pseudoaneurysm or arteriovenous fistula. These lesions, which are often progressive, can cause ongoing discomfort and compress adjacent nerves or tendons. It is critical for emergency physicians to promptly identify and initiate treatment for this potentially limb-threatening condition, which is easily achievable through point-of-care ultrasound, which has become an essential tool in emergency medicine.^6,9^
Therapeutic planning is usually based on the size of the vessel, the imaging characteristics, and the presence or absence of collateral flow in the region of the affected vessel, as well as the hemodynamic stability of the patient and the anatomy of the pseudoaneurysm.^1-3^
Standard pseudoaneurysm treatment includes surgical interventions such as arterial ligation, direct suture, and vein grafting. However, significant challenges to adequate vascular control can occur in such approaches, especially in complex situations involving extensive dissection and tissue distortion due to the pseudoaneurysm.^5,10^
In the present case, considering the patency of the other infrapatellar arteries, surgical ligation could have been performed. However, due to the limited extent of the lesion, primary suturing was selected to preserve the vascular patency of the ATA.
Several therapeutic alternatives, conservative and interventional, surgical and endovascular, have been reported in the literature. These include ultrasound-guided compression, thrombin injection, coil embolization, and stent implantation.^5,10^ The ideal therapeutic approach depends on the specific characteristics of each case, requiring careful evaluation to ensure the effectiveness and safety of the treatment.
Zhou et al.^4^ point out that not all treatment types are equally suitable for infrapopliteal pseudoaneurysms, considering the reduced diameter of the arteries in this region and their deep location. Open surgery in this location is invasive, while ultrasound-guided compression and isolated thrombin injection may not achieve a complete seal. Recent advances and endovascular technologies have shown promise for treating post-traumatic arterial injuries and pseudoaneurysms.
According to a review of case reports, 41% of infrapopliteal pseudoaneurysms were treated with ligation, 24% with endovascular embolization, 10% with direct arterial repair, 10% with covered stent, 4% with venous interposition repair, 4% with ultrasound-guided thrombin injection, 4% resolved spontaneously, and 2% were treated with ultrasound-guided compression.^9^
CONCLUSIONS
Pseudoaneurysm of the ATA, although rare, is a challenging clinical entity that requires early diagnosis and an effective therapeutic approach. Integrating clinical evaluation, advanced imaging tests, such as ultrasound, and a comprehensive understanding of therapeutic options are essential for the effective management of these cases. The diversity of therapeutic approaches reported in the literature reflects the complexity of decision-making for this condition, emphasizing the importance of a personalized approach based on the vascular anatomy, the extent of the lesion, and the patient’s clinical conditions.
This study was duly evaluated and approved by the research ethics committee of the involved institution (certificate 78273124.5.0000.5297; decision number 6.707.252).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kalapatapu VR Shelton KR Ali AT Moursi MM Eidt JF Pseudoaneurysm: a review Curr Treat Options Cardiovasc Med 200810217318310.1007/s 11936-008-0019-818325320 · doi ↗ · pubmed ↗
- 2Nair N Suhania M Anterior tibial artery pseudoaneurysm Med J Malaysia 202176342943134031347 · pubmed ↗
- 3Salahuddin S Janardhanan S Krishnakumar KS Mattummal S Traumatic pseudoaneurysm of anterior tibial artery treated by thrombin injection Heart Views 2021221687010.4103/HEARTVIEWS.HEARTVIEWS_177_2034276893 PMC 8254162 · doi ↗ · pubmed ↗
- 4Zhou X Qiu CY Li DL Zhang HK Treatment of posttraumatic infrapopliteal pseudoaneurysm with a physician-modified covered stent Vasc Investig Ther 202143959710.4103/2589-9686.325189 · doi ↗
- 5Brunoro M Baldassarre V Sirignano P Mansour W Capoccia L Speziale F Endovascular treatment of an anterior tibial artery pseudoaneurysm secondary to penetrating trauma in a young patient: case report and literature review Ann Vasc Surg 201960479.e 5910.1016/j.avsg.2019.03.00531195105 · doi ↗ · pubmed ↗
- 6Thomas A Han GR Soh I Komara J Traumatic anterior tibial artery pseudoaneurysm: a case report Clin Pract Cases Emerg Med 20237425325610.5811/CPCEM.145838353196 PMC 10855291 · doi ↗ · pubmed ↗
- 7Mahmoud MZ Al-Saadi M Abuderman A et al “To-and-fro” waveform in the diagnosis of arterial pseudoaneurysms World J Radiol 201575899910.4329/wjr.v 7.i 5.8926029351 PMC 4444605 · doi ↗ · pubmed ↗
- 8Aslanidi C Athanasiou S Charalampous C et al Endovascular treatment of a post-traumatic pseudoaneurysm arising from a ruptured posterior tibial artery with Menox: a case report Radiol Case Rep 202116113231323610.1016/j.radcr.2021.07.05734484525 PMC 8405942 · doi ↗ · pubmed ↗